
Abstract
Objectives:
The Emilia-Romagna region of Italy has reduced the number of available hospital beds and introduced financial incentives to curb hospital use. The goal of this study was to assess the impact of these policies on changes over time in the number of acute hospital admissions classified in diagnosis related groups (DRGs) that could be treated safely and effectively in alternative, less costly settings.
Methods:
The assessment of the appropriate site of care was based on analysis of hospital discharge data for all hospitals for the selected diagnosis related groups in the Emilia-Romagna region for 2001 to 2005. The necessity for acute hospital admission was based on the severity of a patient's principal diagnosis, co-morbid diseases and, for surgical admissions, procedure performed.
Results:
From 2001 to 2005, potentially inappropriate medical admissions of more than one day decreased from 20,076 to 11,580, a 42% decrease. Inappropriate admissions decreased in both public and private hospitals but there remained a higher rate of inappropriate admissions to private hospitals. Potentially inappropriate medical admissions accounted for 128,319 bed-days in 2001 and 68,968 bed-days in 2005, a reduction of 59,351 bed-days. Potentially inappropriate surgical admissions decreased from 7383 in 2001 to 4349 in 2005, a 41% decrease. Bed-days consumed by inappropriate surgical admissions decreased from 23,181 in 2001 to 13,660 in 2005.
Conclusions:
The Emilia-Romagna region has succeeded in reducing the use of acute hospital beds for patients in selected diagnosis related groups. However, there are still substantial numbers of admissions that could potentially be treated in less costly settings.
Introduction
The appropriate use of the acute care hospital is important for controlling the cost of health care. Reducing the level of inappropriate hospital admissions may also improve the outcomes of medical care. 1 The development of community and ambulatory care services and promotion of appropriate hospital use is an important health policy concern in Italy including the Emilia-Romagna region.
The concept of appropriateness of health care has two components: the appropriateness of the care provided given the characteristics of the patient (i.e. clinical appropriateness) and the appropriateness of the setting in which care is provided (i.e. organizational appropriateness). 2 This paper describes a study undertaken by the Emilia-Romagna region to monitor changes in organizational appropriateness of acute hospital utilization in the region. It describes the criteria used to differentiate appropriate from inappropriate admissions, summarizes the results of a review by a panel of US and Italian clinicians, and analyses the level and trends of potentially inappropriate acute hospital admissions in the Emilia-Romagna region.
The Italian national health service, Servizio Sanitario Nazionale (SSN), was established in 1978 with the goal of providing comprehensive care financed by general taxation. The SSN was modelled on the British National Health Service and combines public financing with a mixture of public and private care providers. The 20 Italian regions have the primary responsibility for the organization and administration of the health care system. The delivery of care is the responsibility of Local Health Units (LHUs) which are funded by the region on a capitated basis and responsible for a wide range of hospital and community services in a geographic area. The Emilia-Romagna region with a population of 4.1 million includes 11 LHUs.
Approximately 85% of hospital care is provided in public hospitals. Private hospitals, if they are accredited, may also provide care under contract financed by the SSN. There are a small number of private non-profit hospitals, mostly church owned. Private, for-profit hospitals treated almost 14% of inpatient cases in 2002. Primary care is provided by GPs and paediatricians contracting with the SSN. While primary care physicians are independent contractors, hospital-based physicians practising in public hospitals are salaried employees of the SSN and may not also practice in private for-profit hospitals contracting with the SSN.3,4
In the mid-1990s two major initiatives were undertaken to control the use of both public and private contracted hospitals. A national program of bed reduction and hospital closures was initiated in 1996; between 1996 and 2001, bed capacity was reduced by 20%. A diagnosis related group (DRG)-based hospital financing system was introduced in Italy in 1994. Control mechanisms implemented by the regions to counteract the incentive inherent in a prospective payment system to increase admissions included automatic reductions in total payments when expenditures exceeded specified thresholds set at either the individual hospital or regional level. In 1995-1998, the initial period after the implementation of the prospective payment system, some Local Health Units in the Emilia-Romagna Region reached agreements with public hospitals to reduce tariffs for selected DRGs of low complexity. Uniform regulations at the regional level were implemented beginning in 1999, in which DRG-specific tariffs were used to influence patterns of care by setting rates below cost to discourage admissions for certain patient types. For example, tariffs for inpatient admission for medical and surgical DRGs considered treatable in outpatient settings were reduced by as much as 50%. 3
Efforts to prevent unnecessary hospital admissions resulted in the publication of a national list of 43 DRGs deemed to be at high risk of including inappropriate admissions, i.e. clinical problems that can be safely and effectively treated in alternative settings to the acute hospital. 5 The Emilia-Romagna region expanded the list to 62 by adding DRGs for which the region had implemented policies such as incentives for the GPs to control appropriateness as well as ‘adjacent DRGs’, i.e. DRGs with the same primary diagnosis but differentiated by the presence of complications or co-morbidities. (The list of 62 DRGs is included as an appendix.)
