
Abstract
Objectives
To examine attitudes to the Mental Capacity Act's new statutory Independent Mental Capacity Advocate (IMCA) service in England and Wales and consider the implications for its delivery.
Methods
Quantitative data describing all referrals to the seven pilot IMCA services (January 2006-March 2007) and qualitative data from semi-structured interviews with 18 doctors, 21 senior nurses and one discharge planning manager in four general hospitals in England.
Results
Of 127 hospital-based referrals to the seven pilot IMCA services, 29 (23%) were for patients facing serious medical treatments, 52% of whom were judged to lack decisionmaking capacity due to a learning disability; ninety-eight (77%) were for patients facing a change of accommodation upon hospital discharge, 62% of whom were elderly and lacked capacity due to dementia. While aware of the potential benefits of the IMCA service, clinicians were generally negative about the contribution advocates could make to patients’ medical care and thought they could only contribute usefully in a minority of ethically complicated decisions. In contrast, they were more positive about the involvement of advocates in hospital discharge decisions and hoped that they would improve current discharge practice.
Conclusions
Clinicians held ambivalent attitudes towards the involvement of a statutory IMCA service in medical decisions, reflecting beliefs that the service was largely impractical and unnecessary given current procedures for making medical decisions in patients’ ‘best interests’. Conversely, clinicians were more likely to support advocacy in discharge decisions because they believed that non-medically qualified advocates could make a valuable contribution to decisions that were seen as predominantly social and where practice was frequently considered deficient. By holding these beliefs, clinicians are failing to have due regard for the IMCA service as a statutory measure for safeguarding patients’ interests.
Introduction
Clinicians in England and Wales are under a new statutory obligation to have regard for the Mental Capacity Act 1 (MCA) and its Code of Practice. 2 Where patients are without relatives or friends and lack the mental capacity to make a decision about a serious medical treatment’ or a change of accommodation, clinicians must appoint an Independent Mental Capacity Advocate (IMCA). As part of an independent evaluation of the work of seven advocacy organizations involved in piloting the IMCA service, 3 we examined the attitudes of hospital clinicians to these new services in order to consider their implications for implementation.
The Mental Capacity Act 2005
The Act introduced a statutory framework in England and Wales to both empower and safeguard adults (aged 16 years or more) who, because of an ‘impairment of, or disturbance in the functioning of, the mind or brain’, are at risk of lacking capacity to make one or more decisions concerning their health, welfare or finances. It sets out procedures for judging whether a person lacks capacity to make a particular decision and it is a fundamental principle of the legislation that a person should only be judged to lack decisionmaking capacity when all ‘practicable steps’ to maximize his or her capacity have been taken without success. In situations where a person is judged to lack decisionmaking capacity, the person requiring the decision to be made (the ‘decision-maker’, often a clinician) can make a decision on the person's behalf, in his or her best interests’ (Box 1). However, when the decision relates to ‘serious medical treatment’ (Box 2) or a change of accommodation, and the person has neither relatives or friends who could be consulted about his or her wishes, nor has made any relevant legal arrangement, the decision-maker must appoint an IMCA.
Summary of the checklist for determining ‘best interests’ 2
Working out what is in someone's best interests cannot be based on their age, appearance, condition or behaviour
All relevant circumstances should be considered when working out someone's best interests
Every effort should be made to encourage and enable the person who lacks capacity to take part in making the decision
If there is a chance that the person will regain capacity to make a particular decision, then it may be possible to put off the decision until later if it is not urgent
Special considerations apply to decisions about life-sustaining treatment
The person's past and present wishes and feelings, beliefs and values should be taken into account
The views of people who are close to the person who lacks capacity should be considered, as well as the views of an attorney or deputy
Definition of ‘serious medical treatment’ 2
Serious medical treatment as defined as treatment which involves giving new treatment, stopping treatment that has already started or withholding treatment that could be offered in circumstances where:
if a single treatment is proposed there is a fine balance between the likely benefits and the burdens to the patient and the risks involved;
a decision between a choice of treatments is finely balanced;
what is proposed is likely to have serious consequences for the patient.
