
Abstract
Objective:
There is increasing international interest in DNA biobanks but relatively little evidence concerning appropriate recruitment methods for these repositories of genetic information linked to patient-specific phenotypic data. To this end, our study aimed to investigate the attitudes of members of the public recruited through general practices to the donation and storage of blood left over from routine clinical tests in general practice.
Methods:
A questionnaire was mailed to 2600 individuals randomly selected from two general practice patient lists in Dundee, Scotland. Using a 7-point Likert scale, respondents rated their attitudes toward DNA biobanks in general, and procurement of blood samples specifically.
Results:
Overall, 841 (34%) of 2471 delivered questionnaires were returned. Compared with patients on the practice lists, respondents were older and more likely to be women. A majority of respondents (61%) were unequivocally positive about storing blood left over from routine tests. Despite general support for this collection method, when asked about open-ended consent, respondents expressed concern about future uses. Respondents’ increasing age and level of deprivation had significant adverse effects on attitudes towards making leftover routine biological samples available for research (P = 0.013 and P = 0.034, respectively). The study had three main limitations: there was a low response rate (34%) such that respondents were not entirely respresentative of the survey population; some respondents had difficulty with the questionnaire; and the study was somewhat underpowered for some comparisons.
Conclusion:
Despite its limitations, this first survey of a general practice population suggests that the majority would be willing to consider giving open-ended consent for the use of blood left over from routine clinical tests in general practice to be stored and used later for medical research.
Introduction
A DNA biobank is a repository of genetic information usually associated with patient-specific clinical information. 1 The potential usefulness of DNA biobanks relies on their large size to provide the power to detect the usually very small differences in phenotype that common genetic variants carry. Access to extensive clinical information is also necessary to realize a biobank's full potential to improve health care, suggesting a concerted population-based approach to recruitment is preferable to ad hoc or opportunistic methods. For population-based studies, obtaining informed consent for both donation and future uses presents a practical problem, 2 especially the latter, which may be impossible to predict at the time of donation. DNA biobanks are designed to facilitate future investigation in unforeseen projects and some argue that requiring consent for each new investigation threatens to stifle research before it begins. 3
A more practical option may be to obtain open-ended consent in advance, allowing the use of DNA samples for future research.4,5 The UK's Biobank project and the Estonian Genome Project already employ this approach.6,7 In principle, such a system could be deployed through general practices so that biological samples would be collected over time from routine tests by retaining left over blood. This method offers a potentially efficient way of collecting blood samples without additional tests 8 and through a trusted party, the general practitioner (GP). Existing large-scale DNA biobank projects such as Generation Scotland (http://129.215.140.49/gs/gindex.html) would be well-placed to benefit from wider contribution engendered by this means.
Ethical considerations around the use of leftover biological materials are, however, controversial. 9 Whether a patient owns these materials is open to debate, as is who should benefit from discoveries made through DNA biobank research. 4 Van Diest has argued that solidarity should take priority over self-determination. 9 Close academic-industry links mean that patients may unknowingly provide samples for commercial research through arrangements between academics and industry 10 and concerns around the possible identification of donors remain. 11 Professional and scientific views on DNA biobanking make valuable contributions (see, for example, Godard et al. 10 ) but the views of potential donors are essential if this debate is to be truly informed. To date, studies reporting the views of individuals on the use of stored biological samples have involved individuals who were already participating in a research project, receiving medical care, or members of the public participating in random surveys.4,12 To our knowledge, no studies have investigated the attitudes of individuals recruited through their general practice to the donation and use of leftover biological material for research.
The current study therefore aimed to explore the attitudes of individuals contacted through their GP to donating, storing and using blood left over from general practice routine tests. Moreover, we wanted to be able to comment on both general attitudes to donating leftover blood together with more specific issues such as linking that blood to a patient's medical record.
