
Abstract
Objectives:
The principles of evidence-based practice (EBP) are fundamental to medical ethics and seem essential for any form of health care. In 2000, a House of Lords Select Committee recommended that the ethos of EBP should extend to complementary and alternative medicine. The aim of this investigation was to determine whether EBP is incorporated in the codes of ethics of British complementary and alternative medicine organizations.
Methods:
We obtained the codes of the following bodies: Association of Naturopathic Practitioners, Association of Traditional Chinese Medicine (UK), Ayurvedic Practitioners Association, British Acupuncture Council, Complementary and Natural Healthcare Council, European Herbal Practitioners Association, General Chiropractic Council, General Osteopathic Council, General Regulatory Council for Complementary Therapies, National Institute of Medical Herbalists, Register of Chinese Herbal Medicine, Society of Homeopaths, UK Healers, Unified Register of Herbal Practitioners. We then extracted the statements referring to EBP and compared this with what the respective codes of British doctors and nurses proscribed.
Results:
Only the General Chiropractic Council, the General Osteopathic Council and the General Regulatory Council for Complementary Therapies oblige their members to adopt EBP.
Conclusions:
This discloses double standards in UK health care which may compromise patient safety.
Introduction
Complementary and alternative medicine (CAM) continues to attract considerable attention from patients, the medical community, the media and the general public. A British survey suggested that 20% of people had used CAM in the previous year 1 and even higher estimates have been noted in the US. 2 Moreover, CAM use seems to be increasing. A US study suggested a 10% rise in one year prevalence of use between 1990 and 1997. 3
Despite the absence of a sound evidence base for many types of CAM, 4 there has been an increase in commissioning by the National Health Service (NHS) in the UK and provision of CAM by NHS Trusts including in cancer. One in three general practices are currently making acupuncture available for their patients and more than one in four make osteopathy and chiropractic available. 5 Furthermore, there are four NHS homeopathic hospitals treating 55,000 patients a year referred by GPs, Primary Care Trusts and NHS specialists at an annual cost of £6 million, 6 even though the results of a systematic review of systematic reviews reported that homeopathy is no more effective than placebo for any condition. 7
Given this uptake of CAM services by the NHS, and that evidence-based practice (EBP) is a fundamental concept in health care and one of the seven pillars of clinical governance, it may seem fair to assume that all services provided to patients by the NHS should be delivered according to current and up-to-date evidence. EBP ‘requires that decisions about health care are based on the best available, current, valid and relevant practice’ 8 and the codes of ethics of most (if not all) conventional health care professions have enshrined an obligation for EBP. The General Medical Council's Good Medical Practice, for instance, states that doctors ‘must provide effective treatments based on the best currently available evidence, 9 and the Nursing and Midwifery Council's Standards of Conduct, Performance and Ethics points out that members ‘must deliver care based on the best available evidence or best practice’. 10
A House of Lords select committee recommended that this ethos should also extend to CAM and that CAM practitioners should have a good understanding of the principles of evidence-based health care. 11 Our aim was to determine to what extent EBP is incorporated in the codes of ethics of several CAM professions in the UK.
Methods
We studied the codes of ethics of 14 major UK organizations and regulatory bodies of CAM practitioners: acupuncturists, aromatherapists, Ayurvedic practitioners, chiropractors, healers, homeopaths, massage therapists, medical herbalists, naturopathic practitioners, osteopaths, reflexologists and traditional chinese medicine practitioners. Organizations were included if they represented the majority of UK therapists within that profession or were cited in the Department of Health Steering Group on the Statutory Regulation of CAM Practitioners as appropriately operating a voluntary code and demonstrating good practice with regard to protecting the public. 12 In addition, the newly established Complementary and Natural Healthcare Council 13 was also included because it is supported by the Department of Health and the Prince's Foundation for Integrated Health. We extracted the information relating to EBP. As reference groups, we used the information provided in Good Medical Practice 9 for doctors and Standards of Conduct, Performance and Ethics 10 for nurses.