‘Serious consequences’ are those which could have a serious impact on the patient, either from the effects of the treatment itself or its wider implications
Advocacy and IMCA
Independent advocacy services have been developed by voluntary sector organizations over the past 25 years. In health care, their aim has been to ensure that patients are empowered to voice their views and needs to the practitioners making decisions about their lives. For people who are unable to express their views and needs clearly, due to mental disability, various forms of non-instructed advocacy have been developed. By developing long-term relationships with patients and/or questioning decision-makers from the patients’ perspectives, advocates seek to ensure equal treatment and access to services for these men and women and make certain that any decisions made have regard to their views and preferences. 4 All forms of advocacy, including non-instructed advocacy, are independent from both the clinician and the health care organization.
The value of independent advocacy has gained increasing recognition in government strategies in the UK for empowering and safeguarding the interests of vulnerable people.5-7 The IMCA service in the MCA is, however, the first statutory provision of advocacy in England and Wales. Like some models of non-instructed advocacy operating in the voluntary sector, the IMCA service offers decision-specific support and representation for people who lack decisionmaking capacity. However, in health care the IMCA service is restricted to decisions concerning either ‘serious medical treatment’ or change of accommodation. 8 Furthermore, the IMCA service specifically aims to ensure that the procedures for determining ‘best interests’ are followed. In contrast with legislation in other jurisdictions, such as Scotland and Canada,9,10 the MCA (with its provisions for the IMCA service) specifies not only who can make decisions on behalf of an adult lacking decisionmaking capacity but how they are to make that decision in the ‘best interests’ of the person concerned.