Methods
Assessment of appropriateness of admission
Analyses focused on admissions to public and private hospitals in Emilia-Romagna for residents of the region aged 18 to 74 years during the period 2001 through 2005. Sixty-two DRGs were selected that may include inappropriate admissions to an acute hospital in that some of the patients classified in these DRGs can be treated with efficacy and safety in alternative, less costly settings.
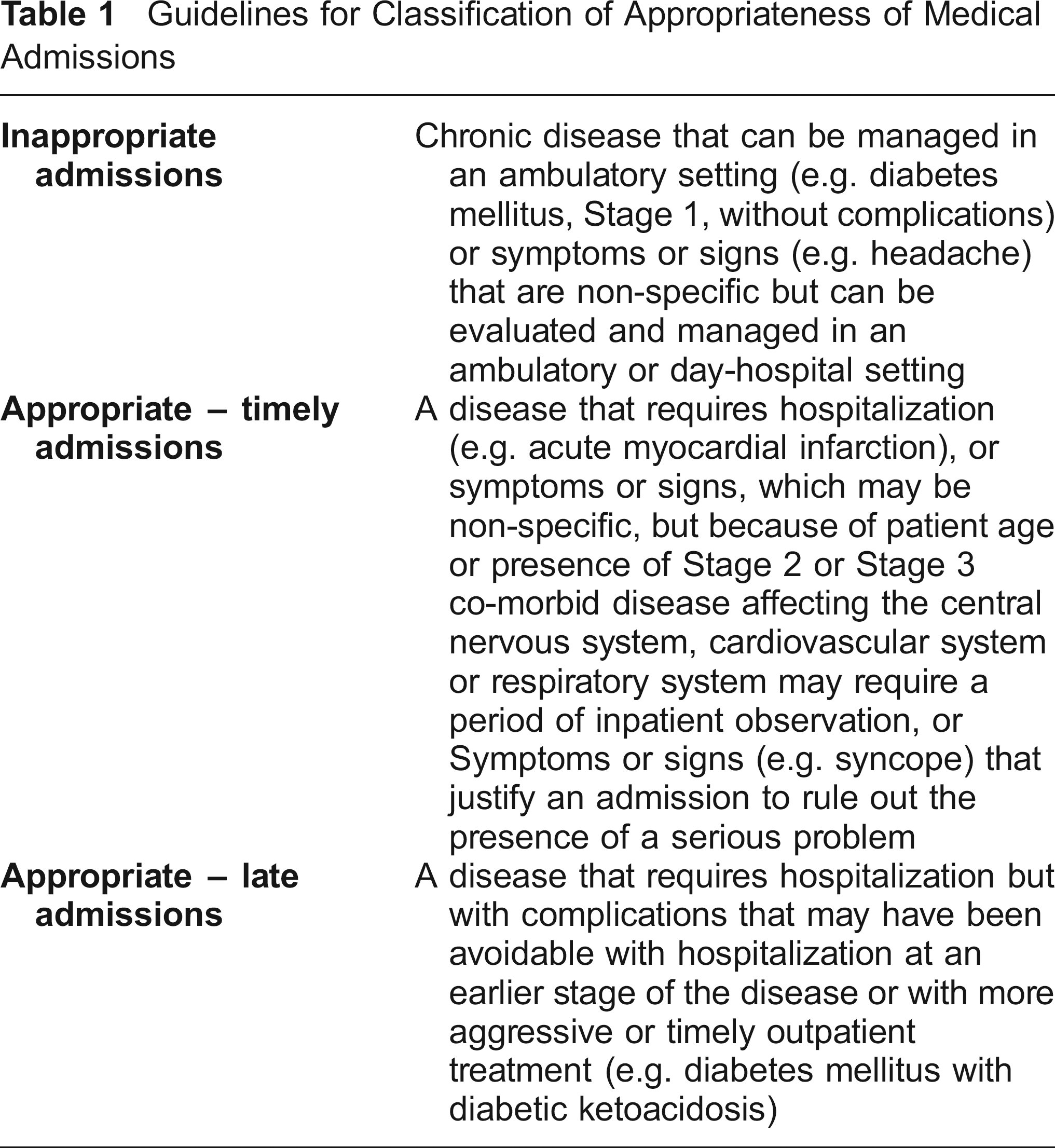
Admissions were classified into one of three appropriateness groups: inappropriate, appropriate and timely, and appropriate but late. The guidelines developed to classify appropriateness of medical admissions are shown in Table 1. Appropriate admissions were divided into two groups, timely and late, in order to assist in the identification of potentially preventable late stage hospitalizations, i.e. patients with complications that may have been avoidable with earlier hospitalization or with more timely or higher quality outpatient care. 6 In both situations, hospitalization is necessary and appropriate. However, for some problems such as diabetic ketoacidosis, the hospitalization is appropriate but may have been avoidable. For some problems, such as bacterial pneumonia with a lung abscess or empyema, hospitalization earlier in the disease progression would be preferable, reducing morbidity and risk of death.