Methods
A six-page, nine-question questionnaire was developed; the first two pages described the study and provided a telephone number in case of questions. Since we aimed to collect information on attitudes regarding future behaviour, we based the design of seven questions on the theory of planned behaviour (TPB) 13 and used a manual (TPB manual) available at http://www.rebeqi.org/?pageID=34&ItemID=72 as a guide. Attitude is a dimension that can be measured directly using the TPB and the questionnaire was developed iteratively by ST using the TPB manual and feedback from AD and a psychologist unconnected with the project. Each of the seven questions comprised three related items scored on a 7-point Likert scale that ranged from ‘Strongly agree’ to ‘Strongly disagree’. There was a hierarchy to the questions, moving from attitudes towards storing blood for medical research through to long-term storage and linking samples to medical records. The questionnaire is given in Appendix 1 (www.jhsrp.rsmjournals.com/cgi/content/full/14/1/13/DC1).
Two general practices in Dundee, UK, took part in the study. For this exploratory study, we selected these practices on the pragmatic grounds that one practice was in the city centre (Practice 1) while the second was in a more affluent area outside the city centre (Practice 2). To guarantee the anonymity of respondents, there were no identifiers, which therefore precluded sending reminders to non-respondents and asking why non-responders had not responded. We aimed to recruit 400 individuals from each practice, which would give a two-sided 95% confidence interval for a single proportion using the large sample normal approximation that extended 0.049 from the observed proportion for an expected proportion of 0.5.
We expected the response rate for our unsolicited questionnaire with no reminder to be around 30% based on data presented in the Cochrane review of methods to increase response rates to postal question-naires. 14 To meet our target of at least 400 completed questionnaires from each practice, we sent the questionnaire to 1300 individuals (2600 in total) over the age of 16 years who were randomly selected from the patient list of each practice. The tool random.org was used to generate the list of random numbers used to select individuals. A letter from the individual's GP was enclosed with the questionnaire, both of which were sent in August and September 2005.
As described in the TPB manual, responses to the three items for each question were averaged, reversing the scales where necessary to ensure that a score of 1 was always the most positive score. These averaged scores were rounded up to the nearest integer and the proportion of scores falling into each point (i.e. 1, 2, … 7) on the 7-point scale was calculated for each question for graphical presentation. This was done separately for each practice and for both practices combined.
We were particularly interested in the proportion of respondents that could be considered completely positive to saving leftover blood because this is likely to define the minimum proportion of individuals who would consent to donating leftover blood in future work. We defined a person scoring less than 4 for all seven Likert-scale questions as being unequivocally positive to the proposal of storing blood left over from routine tests; the proportion of respondents falling into this category was calculated for each practice. Responses to the Likert-scale questions for the two practices were compared using the Mann-Whitney test. The chi-squared test was used to compare the proportions of respondents at each practice who were unequivocally positive to storing leftover blood. The correlation between practice, age, sex and being unequivocally positive was also explored using logistic regression.
Results
Table 1 provides descriptive statistics for respondents to the postal questionnaire, together with some baseline information for the 2600 individuals to whom a questionnaire was sent. We received 841 completed questionnaires, 325 from Practice 1 and 516 from Practice 2. A further 129 questionnaires were returned undelivered, which gave a corrected response rate of 34% (841/2471). Compared to patients on the practice lists, respondents were older and more likely to be women.