Methods
Quantitative data were collected describing all referrals to the seven organizations involved in providing the pilot IMCA services (January 2006-March 2007) which covered 20 general hospitals in England. Qualitative data were collected by semi-structured interviews with doctors and senior nurses in four of these hospitals. Four large general hospitals were selected with access to one of three pilot IMCA services, and within three hours travelling distance from the research team. The hospitals’ medical directors were asked to provide names of clinicians who were: in a medical specialty in which patients at risk of lacking decisionmaking capacity were likely to be treated; involved in discharge planning that might require a change of accommodation; or responsible for hospital-wide implementation of the MCA. Consenting clinicians were interviewed face-to-face or by phone. The interviews included both general questions, relating to the involvement of advocacy in serious medical treatment decisions and discharge decisions, the likely demand for the service and the roles of each of the groups of participants. The interviews enabled respondents to express their understanding and experience of the IMCA service. Notes were taken during the interviews, with key phrases preserved verbatim.
The interviews were examined in Atlas ti for content, 11 with emergent themes identified. These themes were refined and validated as codes in data workshops with members of the research team not involved in data collection. An initial period of data analysis was followed by two participant validation exercises: 12 one involving hospital doctors and advocates involved in the pilot services; the other involving clinicians in an MCA training workshop. Discussions at these meetings were used to assess the reliability of our interpretation and to guide subsequent data analysis. Our analysis focused on concerns over, and arguments for and against, the introduction of the IMCA service. While we consider our analysis to have captured the range of different opinions in our sample, we have little idea how representative these views are of clinical opinion generally.
