
Abstract
Objective
To use evidence from research to identify and implement priority setting and resource allocation that incorporates both ethical practices and economic principles.
Method
Program budgeting and marginal analysis (PBMA) is based on two key economic principles: opportunity cost (i.e. doing one thing instead of another) and the margin (i.e. resource allocation should result in maximum benefit for available resources). An ethical framework for priority setting and resource allocation known as Accountability for Reasonableness (A4R) focuses on making sure that resource allocations are based on a fair decisionmaking process. It includes the following four conditions: publicity; relevance; appeals; and enforcement. More recent literature on the topic suggests that a fifth condition, that of empowerment, should be added to the Framework. The 2007-08 operating budget for Home and Community Care, excluding the residential sector, was developed using PBMA and incorporating the A4R conditions.
Results
Recommendations developed using PBMA were forwarded to the Executive Committee, approved and implemented for the 2007-08 fiscal year operating budget. In addition there were two projects approved for approximately $200,000.
Conclusion
PBMA is an improvement over previous practice. Managers of Home and Community Care are committed to using the process for the 2008-09 fiscal year operating budget and expanding its use to include mental health and addictions services. In addition, managers of public health prevention and promotion services are considering using the process.
Introduction
Health authority decision-makers are challenged to provide publicly funded health services within a fixed budget. It is generally felt that the funding provided is not sufficient to meet all the demands for services. Therefore some method of priority setting and resource allocation is required. It has been common practice in health care to set priorities and subsequently allocate resources based on what has been done in the past. 1 This approach often included adjustments for inflation, wage increases and additional programs added or services expanded based on targeted funding or political agendas. Furthermore, this approach resulted in an ever-increasing budget with little or no onus on ensuring that the maximum benefit is being realized from the resources allocated.
The literature on priority setting and resource allocation in health care suggests that if we are to maximize health benefits with the resources available, there is a need to set priorities and allocate resources based on a systematic approach which explicitly considers both evidence and values. Viewed in this way, ethics as well as economics should be considered in priority setting and resource allocation. A framework known as program budgeting and marginal analysis (PBMA) has been used internationally to set priorities and allocate resources in health care.2–5 An ethical approach known as Accountability for Reasonableness (A4R) has also been used in health care.6–8 Instead of viewing ethics and economics as competing disciplines, the potential exists to combine these frameworks, resulting in a comprehensive approach to priority setting. 9
Our aim was to use PBMA in developing the annual operating budget for 2007–08 for Home and Community Care programs of the Northern Health Authority in British Columbia (BC). The objectives were to identify, develop and implement an ethical, evidence-driven approach to priority setting and resource allocation.
Method
Prior to this project, resource allocation had relied on historical allocations. From a practical perspective, it is important that decision-makers responsible for priority setting and resource allocation buy-in to a new approach if it is to be successful. As part of this, it was felt necessary to determine whether participants believed that the proposed approach would be a better method than that which was currently being used, and also to measure their satisfaction with the new approach after implementation.
Context
Northern Health (NH) is one of six health authorities in British Columbia. NH is responsible for delivering the full range of publicly funded health services to the population of northern BC. The population is approximately 300,000 and the geographic area is 598,000 square kilometers. The health authority is divided into three geographical Health Service Delivery Areas. The 2006–07 operating budget was approximately CAN$521 million (CAN$1 = US$0.93).
As the intervention project had to be completed within the two year EXTRA fellowship program it was decided to undertake a pilot implementation in one of the major programs within NH rather than attempt to apply the process at a macro level across all program areas. We aimed to introduce PBMA for development of the 2007–08 operating budget for Home and Community Care (HCC) Programs within NH. HCC was selected for three reasons. First, the InterRAI assessment tool had just been introduced into NH residential facilities and home support. This tool provides current data on the health status of clients receiving services from HCC. Second, the Ministry of Health in BC has a provincial initiative, mandated to be complete by 2008, that would increase residential beds by 5000 across the province (including 310 in Northern Health). The HCC programs were engaged in a re-design process that includes review of their current programs. Third, it was felt that by conducting a pilot project we could make an informed decision on whether we should apply the priority setting and resource allocation methodology at a macro level across all program areas within NH, or in other program areas.
PBMA
Program budgeting and marginal analysis is based on two key economic principles: opportunity cost (i.e. doing one thing instead of another) and the margin (i.e. resource allocation decisions should result in maximum benefit for available resources). 1 PBMA can be described by asking five questions pertaining to the use of resources. The first two questions relate to the program budget and the last three relate to marginal analysis.