Guidelines for Classification of Appropriateness of Medical Admissions
The selected medical DRGs include a mixture of disease-specific DRGs (such as diabetes mellitus, DRG 294) and ill-defined DRGs based on symptoms or signs (such as DRG 142, syncope and collapse). Even the disease specific DRGs, however, may have large differences in disease severity within the DRG. For example, DRG 294 includes diabetes mellitus without complications as well as diabetic coma. The surgical DRGs include quite specific procedures (such as carpal tunnel release, DRG 6) as well as DRGs that include a wide range of procedures (such as other skin, subcutaneous and breast procedures, DRG 270). Because of the clinical heterogeneity within the selected DRGs it is not possible to say some of the DRGs should be treated in acute setting and some can be treated in alternative settings. The challenge in defining organizational appropriateness is to look within the DRGs and assess the mix of patients classified within each. In order to accomplish this goal, the more clinically oriented Disease Staging classification was used to classify the severity of a patient's principal diagnosis and co-morbid diseases. 7,8 Surgical procedure performed, when relevant, were also identified based on specific ICD-9-CM codes.
Using the 2001-2005 Emilia-Romagna hospital discharge abstract database, all records were classified using the DRG software and the Disease Staging software and all Disease Staging diagnostic categories and all surgical procedures falling within the selected DRGs were identified. Using the agreed guidelines, two physicians from Jefferson Medical College reviewed all the selected staged diagnostic categories and ‘mapped’ them to the appropriate groups defined in Table 1. Subsequently, a panel of 14 Italian clinicians was selected by the Emilia-Romagna region to review the criteria. The physicians from Jefferson Medical College were specialists in internal medicine/infectious diseases, and family medicine. They consulted with colleagues from other specialties when additional input was wanted. The Italian clinicians included medical specialists in internal medicine, emergency medicine and psychiatry and surgical specialists in general surgery, orthopaedic surgery, anaesthesiology and eye surgery.
For surgical admissions, the nature of the surgical procedure performed was also assessed. Procedure codes within the selected DRGs were identified empirically and reviewed by the clinicians to determine whether an ordinary admission is necessary or, assuming the appropriate facilities are available, the procedure can be safely and effectively performed in an ambulatory or day-surgery setting. For example, a unilateral repair of a direct inguinal hernia was classified as a procedure that can be performed in day-surgery while a bilateral repair of an indirect inguinal hernia was classified as a surgical procedure that would justify an acute hospital admission.
Co-morbid disease, i.e. a problem already present in the patient but which was not the main reason for the admission, may modify the appropriateness of hospitalization. For example, the presence of essential hypertension without complications as a co-morbid disease would not justify an ordinary admission for any of the principal diseases analysed. However, a patient with viral pneumonia, who also had chronic obstructive pulmonary disease, might appropriately be admitted to the hospital. Therefore, chronic obstructive pulmonary disease would be considered a significant co-morbidity for this principal diagnosis. Following this logic, a co-morbidity threshold was identified for each co-morbid disease appearing in the database for the selected DRGs. The ‘final’ appropriateness group for each admission takes into consideration the patient's principal diagnosis and stage, the presence and stage of a patient's co-morbid disease, and the nature of operating room procedures performed (for surgical admissions).
In order to assess potential negative impact on patient outcomes of changes in the pattern of hospital use, changes in mortality rates and rates of repeated admissions were analysed. In-hospital mortality rates were calculated for the selected DRGs and age/sex adjusted mortality rates were calculated using direct standardization using the region's demographic database and the standard population from the Italian National Institute of Statistics.
Results
The panel of Italian clinicians reviewed 557 combinations of diagnosis and severity stage. The Italian panel agreed exactly with the initial criteria in 89.0% of the cases or was stricter in the sense that they indicated that more patients could be safely and effectively treated in a less intensive level of care (day hospital or ambulatory setting) instead of an acute hospital setting (9.5%). In 1.5% of the diagnosis/stage combinations, the Italian panel recommended a higher level of care than the initial criteria. The classifications used in our analysis reflect the input from the Italian clinicians with refinements made to account for new versions of both the DRG software and the Disease Staging software. An example of the mapping for diabetes mellitus is shown in Table 2. For early stage bacterial pneumonia and epilepsy the Italian clinicians recommended additional studies of appropriateness of admissions using laboratory data or prior diagnostic information not available in the administrative data used for this study. These admissions were excluded from the analysis.