Results
Profile of patients referred to the IMCA services
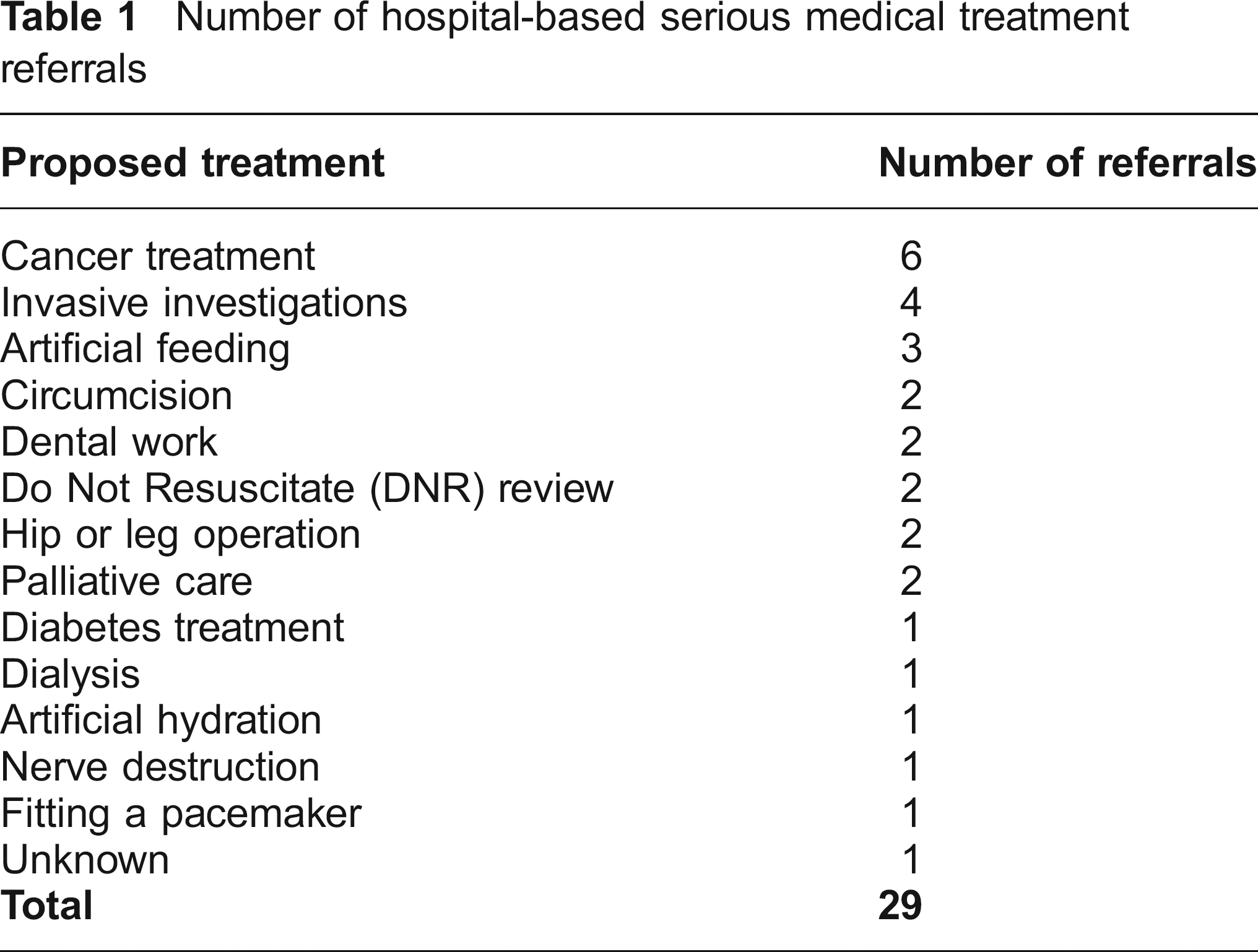
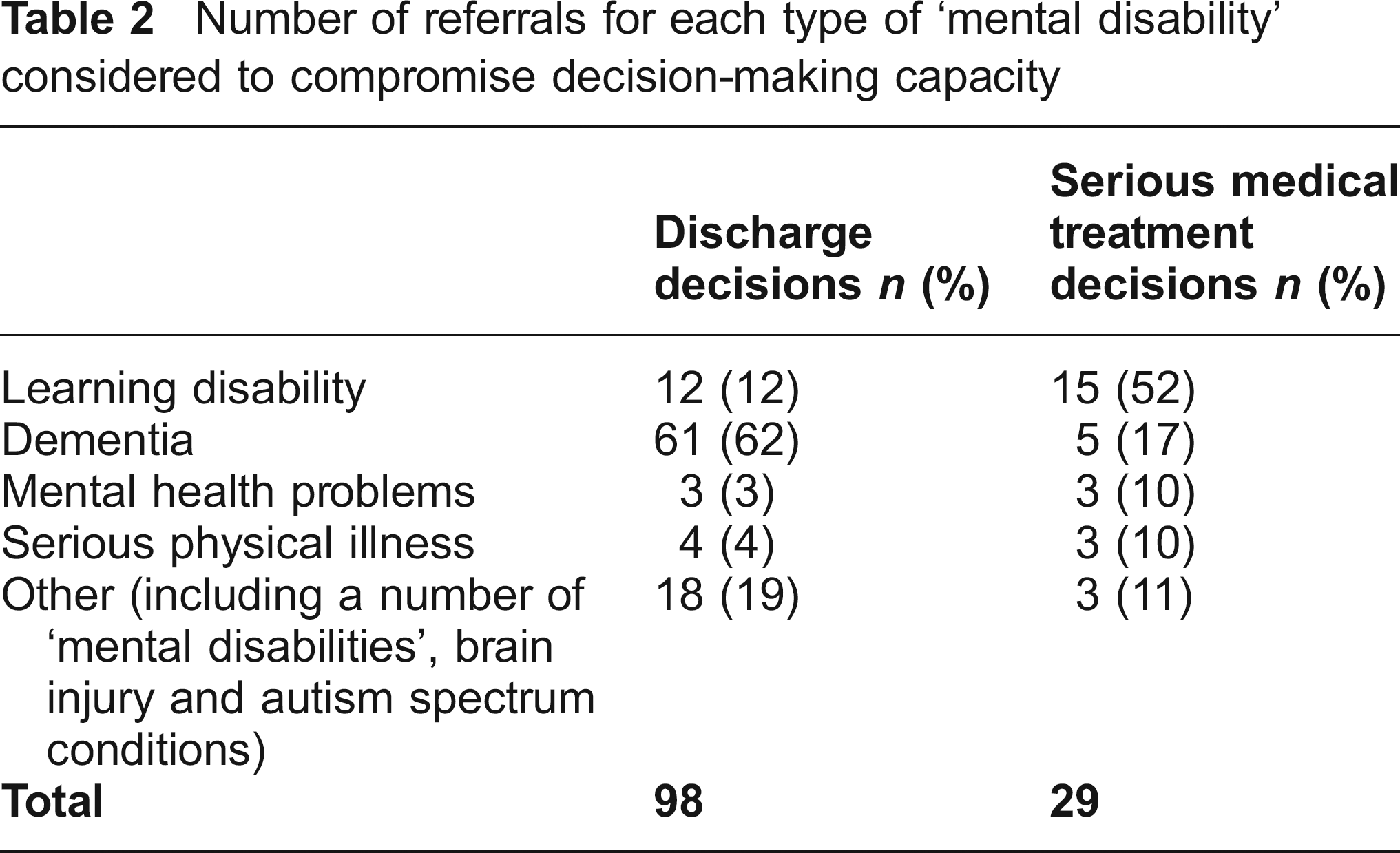
The seven pilot IMCA services received 127 referrals for hospital-based decisions, 29 for a range of hospital-based serious medical treatment decisions (table 1). About half were judged to have difficulties associated with a learning disability (table 2). There were 98 referrals for patients where a change of accommodation was being considered. These were mostly elderly people (modal age group, 80-89 years) diagnosed with dementia (62%). Relatives or friends were available to be consulted in 65 cases, but in 35 of these, they did not wish to be, or could not be (because of frailty or distance), involved. In a further 12, an IMCA was involved because there was thought to be a conflict of interest between the patient and his or her relatives or friends.
Number of hospital-based serious medical treatmentreferrals
Number of referrals for each type of ‘mental disability’ considered to compromise decisionmaking capacity
Most patients (83%) were able to speak English, 14% used alternative means of communication (sign language, pictures and non-standard vocalisations) and only 3% had no obvious means of communication. 3 In 45% of the 60 cases that had been completed by the end of the review period, advocates were confident that, as well as gathering information about a patient's lifestyle and circumstances, they had also ascertained a clear indication of his or her wishes and communicated these to the clinician or manager.
At the time of interview the majority of interview respondents (table 3) only knew of the MCA's pending implementation. Only five clinicians involved in care of the elderly had experience of working with an IMCA for decisions concerning hospital discharge.