What resources are available in total?
In what ways are these resources currently spent?
What are the main candidates for more resources and what would be their level of effectiveness?
Are there any areas of care which could be provided to the same level of effectiveness but with fewer resources, so releasing those resources to fund other services (i.e. technical efficiency)?
Are there areas of care which, despite being effective should receive fewer resources because other options are more effective per dollar spent (i.e. addressing allocative efficiency)?
Typically, there are seven stages used in priority setting using PBMA. 7 These, together with the approach we took are shown in Table 1. In order to assess proposals for investment and disinvestment, we developed a set of decision criteria through discussion with HCC stakeholders and further refinement based on examples in the literature. 8 In the end, the selected criteria were similar to criteria used in other PBMA exercises in Canada, including notions of health gain, access, appropriateness and organizational strategic alignment. Each service proposal was rated against the criteria resulting in overall benefit scores. We also attempted to introduce a notion of cost-effectiveness into the evaluation by deriving ‘cost-value’ ratios, by dividing the benefit scores by the program costs.
Seven stages of priority setting using PBMA and the approach adopted in Northern Health

Accountability for reasonableness
Accountability for reasonableness is an ethical approach to priority setting. The process includes four (or five) conditions that should be met during priority setting to ensure the decisions reached are legitimate and fair. These conditions are relevance, publicity, revisions and appeals, and enforcement. 10 It has been suggested that a fifth condition, that of empowerment, should also be considered. 8 A checklist for ethical conditions that should be present in priority setting 9 and comments on how we attempted to meet the conditions in HCC are shown in Table 2.
Checklist on conditions for ethical priority setting
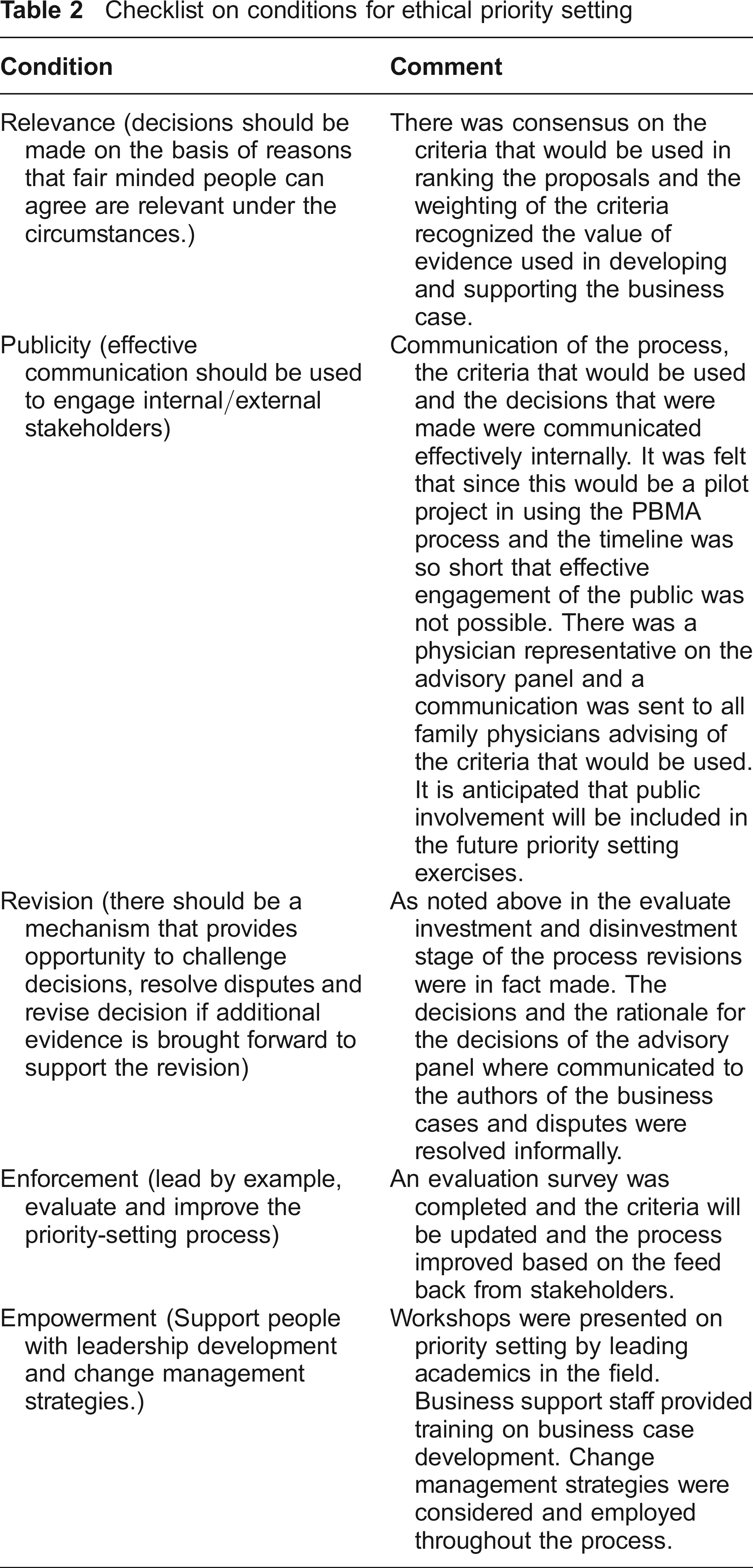
Not all of these ethical conditions were met entirely in our initial attempt to use PBMA. Over time, we plan to expand the use of PBMA and will continue to evaluate and refine our processes to better meet ethical conditions.