Appropriateness of diabetes mellitus diagnostic groups
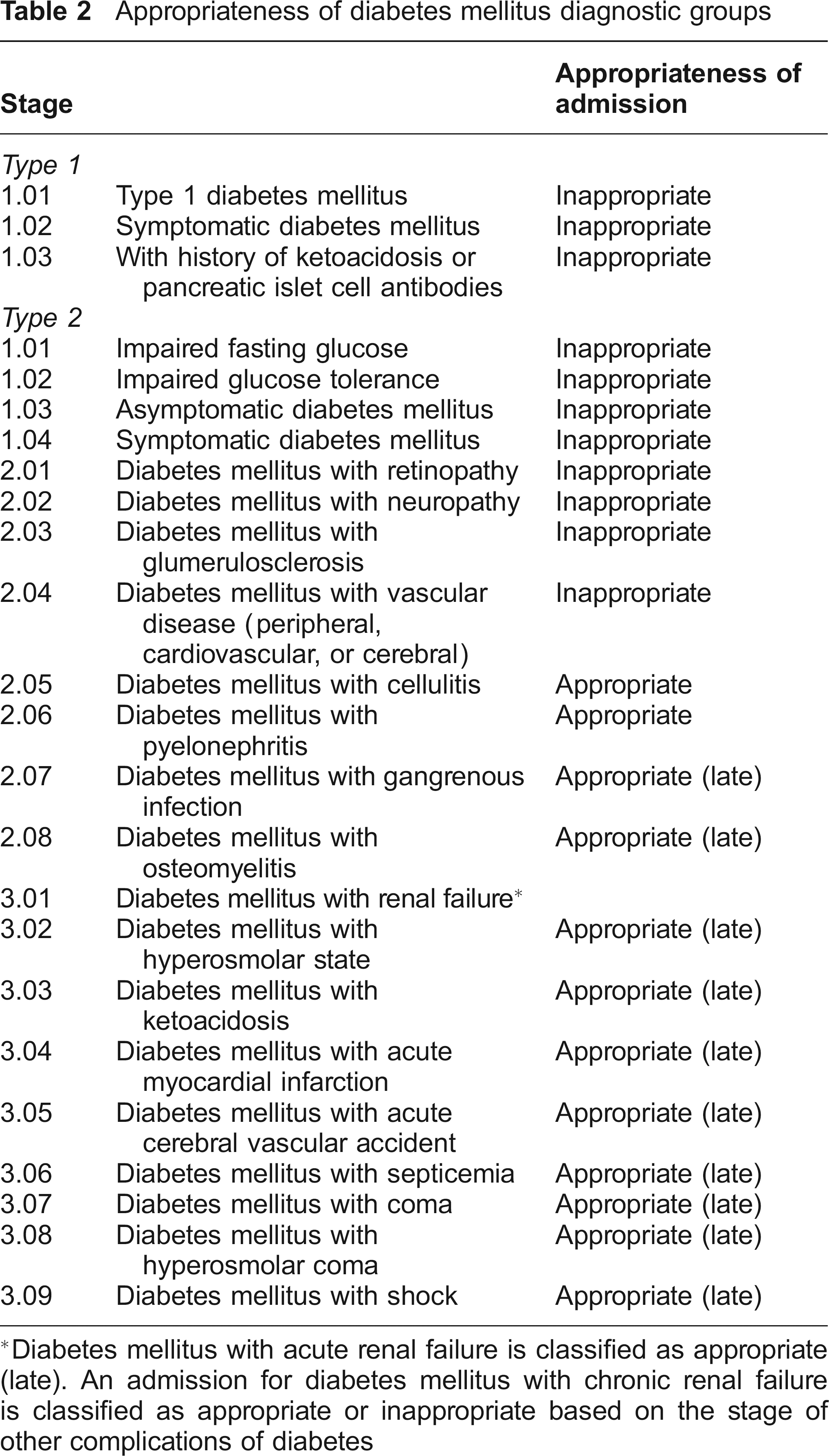
Diabetes mellitus with acute renal failure is classified as appropriate (late). An admission for diabetes mellitus with chronic renal failure is classified as appropriate or inappropriate based on the stage of other complications of diabetes
In 2005, there were 451,860 day hospital and acute hospital admissions of residents of Emilia-Romagna between the ages of 18 and 74 years admitted to hospitals in the region. Of these, 112,712 were classified in one of the 62 DRGs selected for analysis (Table 3). There is a trend towards less use of the hospital with 55,991 fewer admissions in 2005 than 2001, a reduction of 11%. The change was larger among the selected DRGs, with 39,107 fewer admissions in 2005 than in 2001, a reduction of 26%. The location of care and the profile of organizational appropriateness are displayed in Table 4 for the selected surgical DRGs and Table 5 for medical DRGs.