Results
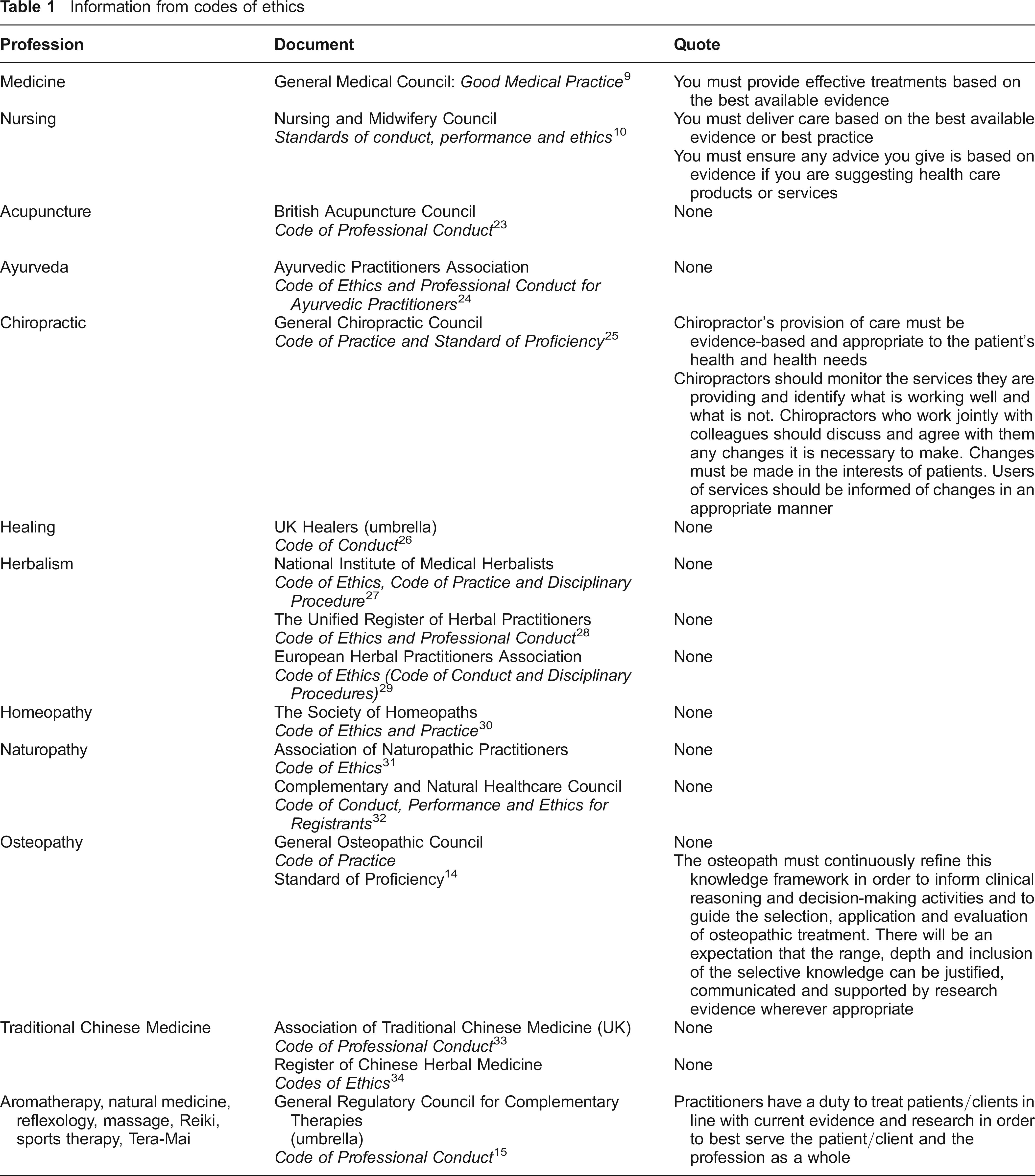
The majority of British CAM providers are not obliged through their codes of ethics to adhere to EBP (Table 1). However, there are several exceptions. Chiropractors are formally required to use an evidence-based approach to practice. For osteopaths, this recommendation is less explicit though evidence is viewed as part of the ‘knowledge framework’ 14 of the profession. The General Regulatory Council for Complementary Therapies (GRCCT) which represents practitioners of aromatherapy, natural medicine, reflexology, massage, Reiki, sports therapy and Tera-Mai also emphasizes the duty to treat patients ‘in line with current evidence and research’. 15 However, the codes of ethics for the other organizations do not require their members to work within an evidence-based practice framework.