Descriptive statistics for the survey respondents
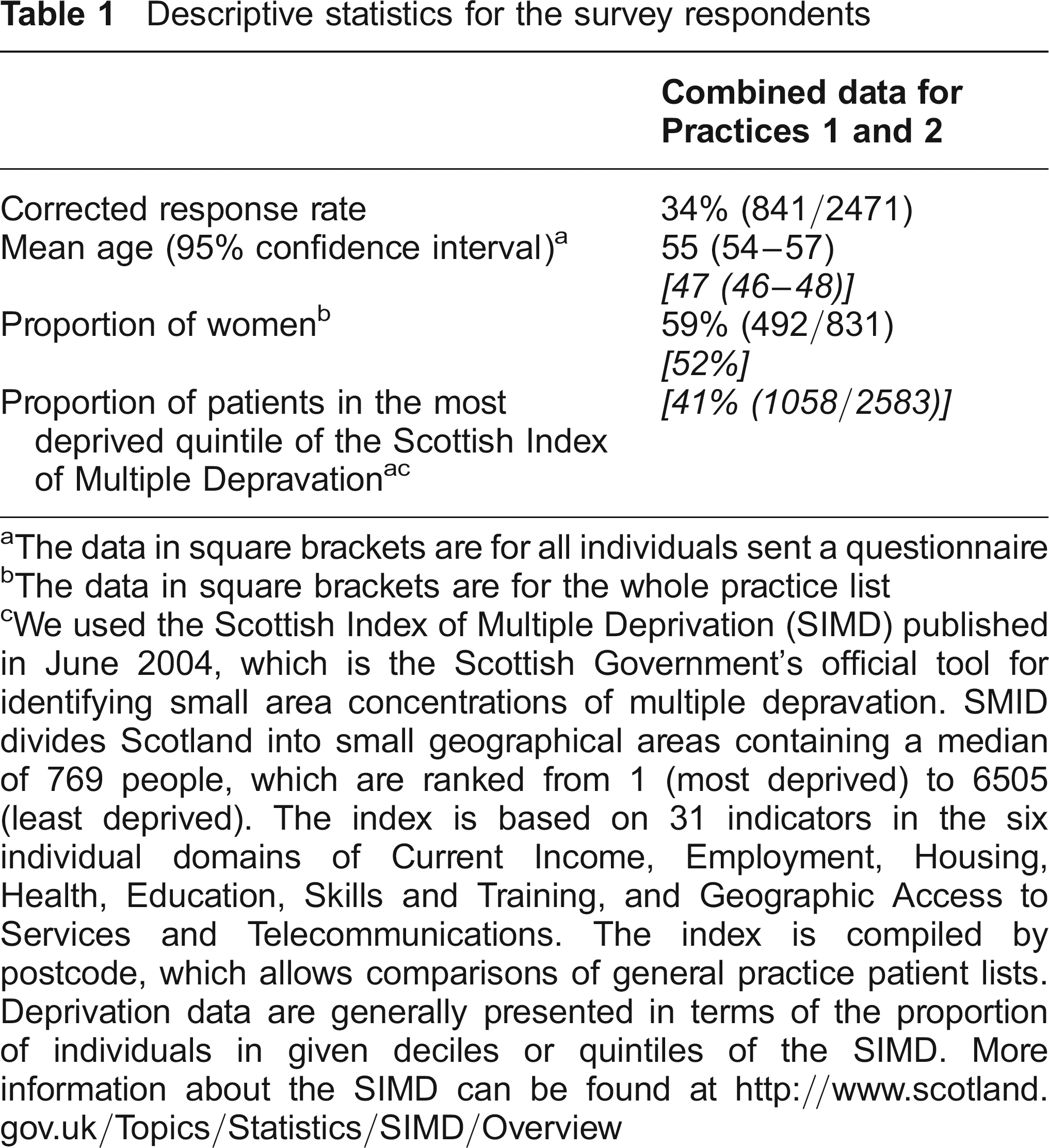
The data in square brackets are for all individuals sent a questionnaire
The data in square brackets are for the whole practice list
We used the Scottish Index of Multiple Deprivation (SIMD) published in June 2004, which is the Scottish Government's official tool for identifying small area concentrations of multiple depravation. SMID divides Scotland into small geographical areas containing a median of 769 people, which are ranked from 1 (most deprived) to 6505 (least deprived). The index is based on 31 indicators in the six individual domains of Current Income, Employment, Housing, Health, Education, Skills and Training, and Geographic Access to Services and Telecommunications. The index is compiled by postcode, which allows comparisons of general practice patient lists. Deprivation data are generally presented in terms of the proportion of individuals in given deciles or quintiles of the SIMD. More information about the SIMD can be found at http://www.scotland.gov.uk/Topics/Statistics/SIMD/Overview
