
Abstract
Critiques of the ‘naïve rationalist’ model of policy-making abound in the sociological and political science literature. Yet academic debate on health care policy-making continues to be couched in the dominant discourse of evidence-based medicine, whose underlying assumptions - that policies are driven by facts rather than values and these can be clearly separated; that ‘evidence’ is context-free, can be objectively weighed up and placed unproblematically in a ‘hierarchy’; and that policy-making is essentially an exercise in decision science - have constrained both thinking and practice. In this paper, drawing on theoretical work from political science and philosophy, and innovative empirical work in the health care sector, we argue that health care is well overdue for a re-defining of what policy-making is.
Policy-making is the formal struggle over ideas and values, played out by the rhetorical use of language and the enactment of social situations. While the selection, evaluation and implementation of research evidence are important in the policy-making process, they do not equate to that process. The study of argument in the construction of policy has the potential to illuminate dimensions of the process that are systematically occluded when policy-making is studied through a naïve rationalist lens. In particular, a rhetorical perspective highlights the struggle over ideas, the ‘naming and framing’ of policy problems, the centrality of audience and the rhetorical use of language in discussion to increase the audience's adherence to particular framings and proposals. Rhetorical theory requires us to redefine what counts as ‘rationality’ - which must extend from what is provably true (by logic) and probably true (by Bayesian reasoning) to embrace, in addition, that which is plausibly true (i.e. can convince a reasonable audience).
Future research into health care policy-making needs to move beyond the study of ‘getting evidence into practice’ and address the language, arguments and discourse through which policy is constructed and enacted.
Limitations of naïve rationalism as a framework for policy-making
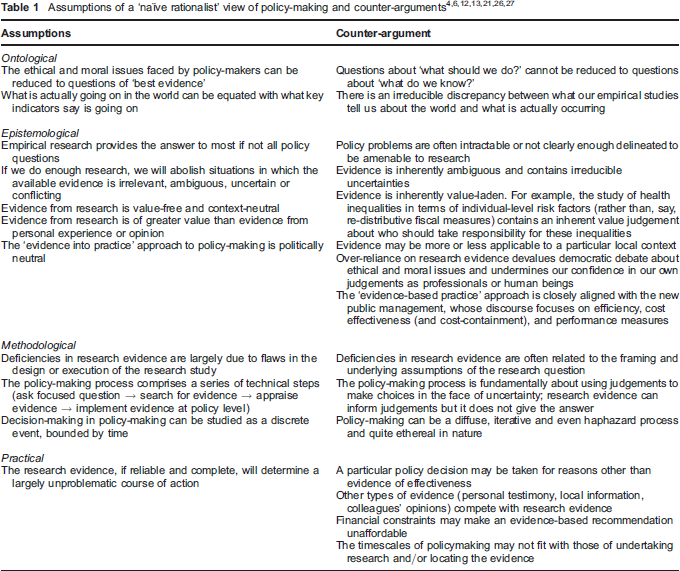
A straw poll of the titles of journal articles listed on the Medline database - such as ‘Translating evidence into practice’ and ‘Bridging the know-do gap’ - illustrates the conceptual cul-de-sac into which the evidence-based medicine movement has driven the study of health care policy-making. The idea that policy-making is all about finding and implementing best research evidence, and that the answer to improving policy-making is to identify and overcome barriers to smooth flow of best evidence into practice is taken as given by many influential medical opinion leaders1,2 and persists as the default expectation of both researchers and policy-makers in health care. Drawing on the work of philosopher Paul Feyerabend, we characterize this perspective as ‘naïve rationalism’. 3 The appeal and influence of this perspective endures despite significant critical analyses from social and political scientists over the past two decades,4–6 that have drawn attention to the limitations of naïve rationalism (Table 1).