Number of day hospital and ordinary admissions, Emilia-Romagna region *

Residents of Emilia-Romagna aged 18-74 years hospitalized in hospitals in the region, excluding admissions to departments of long-term care, rehabilitation, neuro-rehabilitation, spinal care and psychiatry
Location of care and profile of organizational appropriateness, selected surgical DRGs *
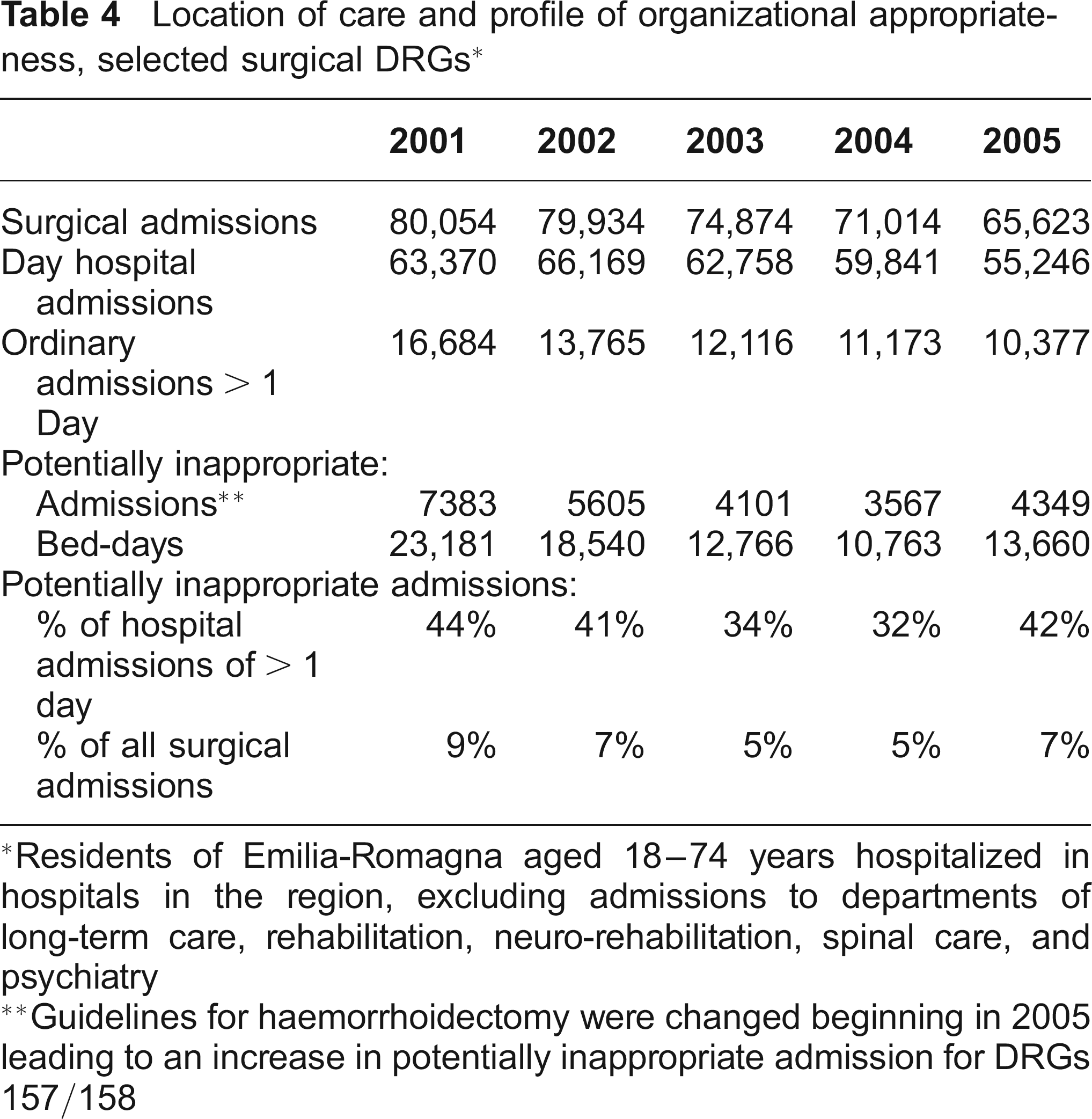
Residents of Emilia-Romagna aged 18-74 years hospitalized in hospitals in the region, excluding admissions to departments of long-term care, rehabilitation, neuro-rehabilitation, spinal care, and psychiatry
Guidelines for haemorrhoidectomy were changed beginning in 2005 leading to an increase in potentially inappropriate admission for DRGs 157/158
Location of care and profile of organizational appropriateness, selected medical DRGs *
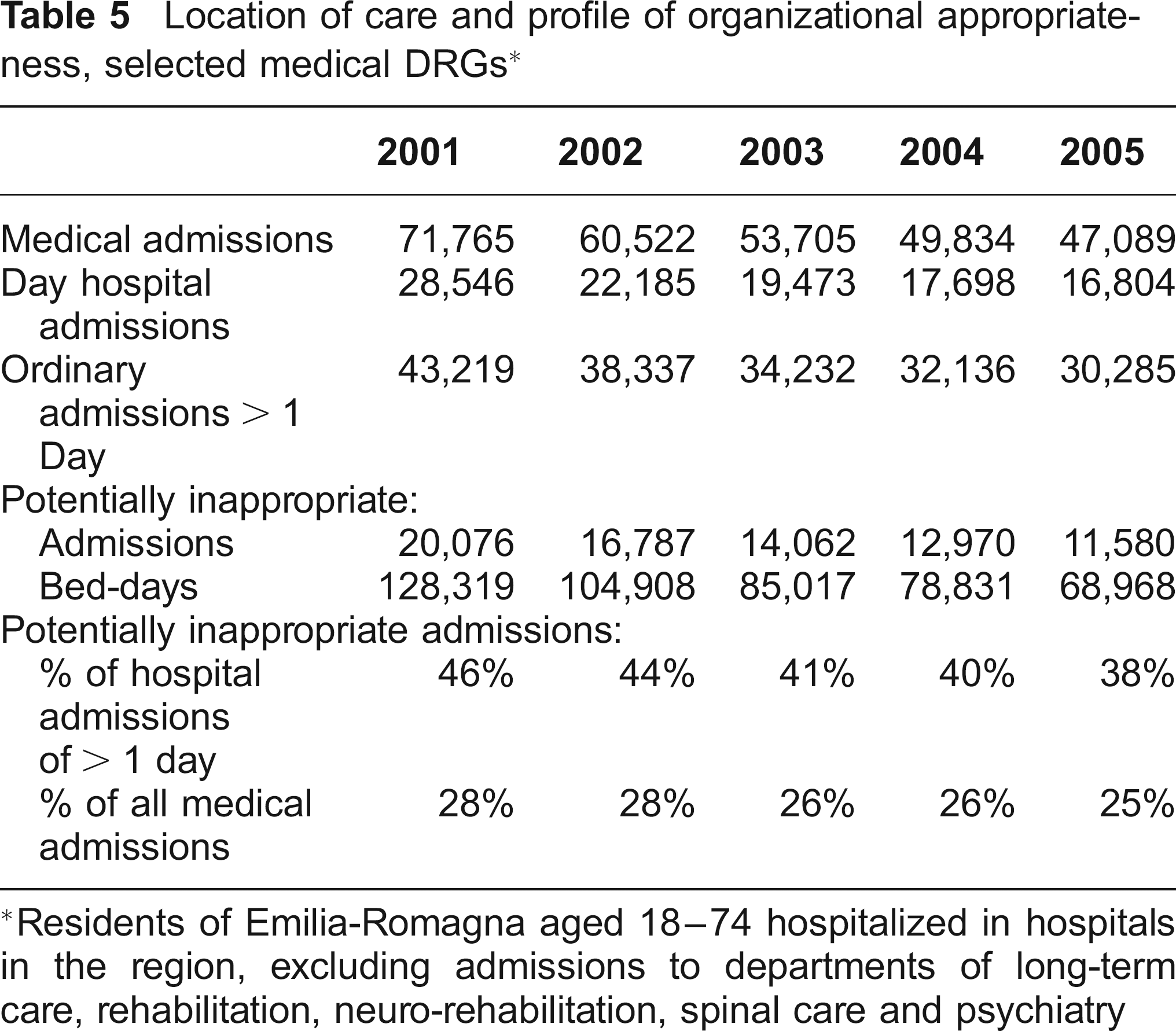
Residents of Emilia-Romagna aged 18-74 hospitalized in hospitals in the region, excluding admissions to departments of long-term care, rehabilitation, neuro-rehabilitation, spinal care and psychiatry
There were important changes in the profile of care for surgical procedures analysed. Of the 80,054 surgical admissions in 2001, 16,684 (21%) involved an acute hospital admission of greater than one day, with the remainder of these procedures performed in a day-surgery setting. In 2005, 10,377 were performed during an acute hospital admission of greater than one day, 38% fewer than in 2001. The number of admissions of more than one day that were judged to be potentially inappropriate decreased from 7383 in 2001 to 4349 in 2005. Bed-days consumed by inappropriate surgical admissions decreased from 23,181 in 2001 to 13,660 in 2005. In 2005, admissions judged to be potentially inappropriate admissions were 44% of the acute hospital admissions of greater than one day and 9% of the procedures performed in the selected DRGs.