Number of interview respondents in each hospital and specialty
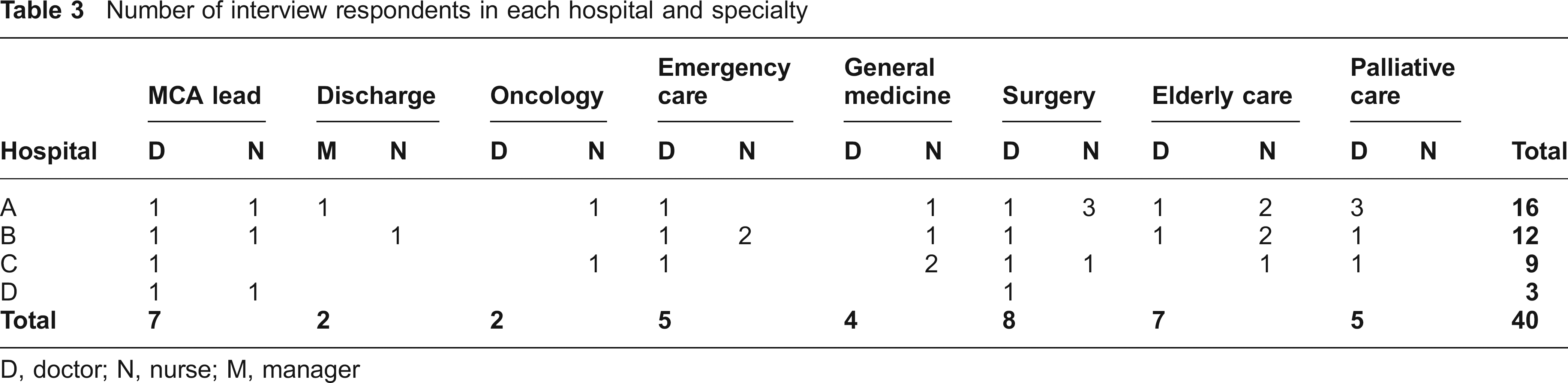
D, doctor; N, nurse; M, manager
Serious medical treatment decisions
Virtually all the respondents were able to identify some potential benefits of involving an advocate. They specifically mentioned how an independent advocate could bring a holistic perspective to a decision, make clinicians more accountable for their decisions, and foreground patients’ wishes in decisionmaking. Nevertheless, while clearly affirming the relevance of these policy commitments, clinicians also raised concerns about the viability of a statutory IMCA service (Box 3). In particular, they referred to practical issues such as the advocates not having any medical training, having a biased rather than impartial point of view, the service being available only within office hours, and being too slow for emergency medical decisions. Specifically, the possibility of an advocate offering a holistic perspective was thought by many to be undermined by their lack of medical knowledge. Two clinicians, however, proffered the contrary view, believing that advocates without medical qualifications were better able to adopt the patients’ perspectives and ask questions appropriately. Several clinicians were concerned that the independence of the service could be compromised by biased views from advocates. A particular worry was that advocates would not be able to relinquish strongly held personal views about when it was or was not appropriate to offer medical intervention.
Clinicians’ responses to the IMCA service
This respondent felt that doctors should be challenged about their decisions, but that it depended on how the challenge was put. She used the phrase, ‘We are all working to the same “best interests” goal’. However, she continued by saying that advocates’ ‘societal view may not understand the medical model’. She could see a value of the advocacy service, but was concerned that IMCAs would not be able to understand the medical factors involved in determining a patient's ‘best interests’.
Consultant in Palliative Care (Hospital B)
This respondent felt that an IMCA could assist in a decision by obtaining additional background information about the patient and providing the decisionmaking team with a better picture of what the patient would have wanted. However, he then pointed out that patients’ wishes can change, and that the information provided by family members may no longer represent their wishes and interests. He had identified a way in which advocacy could improve decisionmaking and assist the medical team, but also expressed a conceptual problem in obtaining reliable patient wishes.
Consultant in Elderly Care (Hospital B)
This surgeon acknowledged that advocacy would, in principle, ensure that patients are treated fairly, but then added that he hoped current medical practice already ensured that patients were treated fairly. He had demonstrated an understanding of the IMCA service as a safeguard for patients’ interests, but felt that such a safeguard was not necessary given the good quality of patient care.
Consultant in Surgery (Hospital A)
This respondent stated that hospital decisionmaking processes would be improved by including the independent view of an advocate. However, he then followed this statement by citing two practical problems associated with the IMCA service: i) he felt that hospital staff would have great difficulty judging a patient's family and friends, and that the MCA offered insufficient guidance for them; and ii) hospital staff would find the process of assessing and documenting capacity to be too complicated in acute medical situations. This respondent had identified a principle benefit of the service, but considered that its delivery may be impractical in hospital settings.
Medical Director (Hospital A)
This respondent said that nurses often take the role of patient advocates because they are able to build relationships with them over the long course of their treatment. She used the phrase, ‘patients don't need any more advocacy’ and stated that she had ‘never felt that a patient is under-represented’. However, she then reflected that another supporting person may be useful in the very complicated decisions. She saw independent advocacy as unnecessary for her patient group, but had also identified the benefit of additional support in particular cases.