Results
A briefing note was prepared for the HCC Executive Team meeting held in October 2006. The briefing note outlined the process that had been used, key points, lessons learned, assumptions on which the recommendations were based and four recommendations on resource allocation for the 2007–08 HCC operating budget. The Executive approved all four recommendations, with the HCC preliminary operating budget for 2007–08 being increased by $79,513 (new and expanded programs of $232,672 and program reduction of $153,159). In addition, funding of $200,000 was provided to address two of the recommendations.
The ability to meet the established deadlines and to deliver on the major milestones had been identified as a significant risk in the project planning documents. The implementation of the project proceeded within the established timelines and all major milestones were delivered on schedule. This was accomplished through cooperation of all those involved in the project whose contribution was pivotal to the success of the project.
Discussion
Although the monetary impact of the recommendations was limited, the impact of the project on the culture of the organization was significant. The increase in managers' awareness of the potential benefits of using research evidence to support their business cases and the increase in knowledge of what makes up their departmental budgets were two examples of positive outcomes of the project. The HCC Executive's approval of the recommendations from the Advisory Panel could be considered to be a small but significant achievement in changing the culture of the organization from accepting of the status quo to willing to engage in change, in this case around implementation of a new approach to priority setting and resource allocation.
One of the desired outcomes was to increase the use of evidence-informed decisionmaking. The introduction of a systematic and values based approach to priority setting and resource allocation that was identified through review of research findings is evidence of that. Also the managers, in developing the business cases for consideration, increased their awareness and commitment to using evidence from research to support their requests for resource allocation. Discussions are currently underway within the organization to expand the use of the PBMA process to other portfolios. The mental health and addictions program is committed to using the process for development of their 2008–09 operating budget.
The introduction of a priority setting and resource allocation in health care that encompasses both economic and ethical principles is challenging but possible. PBMA, as applied in HCC, was based on multicriteria decision analysis. Baltussen & Niessen state:
‘Priority setting of health interventions is often ad hoc and resources are not used to an optimal extent. Underlying problem is that multiple criteria play a role and decisions are complex. Interventions may be chosen to maximize general population health, to reduce health inequalities of disadvantaged or vulnerable groups, and/or to respond to life-threatening situations, all with respect to practical and budgetary constraints … Therefore, the development of a multi-criteria approach to priority setting is necessary, and this has indeed recently been identified as one of the most important issues in health system research … We call for a shift away from present priority setting tools in health – that tend to focus on single criteria – towards transparent and systematic approaches that take into account all relevant criteria simultaneously.' 11
The demands on health care resources, both fiscal and human resources, is the most important challenge facing health care managers. The need to set priorities and allocate resources where the most benefit can be realized is critical to maintaining services. This is especially true in a publicly funded system such as in Canada.
Footnotes
Acknowledgements
The authors thank Cathy Ulrich, Northern Health for her support; Yvette Rutherford, Northern Health and Tammy Klassen, University of Northern British Columbia for comments on early drafts of this manuscript; and the EXTRA program of Canadian Health Services Research Foundation for the opportunity to undertake this project. Craig Mitton and Stuart Peacock are funded by the Michael Smith Foundation for Health Research. Craig Mitton also receives funding from the Canada Research Chairs Program.