For the selected medical DRGs, the total number of day hospital and acute hospital admissions decreased over the five years of the study from 74,261 to 40,079. Acute hospital admissions of more than one day decreased by 29%; from 45,715 to 32,275 (Table 5). Of the patients admitted for more than one day, potentially inappropriate admissions decreased by 42% from 20,076 in 2001 to 11,580 in 2005. Potentially inappropriate medical admissions accounted for 128,319 bed-days in 2001 and 68,968 bed-days in 2005, a reduction of 59,351 bed-days. However, potentially inappropriate medical admissions in 2005 were still 38% of the acute hospital admissions of more than one day and 25% of all medical admissions in the selected DRGs. The number of appropriate but late admissions decreased over time; in 2001, there were 6907 appropriate but late admissions while in 2005 there were 6393 late admissions.
The majority of health care in Emilia-Romagna is provided in public hospitals; 84% of hospital beds in the region are in public hospitals. However, there are private hospitals which provide care under contract with the region. The number and percentage of potentially inappropriate medical admissions to public and private hospitals are displayed in Figure 1. In 2001 there were 17,101 potentially inappropriate admissions to public hospitals and 2975 to private hospitals. Of the private hospital admissions, 61% were judged to be inappropriate in 2001. The number and proportion of inappropriate admissions to both public and private hospitals decreased from 2001 to 2005. However, in 2005, 37% of public hospital admissions and 53% of private hospital admissions were potentially inappropriate.