Matron in Oncology (Hospital C)
Those respondents with a more detailed knowledge of the legislation were concerned about the exemption from appointing an IMCA in urgent decisions. The problem, as described, by a clinician in elderly care, involves the degree of urgency (e.g. resuscitation compared with surgery following a fractured hip). The precise obligation to appoint an IMCA, or not, was thought to be unclear. Similarly, several clinicians including those with less detailed knowledge of the legislation commented on the difficulty of judging whether relatives were, or were not, ‘appropriate to consult’. Their comments predicted that such judgements would be subjective given that they often had very little information about patients’ families. Many clinicians rejected the idea of statutory advocacy for medical decisions because, as they saw it, multidisciplinary teams already made strenuous efforts to ensure that decisions were made in patients’ best interests. None of the respondents referred to the best interests procedures set out in the MCA, but they did report that when making decisions they consulted with family members or care staff who knew the person, and tried to ascertain the patient's wishes or beliefs. Furthermore, nurses were keen to claim that they already acted as patients’ advocates. Three nurses and one doctor considered that IMCAs could not provide a service that surpassed the advocacy offered by nurses. Another six nurses and five doctors, however, believed that, while nurses can provide patient advocacy, a service provided by an IMCA was thought to have some advantages: more time to ascertain patients’ wishes and obtain personal information; a more extensive legal knowledge; and some credibility with patients who find it easier to talk to someone outside the health care team.
Although the number of respondents from each medical specialty was small, for some, it was possible to identify particular themes. We found that clinicians in emergency care, where most treatment decisions were considered urgent, raised few concerns about involving an advocate because they recognized that their decisions would be exempt from the IMCA service. They did, however, consider that the IMCA service might be useful in a minority of decisions with ethical complications, such as withdrawing treatment from a patient in a persistent vegetative state. In contrast, clinicians caring for older people considered that the service would be relevant and, therefore, raised many of the practical concerns described above, but not as insurmountable barriers to the operation of the service. This group of clinicians had the most experience of working with advocates (both IMCAs and other advocates) and appeared to be the most willing to include advocates in treatment decisions. Clinicians in surgical specialties were most likely to consider decisions to be predominantly determined by medical factors, making irrelevant the involvement of an advocate without medical knowledge. They did, however, report that personal factors were considered where relevant and also considered that advocacy may be useful in a minority of ethically complex decisions, such as advanced decisions to resuscitate a frail patient, or where considering an organ transplant for a patient whose religious beliefs did not support such an operation (Box 4). They also reported that many surgical decisions are made over several consultations, starting with a general practitioner, and that it would be unrealistic to expect an advocate to be present throughout this process. They also felt that a significant proportion of surgical decisions (those following trauma) would be classed as urgent and exempt from the service.
Clinicians’ views of IMCA as an aid in ‘ethically complex’ cases and change of accommodation decisions
This respondent considered that hospital staff would only make referrals to the service where there were difficulties in placing the person in suitable accommodation, or their family disagreed with the proposed options. For her, she could see other practitioners using IMCA as a tool to assist in complicated decisions.
Consultant in Palliative Care (Hospital A)
This respondent considered that advocacy would not be feasible in the majority of Intensive Care decisions, where treatment is often required urgently or patients’ medical conditions change quickly. However, he then stated that advocacy may be useful when looking at whether to withdraw treatment from a patient in a persistent vegetative state. This treatment decision was considered to be ethically complex and one where the IMCA could usefully contribute a more holistic perspective.
Consultant in Intensive Care (Hospital A)
When asked for her understanding of the IMCA service, this respondent stated that it was a person who would be called in to assist complex decisions where the patient lacked capacity. This signalled an understanding of the service a tool rather than a patient right in all eligible SMT and discharge decisions.
Clinical Nurse Manager for General Medicine (Hospital B)
This respondent considered that advocacy involvement in discharge decisions could be very useful. She qualified this by saying that discharge into residential care is a ‘big step for patients’ and that complex financial arrangements needed to be made. She considered that these were ‘difficult’ decisions and hoped that advocacy could assist the process.
Senior nurse in surgery (Hospital C)
Change of accommodation decisions
Almost all the respondents were positive about involving an advocate in discharge decisions. Those clinicians in elderly care settings who had worked with an IMCA gave positive feedback although one clinician felt that involving an IMCA had delayed the discharge of a patient. In contrast to decisions about treatment, applying the eligibility criteria for discharge decisions was seen as straightforward. Their positive views, however, were made with reference to inadequacies in current practice (Box 4). These included poor communication between health and social care teams, and problems in identifying or securing funding for residential placements. In addition, difficulties were reported in situations where relatives disagreed over care arrangements, particularly those requiring the sale of property, or where the decision to be made contradicted patients’ expressed wishes. In this context, clinicians were enthusiastic about involving an advocate: they hoped that advocacy would minimize delays in discharge and ensure that discharged patients were both safe and contented.