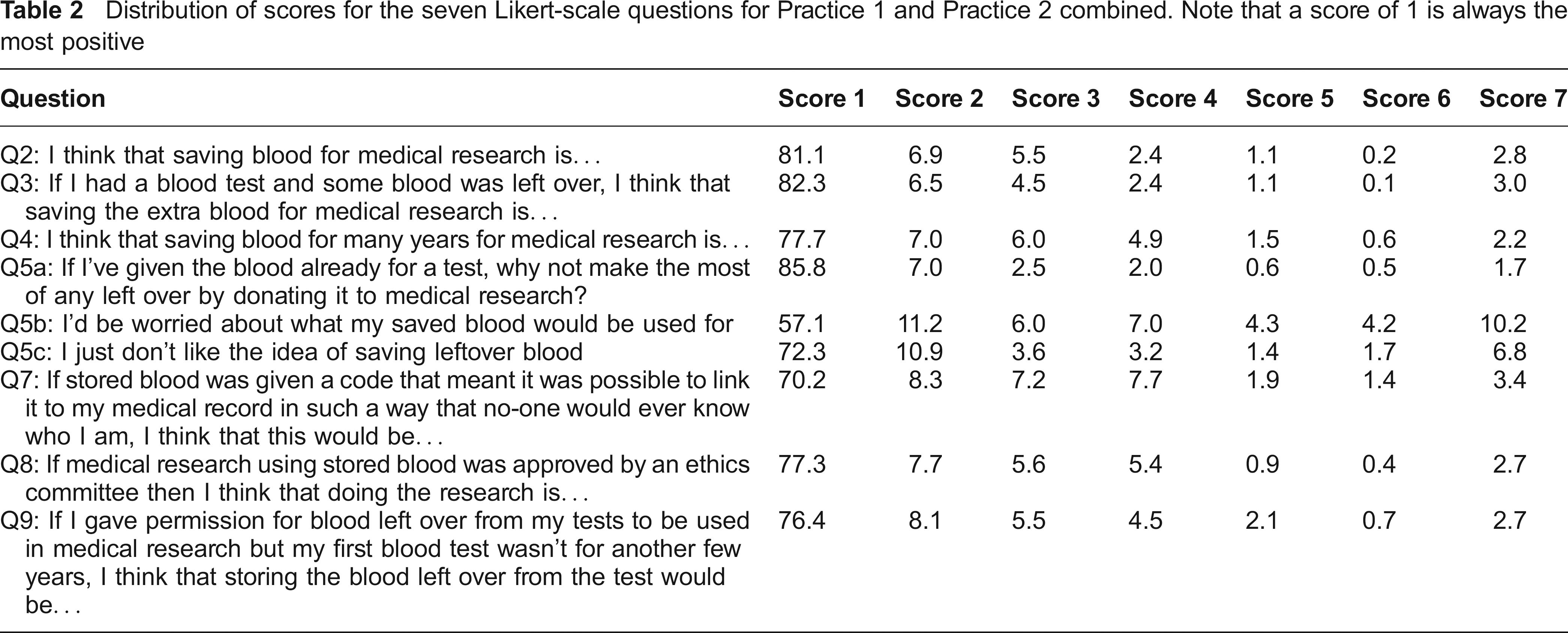
Mann-Whitney tests comparing scores for each Likert-scale question at the two practices did not show any significant differences (P > 0.19 for all questions). Table 2 shows the distribution of scores for the seven Likert-scale questions for the two practices. The most positive score (a score of 1) on the scale was used by 82% of respondents when asked how they felt about saving blood leftover from clinical tests for research (Question 3 on the questionnaire). The majority of respondents replied positively to these questions although there was some concern regarding the potential use of the stored blood (Question 5b). Table 3 shows the proportion of respondents considered unequivocally positive to storing leftover blood (ie. they scored less than four for all questions). There was a significant association between practice and being unequivocally positive, with respondents from Practice 2 being more positive (P = 0.029).