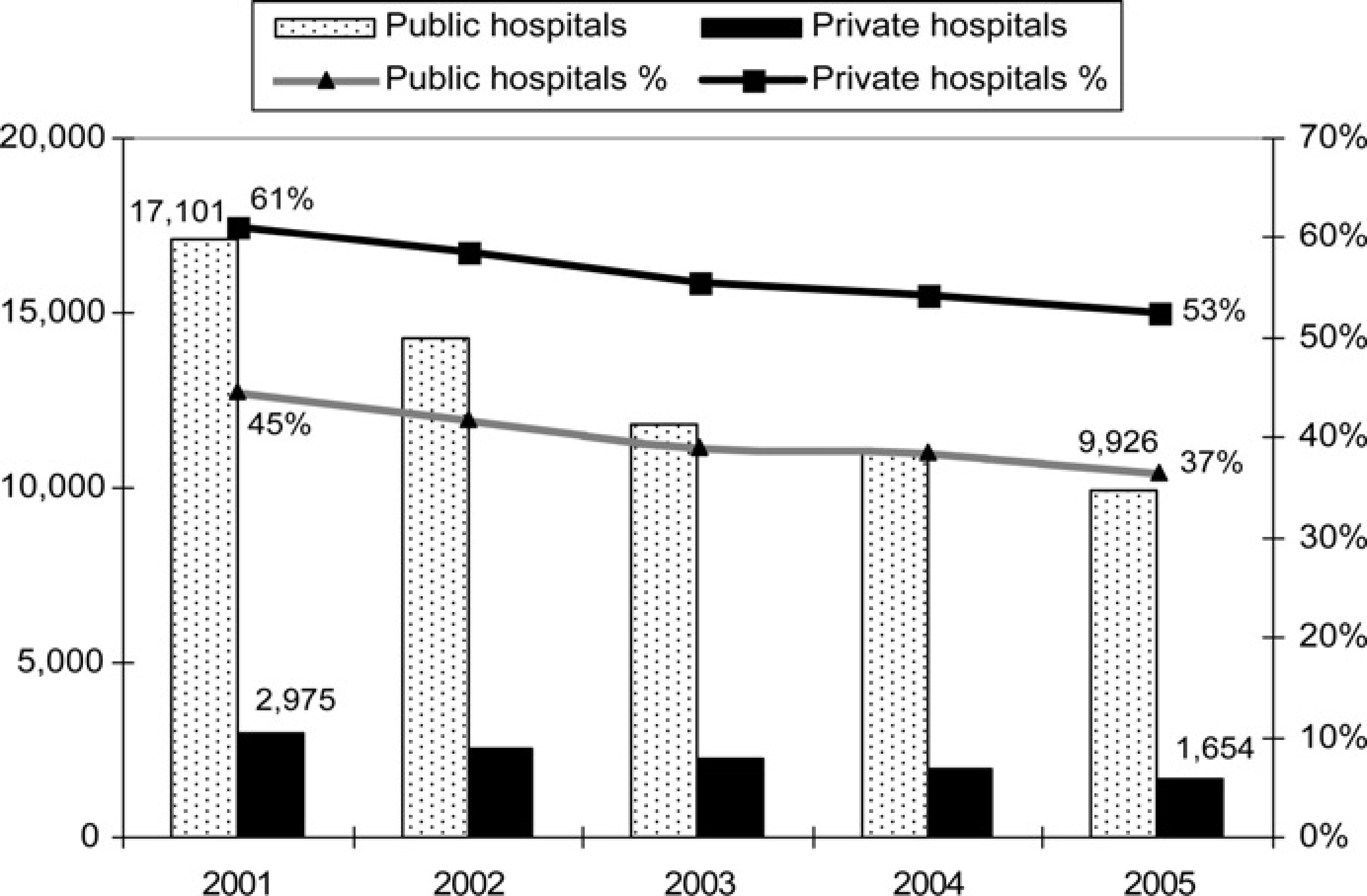
Number and percentage of inappropriate medical admissions, public and private hospitals
Both the crude mortality rate and the age/sex-adjusted mortality rate decreased from 2001 to 2005. No changes were observed in inpatient mortality rates for patients hospitalized for conditions classified in selected DRGs. Re-admissions did not change significantly; in 2001,91.7% of patients in the selected DRGs had only one admission compared to 92.0% of those hospitalized in 2005.
Discussion
Efforts in Emilia-Romagna to improve the appropriateness of acute hospital use appear to have been successful for both the medical and surgical cases identified as targets for improvement. For the elective surgical procedures evaluated, the site where these procedures were performed did change substantially. Comparing 2001 to 2005, there was a 38% reduction in the number of these procedures performed in the context of an acute admission of more than one day. Of the acute hospital admissions of more than one day, there were 41% fewer potentially inappropriate admissions.