Implementation in hospitals
Seven clinicians with hospital-wide responsibility for implementing the MCA were interviewed. All the hospitals had identified wards in which patients at risk of lacking decisionmaking capacity (elderly care, neuro-sciences, intensive care, hepatology and haematology) were most likely to be accommodated. One hospital had collaborated with the IMCA service to raise awareness on its elderly care and neurosciences wards, featured the MCA in a grand round, and organized a special training event on the legislation. In all four hospitals, clinicians leading implementation expressed doubts about the relevance and viability of the IMCA service.
Discussion
Findings
For decisions involving serious medical treatment, clinicians believe that statutory advocacy is mainly either impractical or irrelevant. They believe that the introduction of the IMCA service is of little value in decisions where medical factors predominate, nurses are able to provide patient advocacy, and multidisciplinary teams have the expertise and experience to determine what treatment is in patients’ best interests. While several clinicians identified independence as a benefit of the IMCA service, their beliefs suggest that they do not recognize independence as an essential feature of advocacy. This does not match the widespread view in the advocacy sector, that independence is vital to prevent a conflict of interest and enables the advocate to represent the patient as if they were that person. While some in the advocacy sector might support the role of nurses as patients’ advocates, it is believed that the patient is entitled to a voice that is independent of health care interests and loyalties. For the majority of clinicians, the IMCA service was not seen as a measure for safeguarding the interests of vulnerable people, let alone their human rights, but as a tool useful only in a minority of cases in which ethically complicated decisions had to be made.
In contrast, the involvement of advocates in decisions concerning discharge from hospital was viewed by clinicians as a potential solution to decisions often complicated and slowed down by a variety of social factors. Here their views reflected the belief that advocates without medical knowledge could both assist with decisions that were frequently difficult, and improve an area of health care where practice was thought to be inadequate.
Strengths and weaknesses of the study
This was an evaluation of pilot IMCA services where the respondents had had limited experience of working with non-instructed advocates. Its value lies in its ability to inform those implementing the IMCA service about the attitudes of clinicians who are now under a statutory obligation to make referrals to it.
Implications for implementation
Our findings indicate significant attitudinal barriers to the implementation of the IMCA service. Clinicians responsible for implementation will need to take colleagues’ objections seriously. Since there is no way of monitoring whether eligible patients are referred to the IMCA service, clinicians reluctant to involve an advocate may interpret urgent and serious idiosyncratically. Clinical training will need to address a tension between the MCA's principle of empowering patients and medical expertise of individual clinicians and/or multidisciplinary teams. Furthermore, clinicians need to be aware that while advocates will draw attention to patients’ beliefs, wishes and cultural backgrounds, as is required in determining patients’ best interests, clinical expertise in considering medical factors will not be undermined; the MCA definition of best interests includes consideration of all relevant factors, both personal and medical.
Consistent with other studies,14-16 our findings show that many patients lacking mental capacity can, with appropriate support, contribute to decisionmaking. Training for using the IMCA service and efforts to address objections to it should not be confined to staff working with patients believed to be at risk of lacking decisionmaking capacity. Such patients exist across a wide range of hospital wards.
Clinicians’ enthusiasm for the involvement of advocates in discharge decisions may initially be helpful in promoting acceptance of the service. Unfulfilled expectations may, however, undermine clinicians’ support for the new arrangements. The extent to which an advocate can influence the complex social factors involved in change of accommodation decisions is uncertain; the IMCA service promises only to ensure that patients’ ‘best interests’ are the focus of the decisionmaking process.
Since April 2007 all hospital clinicians in England and Wales have had a duty to appoint an IMCA where appropriate. Our findings suggest that clinicians’ observance of this new duty needs to be monitored.
Footnotes
Acknowledgements
We thank the medical directors of the four hospitals, and all of the clinicians who agreed to be interviewed or assisted in the participant validation exercises. We also thank the managers and Independent Mental Capacity Advocates who were involved in the pilot IMCA services for recording details of all their referrals and contributing to our participant validation exercise. Finally, we would like to thank the Department of Health for funding this research.