Distribution of scores for the seven Likert-scale questions for Practice 1 and Practice 2 combined. Note that a score of 1 is always the most positive
The proportion of respondents considered to be unequivocally positive to the storing of leftover blood (i.e. they scored less than 4 on all Likert-scale questions). Respondents’ preferences for the organization storing the blood are also given
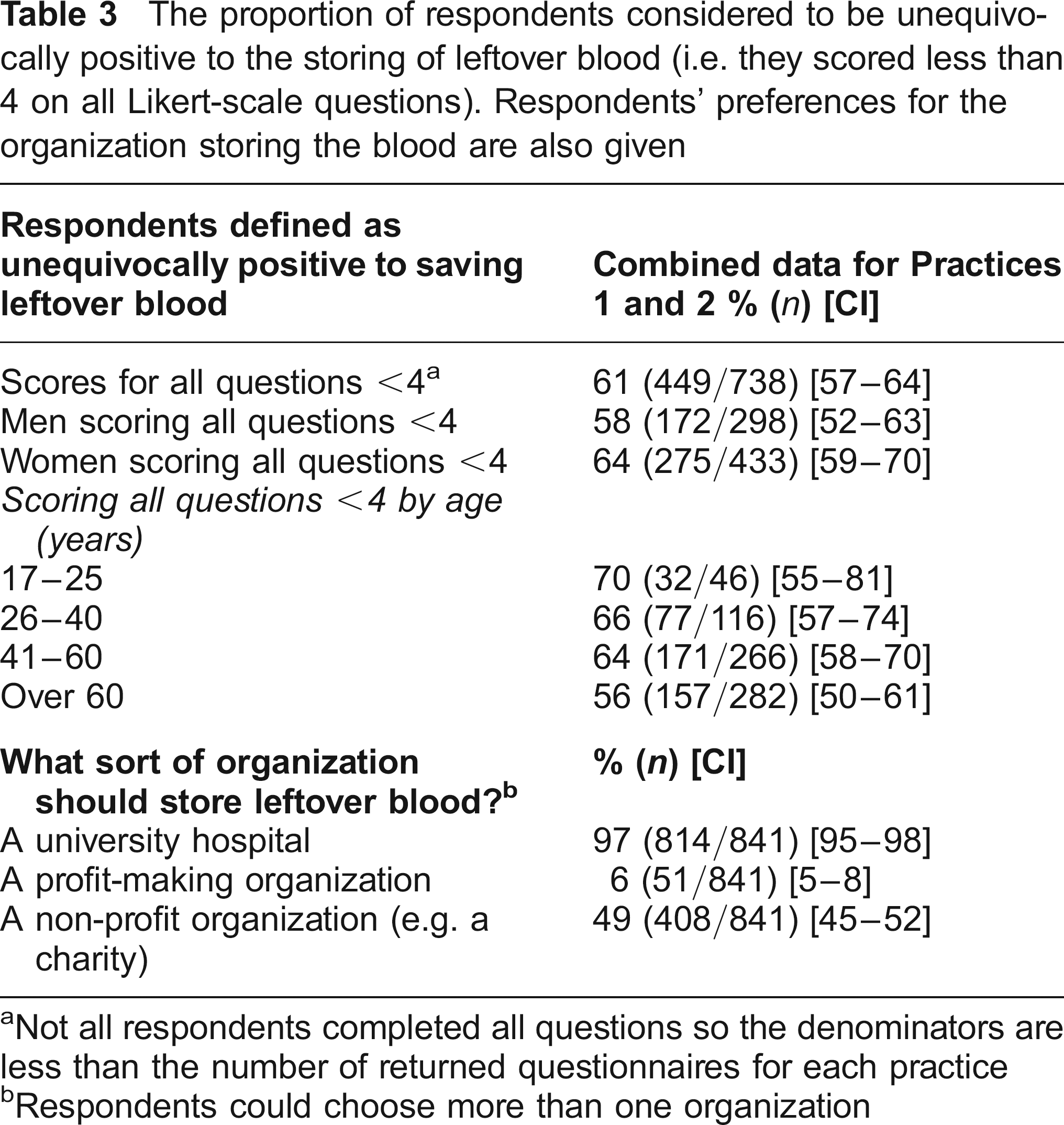
Not all respondents completed all questions so the denominators are less than the number of returned questionnaires for each practice
Respondents could choose more than one organization
The logistic regression showed that age and practice were significant predictors of whether respondents were unequivocally positive (P = 0.013 for age and P = 0.034 for practice; sex was not a significant predictor, P = 0.089). In short, increasing age and being from Practice 1 reduced the likelihood that a respondent would be unequivocally positive to saving leftover blood. The vast majority of respondents, 97% (95% confidence interval [CI] = 95–98%) felt comfortable with a university hospital managing the storage of leftover blood, while only 6% (95% CI = 5–8%) were comfortable if a for-profit organization were managing the same information (Table 3).