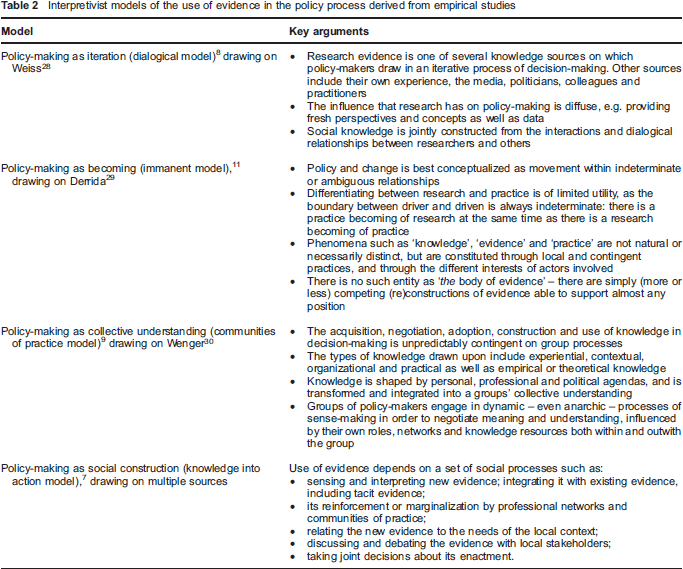
These analyses and recent empirical studies into the use of evidence in health policy settings7–11 have highlighted a far more complex relationship between evidence and policy (Table 2). Taken together, a rich picture emerges of policy-making as a communicative process of sense-making, embedded within specific political and institutional structures, and influenced by the interaction of individual and collective values, in which research evidence plays an important but only one part alongside other types of evidence, and rather than being ‘put into practice’ is dynamically constructed through local and contingent practices.
Interpretivist models of the use of evidence in the policy process derived from empirical studies
A necessary question, given these illuminating contributions to our understanding of the policy process, is why so much mainstream health policy discourse (for example, official policy documents, the work of the National Institute for Health and Clinical Excellence and the majority of academic papers published on evidence-based policy) continues to be indexed to the general logic of naïve rationalism. One reason is that the empirical research from which the perspectives shown in Table 2 are derived is made up of study designs (ethnography and qualitative interviews) that rank low in evidence-based medicine's traditional ‘hierarchy of evidence’. Furthermore, the prevailing political climate in UK health policy (and national policy-making more widely) is dominated by the discourse of modernism, in which good practice is equated with finding out ‘what works’, implementing it efficiently and cost effectively, and measuring progress in terms of key outcome indicators. It is suggested that this ‘utilitarian turn’ in the perceived role of research has led to the further entrenchment of naïve rationalist conceptions of the policy process. 13 By bringing together the normative goals of policy-making with those of new public management, the UK government's modernization project has successfully de-politicized and managerialized knowledge production and its utilization.12,13
The various models of policy-making outlined in Table 2, whose conceptual commonalities are far greater than their differences, all focus on the dynamics of social interaction and take the group in its social context as their unit of analysis. This emerging (but still marginal) research tradition in health care has begun to highlight how policy-making in practice depends crucially on what is said, by whom, and on whether others find their arguments persuasive. If we wish to study policy-making ‘as is’ rather than as the naïve rationalists believe it should be, then we require a framework of ideas that addresses the role of language, argument and discourse. Argumentation theory, and specifically rhetoric, is ideally suited to this purpose.
Argumentation theory and the contested place of rhetoric
The academic study of argumentation (that is, of reasoning and persuasion) is an interdisciplinary field, attracting attention from philosophers, logicians, linguists, legal scholars, political scientists and sociologists. The foundations of argumentation theory were laid by Aristotle, who defined three dimensions of scholarship – analytic (logical argument using premises based on certain knowledge) dialectic (debating to argue for and against a standpoint) and rhetoric (the use of persuasion to influence the thought and behaviour of one's audience). 14
Prior to the Enlightenment, rhetoric was the dominant element in most claims to scholarship. Aristotle taught his students to augment their use of logic in argument with rhetorical devices (metaphor, irony and so on) and by gaining the audience's trust by various appeals to credibility. But with the rise of modern science, ‘demonstration’ (formal logic) superseded other methods of inquiry as a way of explaining the world, and dialectic and rhetoric were pushed to the background. Rhetoric in particular was consigned to the margins of legitimate scholarship and came to be construed in a pejorative sense as ‘spin’ or ‘bias’ that would, if not systematically expurgated, detract from the reasoning process.
In recent years, there has been a resurgence of interest in the study of rhetoric in academic inquiry. 15 Carolyn Miller's work suggests that rhetoric is a skill that makes the creation and change of belief through symbolic exchange both the goal and the means of making decisions. 16 In this sense, rhetorical argument encourages reasoned moral political discourse.17,18
Rhetorical skills are often used to introduce research evidence in the policy-making process, as in:
‘Members of the committee, last week I attended the funeral of one of my patients, a single parent who died of breast cancer at the age of 32, leaving four young children. The latest research evidence from the paper I have circulated suggests that had she received drug X at diagnosis, her five-year survival would have been 70% instead of 30%. I urge you, therefore, to consider funding drug X.’