The total number of medical admissions in the selected DRGs decreased from 74,261 to 49,079 over the five years of the analysis. It is unlikely that this reflects changes in the prevalence of disease. It is more reasonable to assume that these patients are now being treated in ambulatory settings. If there were serious problems in the ambulatory care provided to this population potentially avoidable complications might be expected to lead to late admissions. 9,10 It is therefore reassuring that the number of late admissions in the selected medical DRGs decreased from 2001 to 2005. In addition, no changes were observed in mortality rates or re-admission rates for the selected DRGs and overall mortality rates decreased slightly.
Despite these changes, there remain a relatively high number of potentially inappropriate admissions. The higher proportion of inappropriate admissions in private hospitals is especially troubling.
Several tools are available for the assessment of appropriateness of hospital admission. 11,12 In particular, the Appropriateness Evaluation Protocol (AEP) has been widely used in Italy to identify potentially avoidable use of hospital resources. 13,14 However, the AEP depends on review of the medical record, requires specially trained personnel, and would be prohibitively expensive to apply in order to analyse the more than 500,000 admissions in the region. The method used in this study is based on routinely collected hospital discharge abstract data and is therefore less costly to use for monitoring the impact over time of the policies of prospective financing and bed closures implemented by the Emilia-Romagna region.
The criteria for assessing appropriateness of hospital admission used in this study were developed by physicians in the US and validated through review by a panel of clinicians from the Emilia-Romagna region of Italy. There was a high degree of agreement between the Italian and US clinicians. 15
The validity of the results may be limited by the use of ICD-9-CM coded hospital discharge abstract data which are the basis for both the DRG and Disease Staging classification used in this study. These data may not include information relevant to the determination of appropriateness of admission such as a complete record of complications and co-morbid disease. This information may be more relevant for assessing appropriateness of certain medical admissions, but is likely to be less important for the elective surgical procedures included in the analysis. Surgical procedures are likely to be well coded in administrative databases. 16 One study found that administrative data generally agree with patient chart data for recording of co-morbidities although co-morbidities tend to be under-reported in administrative data. 17 Observed changes in the levels of appropriateness of hospitalization may be influenced by coding changes. In fact, for the selected DRGs, the percentage of records with 4 or more ICD codes recorded increased from 20% in 2001 to 26% in 2005. Given fewer inappropriate admissions, this degree of coding change is not unexpected. Additional studies, including review of a sample of medical records, would be necessary to compare the validity and reliability of the AEP to the method used in this study. However, simply adding more codes would not necessarily change either the DRG or Disease Staging classification assigned to an encounter. And, the substantial overall reduction in the number of admissions would not be affected by ICD coding.
The Emilia-Romagna region has a system in place to monitor the quality of diagnosis and procedure coding in their hospital discharge abstract data. Controls at both the hospital and regional level assess the validity of coding and the consistency of codes assigned such as congruity between sex, age and diagnosis and between diagnosis and procedure. Despite the limitation of administrative data, they have many advantages for evaluation of regional or national policies: they are readily available, relatively inexpensive to analyse and cover large populations over many years. They are ideal for uncovering patterns of care. If information from the medical records is needed, the results of these analyses can then be supplemented by focused clinical reviews at the local level. 18
Many factors besides a patient's clinical characteristics may influence the decision to admit a patient to the acute hospital. Some of these factors are related to the availability of specific diagnostic and treatment facilities in the day-hospital or other settings. The availability of alternative care such as home care may affect the decision to admit a patient. A patient's family situation may also be considered. While it is not possible to evaluate all of these factors using data from the hospital discharge abstract, or even the complete medical record, the type of information described in this article can be used by clinicians and managers at the local level as a screening tool to help identify ways of improving the efficiency of use of the acute care hospital while providing the appropriate level of alternative, lower intensity treatment settings for patients who do not need acute care hospitalization.
The introduction of DRG-based prospective payment system runs the risk of hospitals increasing the quantity of admissions to offset the constraints on per admission reimbursements. To counterbalance this risk, the Emilia-Romagna region implemented a number of reforms including a reduction in the available bed stock in regional hospitals and a decrease in tariffs for selected DRGs considered to be at high risk of inappropriateness. The study described herein is a part of the region's efforts to monitor to the impact of these changes in health policy. The results appear to be promising in terms of increasing appropriateness of hospital use. Whether or not this has led to increasing efficiency will require additional analyses of the availability of alternative health care services, cost to the SSN, the Emilia-Romagna region, and to patients and their families, and quality of care provided outside the acute care hospital.19,20
Footnotes
Acknowledgements
This project was funded by the Agenzia Sanitaria Regionale, of the Emilia-Romagna region, Italy. The authors would like to thank the clinicians who provided their expertise to this project. Their input was invaluable; however, the authors take responsibility for errors.
Appendix
Medical and surgical DRGs identified by the Italian Servizio Sanitaria Nazionale and the Emilia-Romagna region as including potentially inappropriate admissions.