Space on the questionnaire allowed respondents to provide free-text comments and 171 individuals chose to do this (Table 4). Just over half of the comments were positive statements about medical research in general and/or the project, while about 10% were critical of the questionnaire itself. Misuse of stored blood was a worry for some and the involvement of for-profit organizations attracted criticism, which reflects the results shown in Table 3.
A sample of respondents’ free-text comments
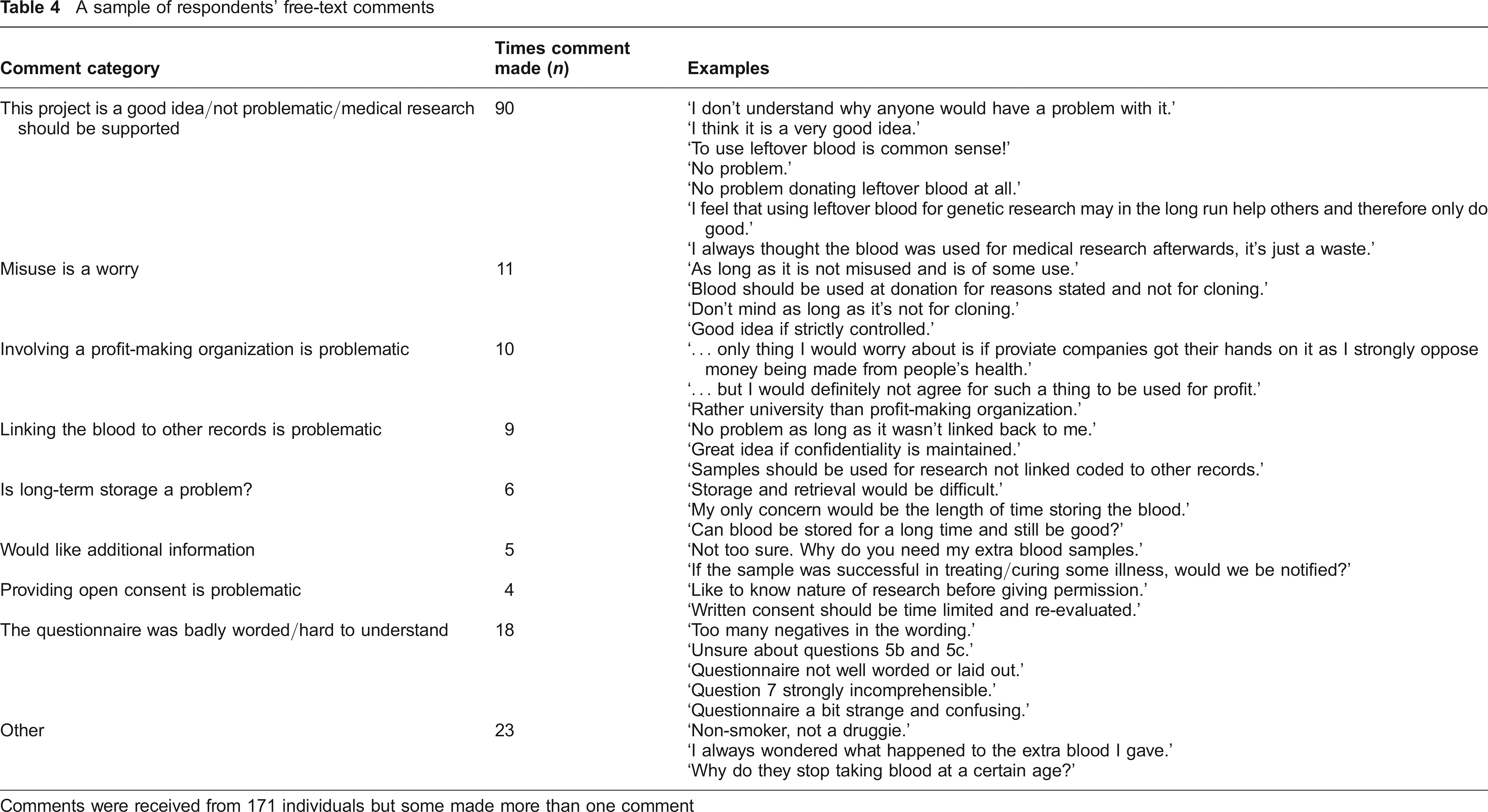
Comments were received from 171 individuals but some made more than one comment
Discussion
The majority of those completing the questionnaire considered saving and using leftover blood for future medical research to be unproblematic, including linking the sample to their medical records. Indeed, with the exception of one question, at least 70% of respondents selected the most positive response to the question on the seven-point scale (Table 2). This broadly favourable attitude is similar to recent work with health care professionals. 1 The exception was a question about what the blood would be used for in the future, but even here 57% of respondents chose the most positive response. Respondents were clear in rejecting for-profit organizations as potential custodians of saved blood. Other studies asking patients and the public about hypothetical donation have also found some wariness about commercial organizations,12,15,16 although studies involving a real donation or consent decision have found participants to be less concerned.17,18 This is encouraging for DNA biobanks since many do involve commercial partners. If potential donors are given adequate information, donating tissue to research involving commercial organizations does not appear to be contentious. 18
Older respondents tended to be more reluctant to save leftover blood, which contrasts with other studies that either found no difference8,19 or found older people more likely to participate.12,20 It is not clear why our study differs from these earlier studies. It may be that older Scottish people are more cautious about taking part in research, or are less informed of the potential benefits. The difference may be less important than it appears; a majority of respondents aged over 60 years (56%) were still unequivocally positive to saving leftover blood and the confidence intervals for the age data in Table 3 overlap.