Note that in this fictitious example, the research evidence is not deliberately distorted by the arguer, in that the survival figures derived from the research paper are (let's assume) correct. But the importance of this evidence, and the weight it is likely to carry in the policy-making process, have been bolstered by the use of rhetorical devices: powerful imagery and a claim to credibility. Assuming that all players understand the evidence, the argument around this particular policy-making table will probably be driven by equally rhetorical counter-narratives of other ‘deserving causes’ that are competing for the same limited funding pot. Fundamental to rhetorical inquiry is the notion that facts and values are not cleanly separable, and that values are not fixed but emergent and negotiable.
How rhetoric can add value in policy-making research
Drawing partly on Miller's characterization of the differences between a scientistic and rhetorical approach to decision-making, 16 we identify five salient features of rhetoric in the study of policy-making to suggest ways in which a rhetorical perspective can enrich rather than compromise the analysis of health care policy.
Rhetoric highlights the struggle over ideas
The naïve rationalist approach to evidence-based policy often implies (and occasionally states overtly) that ‘what to do’ will be self-evident once enough high quality research evidence of ‘what works’ has accrued. Political scientists would disagree, since politics (and therefore much of policy-making) has at its heart the contestation between different world views:
‘The essence of policy-making in political communities [is] the struggle over ideas. Ideas are at the centre of all political conflict … Each idea is an argument, or more accurately, a collection of arguments in favour of different ways of seeing the world.’ 6
A rhetorical perspective allows us to analyse not merely how policy-makers solve problems but also how they formulate and prioritize those problems in the first place – and conversely, how certain issues come to be defined as ‘non-problems’, or simply not seen at all. Viewed as argument, policy-making represents a constant discursive struggle over the ‘naming and framing’ of problems, the boundaries of problem categories, and the definitions and negotiations of ideas that guide the ways people create the shared meanings which motivate them to act.6,19,20
Rhetoric confronts uncertainty in policy-making
Much conventional thinking about evidence-based policy construes uncertainty in terms of an ‘evidence gap’. The assumption is that more and better evidence, implemented with more commitment and skill from practitioners, will eventually abolish uncertainty. By contrast, Aristotle believed that uncertainty in the policy arena generally concerns questions not of ‘what do we know?’ (problems of evidence) but of ‘what should we do?’ (problems of action). Naïve rationalism's error has been to reduce the latter to the former. The example in Figure 1 highlights how an analysis of values and reasoning can expose fundamental problems of action that are essentially contestable and cannot be solved simply by recourse to evidence.
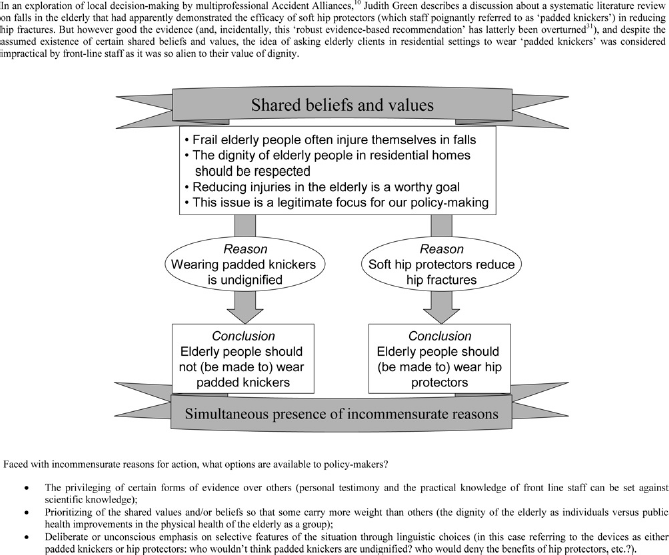
Problems of action
Miller argues that the task in solving a problem of action is not to acquire more information, but to exercise practical reason. 16 Practical reason involves persuasion, reflection upon values, prudential judgement and free disclosure of one's ideas. 21 The strength of a rhetorical analysis is that it allows us to expose and study precisely these processes of practical reasoning.
Policy deliberation depends fundamentally on human judgement; its success rests on criticism and debate rather than procedural correctness. Rhetoric has even been presented as a theory of human choice, 17 fundamental to freedom itself. 22 This anchoring of policy-making in philosophical truths about what it means to be free contrasts starkly with naïve rationalism, which fails to recognize the need for deliberation about what we ought to do or be, and thus does not accommodate the possibility of choice based on the consideration of competing values.