The TPB 13 provides a theoretical framework for measuring an individual's attitude towards a particular behaviour. The direct measures of attitude we used from the TPB manual are generic and can be used with a range of behaviours. This has two advantages. First, questionnaire items are easy to develop, as the same format can be used for a range of behaviours. Second, responses with respect to different behaviours are directly comparable. For these reasons we chose to use questions based on the TPB. There has been criticism of this theory, particularly that it cannot be tested and that it fails to explain sufficiently the variance in intention or behaviour. 21 Azjen and Fishbein have robustly defended the theory, 22 while a meta-analysis of 185 studies found that the theory accounted for 27% and 39% of the variance in behaviour and intention, respectively. 23 Attitude alone accounted for 24% of the variance in intention. 23 Before the introduction of reasoned action models such as the TPB, most studies accounted for 10% or less of the variance in behaviour. 22 Moreover, the closely related theory of reasoned action has predicted intention to donate, albeit of bone marrow rather than leftover blood. 24
The study has limitations. Some respondents did not fully understand the questionnaire (Table 4). Of the 171 free-text responses, 18 were critical of the questionnaire. We speculate that the format of the TPB questions was sufficiently unfamiliar to cause some confusion. Although the format was based on a large body of research (see http://www.rebeqi.org/?pageID=34&ItemID=72), we underestimated its novelty for many people. So, while we believe the use of the TPB to be reasonable, our experience suggests that the use of the TPB manual format in mailed questionnaires should at the very least provide a clearer explanation of how to complete questions than was given in our questionnaire. The study would have benefited from a pilot and researchers considering mailed TPB questionnaires are encouraged to run one.
To guarantee anonymity, we chose not to add identifiers to questionnaires, which meant that we could not send reminders to non-responders. This was expected to affect the response rate 14 and the number of individuals to whom we sent a questionnaire was calculated with this in mind. Surveys similar to ours that achieved higher response rates (e.g. Kettis-Lindblad et al. achieved 49.4%, 12 Wong et al. 70% 8 ) did use reminders, in some cases as many as three. We received fewer completed questionnaires for Practice 1 than the 400 for which we aimed; correspondingly, our study is somewhat underpowered for detecting differences between practices. The actual power for the comparison used in the sample size calculation is 0.54 rather than the customary 0.80. Although the lack of power was unproblematic for our primary comparison between practices of those unequivocally positive to donating leftover blood, it may hide other differences.
An advantage of the study was that it involved two practices with different types of patients, with almost two-thirds of patients from one practice coming from postal addresses falling into the most deprived quintile of the Scottish Index of Multiple Deprivation (see http://www.scotland.gov.uk/Topics/Statistics/SIMD/Overview). Despite a lower response rate from this practice, and a tendency for patients to be more conservative about saving leftover blood, most respondents did favour storage. This message was so strong (Table 2) that we believe our study identified a generalizable attitude and we are confident that a larger sample would produce similar results, at least in Scotland. Our data show that it will be harder to recruit people living in more deprived areas to DNA biobank studies. The current study implies that postal surveys of individuals from deprived areas should compensate for a response rate that could be 15–20% lower than that from less deprived areas.
Much of the debate around DNA biobanks relates to consent; specfically, a major question revolves around obtaining open-ended consent. The results of studies investigating the views of the public in this regard have been equivocal, with some finding respondents in favour of open-ended consent17,25–27 and others against.28–31 Hoeyerand colleagues found that, although 67% of participants were willing to let an ethics committee decide whether to approve new research without contacting donors, 48% said they would, nevertheless, appreciate being asked. 32 While linking samples to medical records seems essential to maximizing the benefit of DNA bio-banks, obtaining specific consent to do so may pose a problem. Even in studies that found generally positive attitudes to donating material, a large number of participants would not be willing to allow researchers to access medical records without permission.15,32 Asai and colleagues concluded that the public has conflicting attitudes towards the need for specific consent, with some donors willing to give open consent while others require consent for each new use. 33
Those responding to our survey were generally relaxed about donating leftover blood, including linking samples to medical records (Table 2). This is encouraging for those working with DNA biobanks. Tayside, where the study was based, has a long history of high quality epidemiological record linkage studies based on Scotland's Community Health Index, a unique patient identifier that has been used in Tayside for 20 years. Similar linkages will eventually be possible throughout Scotland and the UK through increased integration of health information systems. If the wider Scottish and British public are as positive about this linkage as our study suggests, it should be possible to successfully combine DNA samples with increasingly rich phenotypic information on very large numbers of individuals while ensuring the wishes and attitudes of donors are respected.
Conclusions
With regard to general attitudes, over 75% of our respondents believed that saving leftover blood for years was not a problem nor was using this blood in future research. Provided research is approved by an ethics committee, respondents also believed it was unproblematic to link medical records to genetic information as long as some protection against identification was made. Hansson and colleagues have argued for broad consent in biobank research; 3 the results of this exploratory survey suggest that many (though not all) members of the public, approached through their GP, would be willing to give this form of consent.
Ethical approval
Ethical approval for the study was obtained from the Tayside Committee on Medical Research Ethics.
Footnotes
Acknowledgements
We would like to thank Dr Debbie Bonetti, a psychologist at the Dental Health Research Unit, University of Dundee, for her help and advice regarding the Theory of Planned Behaviour. This study was funded by the East of Scotland Primary Care Research Network (EastRen) grant number 95-03.