Arguments are constructed for particular audiences
To Aristotle, the art of persuading an audience comprised three elements: logos – the argument itself; pathos – appeals to emotions (which might include beliefs, values, knowledge and imagination); and ethos – the credibility, legitimacy and authority that a speaker brings and develops over the course of the argument. 23 A rhetorical perspective, therefore, requires us to move away from any sense of disembodied evidence, towards not only how evidence is constructed, but also by whom (and for whom) it is constructed, how the evidence and the speaker are received, and the meaning the evidence holds for its audience. In short, different audiences will be persuaded by different sorts of appeal.
A landmark publication in modern argumentation theory was The New Rhetoric which outlines how discursive techniques can be used to increase the adherence of an audience to ideas that are presented to it. 22 Spoken (and, to a lesser extent, written) argument develops in terms of the audience's (anticipated) reaction, and the quality of an argument might be judged in terms of whether the audience is indeed persuaded by it. In The New Rhetoric, the authors analyse the ways in which argumentation moves in a debate develop (or fail to develop) the intensity of an audience's adherence to a particular viewpoint. Because of the opinions and beliefs they hold (and the values underlying them), the audience creates a context in which certain premises hold. To decide on the best argument, the arguer has to put him/herself into the audience's shoes and consider what Perelman and Olbrechts-Tyteca 22 call their ‘points of departure’. In the fictitious example quoted above, the GP speaker might have deliberately chosen to talk about orphaned children because she knew that key decision-makers on the committee were the parents or grandparents of small children. Had this not been the case, a different choice of words might have had greater rhetorical weight. A committee made up entirely of childless finance managers, for example, might have been more easily persuaded by an argument couched in terms of the cost to society of placing four children in care.
Rhetoric extends the realm of the rational
Naïve rationalism restricts the ‘evidence’ for policy-making to analytic deductions of the general form ‘if-X- then-necessarily-Y’ and Bayesian probabilities of the general form ‘if-X-then-probably-Y’. A rhetorical perspective embraces not only these forms of rationality, but also the upstream ‘naming and framing’ that defines what is important and what is valuable in a particular group or society, which in turn requires democratic debate about the ethical and moral worth of alternative courses of action.
If we accept the ontological premises that facts are always value-laden and judgements context-dependent, it follows that the practical reasoning necessary for the reduction of uncertainty discussed above (what Aristotle called phronesis) is a reasonable and legitimate form of ‘evidence’ – indeed, that it may be the most important form of evidence needed in the messy, context-bound business of policy-making. But the elevation of phronesis to the status of rational is a direct affront to the evidence-based policy movement's fixation with framing evidence around episteme (theoretical knowledge) and techne (instrumental knowledge). 13 This is the crux of the incommensurability between the ‘science’ and the ‘art’ of policy-making: if we accept a broader definition of what is rational (Box 1) to include that which is considered plausibly true, the pursuit of ‘evidence-based policy’ has led not to more rational decision-making but, as Schwandt suggests, to a devaluation of the intellectual virtue of phronesis, and a deadening of moral sensibilities, as we increasingly concede the task of decision-making to the expertise of science. 21
Three conceptualizations of what is ‘rational’
Rationality is concerned with:
what is provably true (the evidence of logico-deductive reasoning);
what is probably true (the evidence of Bayesian reasoning);
what is plausibly true (the evidence of arguments that are sincere and will convince a reasonable audience).
Rhetorical analysis can reveal wider social practices and ideologies
Argumentation theory's focus on the detail of linguistic exchanges may give the impression that this sort of analysis is primarily confined to the study of micro-level interaction, and could be seen to run the risk of reducing policy-making to specific instances and definitive moments of argument. But this is far from the case, since the language and rhetorical devices used in policy arguments serve as a window to the wider social practices that support the saying of particular things in particular ways. For example, what a speaker actually says carries implicit assumptions about what can be left unsaid (because everyone is assumed to be agreed on it). By identifying rhetorical appeals to what Perelman and Olbrecthts-Tyteca 22 call the ‘universal audience’, we can gain insights about the societal ideologies and values shared by such an audience (though not, of course, held to the same extent by each of its members). 24 The fictitious speaker arguing above for funding an expensive breast cancer drug is taking as given that (a) it is the State's responsibility to fund medical treatment for the individual (there is no suggestion, for example, that the woman ought to have been privately insured); (b) the availability of an effective drug creates some obligation to fund it, whatever the cost; and (c) the lives of young adults, especially parents, are worth more than the lives of older people.
The study of political and ideological ‘drivers’ for policy-making through the analysis of the rhetorical moves made in decision-making situations is a specific example of the way in which the broad field of discourse analysis ‘examines how language constructs phenomena, not how it reflects and reveals it’ [sic] 25 and enables the researcher to explore connections between arguments, wider discourses and social contexts.
Conclusion
Over the past few decades the field of policy studies has experienced an important shift away from what Stone describes as the ‘rationality project’, 6 towards postpositivist approaches that define policy-making as the formal struggle over ideas and values. Yet, disappointingly, the fruitful ideas emerging from this ‘argumentative turn’ 5 in policy studies have been little explored by UK health policy researchers, whose work in the main continues to be indexed to the general logic of evidence-based medicine. In this paper we have argued that there is much to be gained from exploring health care policy-making from a rhetorical perspective (Box 2). The study of argument has the potential to illuminate dimensions of the policy process that remain hidden when policy-making is studied through a naïve rationalist lens, enabling a rich description of policy-making as is rather than as researchers believe it ought to be. Acknowledging that in the messy world of policy-making there is no single ‘right answer’, only more-or-less good reasons to arrive at more-or-less plausible conclusions, rhetorical theory directs analysis towards the human processes of judgement and justification, and thus supports critical inquiry into how evidence is constructed.
What can policy analysts and policy-makers gain from understanding policy-making as argumenative processes?
A rich description of the naturalistic processes occurring around the policy-making table
Recognition of the legitimacy of different perspectives leading to greater understanding of others’ positions
Emphasis on processes of judgement and justification, rather than simply the decision-making outcome
Ability to probe assumptions critically, appreciate and be able to justify value judgements
More sophisticated understanding of the audience (appeal to audience through choice of arguments likely to gain adherence)
Alternative framings → ‘pushing out the boundaries of the possible’ → more creative thinking to solve complex problems
The benefits of a rhetorical perspective are not limited to academic inquiry. Making visible the role of language, argument and discourse in policy discussions has the potential to play an emancipatory role in giving policy-makers new insights into their work, and increasing awareness of the conditions that shape their actions and choices. Rein and Schon have proposed that if the essence of policy-making is argument about the best course of action, a key to achieving this task effectively is the development of a critical awareness of the rhetorical use of language by oneself and others – a state they have called ‘frame reflective awareness’. 20 Awareness of our ‘frames’ (that is, the conceptual and perceptual lenses through which we view the world) can help expose the system of values, preferences and beliefs from which we (and our opponents) are arguing; how we (and they) construct and position potential audiences; and even how we formulate and construct what ‘the problem’ is taken to be. This increased awareness opens up the possibility for alternative framings, and thus opportunities for policymakers to engage in creative thinking to solve the complex problems they face.
The first step in achieving frame reflective awareness is to recognize that ‘naming and framing’ and the struggle over ideas goes on at all. As Table 1 illustrates, this recognition requires the naïve rationalist to cross a huge ontological divide: he or she must accept the socially constructed (and hence fluid and contestable) nature of truth. Few health care policy-makers, steeped in the dominant culture of evidence-based medicine, will find this easy. The suggestion that they should include within the realm of the rational choices that are irreducibly subjective is seen by many as a regressive step into a pre-Enlightenment world of biased, illogical and unreliable decisions. Feyerabend articulates the fears of such people:
‘… the longing for a world in which one need not make fundamental decisions but can always count on advice, has made rationalists act like frightened children. “What shall we do?”, “How shall we choose?”, they cry when presented with a set of alternatives, assuming that the choice is not their own, but must be decided by standards that are a) explicit and b) not themselves subjected to a choice.’ 3
Feyerabend has the following response to such questions: ‘You are grown up now, children, and so you have to find your own way’. 3 Our modest contribution in this paper is to suggest that a greater awareness of rhetoric and an understanding of policy-making as an argumentative process has a small but important part to play in developing the sort of critical intelligence that can empower decision-makers to ‘find their own way’.
In conclusion, in this paper we have argued that it is time to problematize the notion of ‘evidence’ in the health care policy-making process and to legitimize rather than devalue the place of practical judgement (phronesis). We have also highlighted the dearth of theory-driven empirical studies to date that have explored the rhetorical process by which health care policy is constructed. Our own team is currently engaged in one such study, exploring decision-making about resource allocation at a local level in primary care, and we hope to report empirical findings shortly.
Footnotes
Acknowledgements
This work was part funded by a grant from the Leverhulme Trust to explore cross-disciplinary issues in the nature of evidence at University College London (see ![]() ). We are grateful to fellow researchers on that interdisciplinary project for numerous discussions and seminars that helped formulate the ideas presented in this paper.
). We are grateful to fellow researchers on that interdisciplinary project for numerous discussions and seminars that helped formulate the ideas presented in this paper.