Information from codes of ethics
Discussion
For most CAM professionals, there is no obligation to adopt the principles of EBP. The General Chiropractic Council, the GRCCT and to some degree the General Osteopathic Council are the exceptions. Although osteopaths and chiropractors are statutorily regulated in the UK, the code of conduct of the former does not explicitly insist on EBP. The Osteopathic Standard of Proficiency 14 acknowledges research evidence but does not emphasize its importance as a culture of care delivery.
The newly established Complementary and Natural Healthcare Council 13 also fails to oblige members to engage in EBP. In fact, its Code of Conduct, Performance and Ethics for Registrants only requires members to ‘provide the treatment or advice if you believe this is appropriate’, ignoring the tenets of EBP. This is surprising given that a House of Lords Select Committee recommended that the ethos of EBP should extend to CAM and that the Council has the support of the DH. Given this absence of EBP, the Council objective to establish itself as ‘the quality benchmark for NHS referrals’ is concerning.
We believe that the discrepancy between conventional and CAM organizations points to double standards in UK health care which may compromise patient safety. We have shown previously, for instance, that advice offered by British acupuncturists, medical herbalists and homeopaths failed to be evidence-based, often to the extent of constituting a risk to patients.
UK chiropractors are in theory obliged by General Chiropractic Council standards to adopt EBP. However, there is evidence that this does not always happen in practice. Despite the existence of little compelling evidence to support the use of chiropractic for non-spinal conditions many chiropractors seem to advocate spinal adjustment for visceral conditions. Indeed, their council website states that chiropractic is an effective treatment for asthma and in one study, 72% of a sample of UK chiropractors advised their clients to use chiropractic as a treatment for asthma. 16 Yet a systematic review found insufficient evidence to support this claim. 17
Similarly, the statement by the GRCCT that all registrants ‘have a duty to treat patients/clients in line with current evidence’ 15 seems at odds with the claims made by practitioners represented by this organization. A survey of British CAM organizations reported that practitioners of magnet therapy, Reiki and yoga advocated their therapies for cardiovascular conditions, including high blood pressure and circulatory conditions. Other practitioners maintained that aromatherapy and reflexology can benefit patients with HIV/AIDS. 18 Again there is no sound clinical evidence to support such claims. 4
The absence of EBP also seems to impact on the information supplied to the public. Several analyses of CAM websites showed that misinformation about the efficacy of certain CAM treatments for serious conditions such as cancer, AIDS or depression was common. 19 Given that patients increasingly rely upon the mass media as their primary source of health information and more than 30% of Internet users are looking for information on CAM, 20 this situation means that patients’ health may be put at risk.
A recent DH report 12 has recommended statutory regulation of acupuncturists, herbalists and traditional Chinese medicine practitioners through the Health Professions Council in an attempt to standardize education and care in order to safeguard the public from poor practice. Part of this report included a draft Standards of Proficiency for each of those professions, stating that registrants ‘must be able to practise evidence-based practice, evaluate practice systematically, and participate in audit procedures’. 11 Insisting on EBP is essential for public protection because of the inextricable links between effectiveness and safety. However, because the evidence for these complementary medicines is incomplete and for some conditions negative,5,17 if EBP were to be adopted then CAM practitioners such as acupuncturists and chiropractors would have to discontinue treating conditions for which the evidence is negative.17,21 However, this could, in time, be beneficial for CAM practitioners by creating pressure to conduct rigorous research testing the efficacy of CAM and thus, potentially, increasing the scope of practice for those professions.
The recommendation for a greater emphasis on EBP in CAM issued by a House of Lords select committee in 2000 is commendable. 11 However, the concept and process of EBP needs to be both taught and learned. Currently, EBP is not a core component of most CAM training programmes and the opportunity to learn the principles of EBP post-qualification is extremely limited. One UK study was unable to find any courses on EBP and research methods for CAM practitioners in one region. 19 Thus, fewer CAM practitioners consider EBP to be essential to their practice or identify a need for further training in EBP than allied health practitioners. 22 Provision of EBP courses should be the responsibility of the CAM professional and regulatory bodies.
In conclusion, the codes of ethics of many UK CAM organizations do not oblige members of these organizations to adhere to the principles of EBP. This discloses overt double standards in UK health care which may compromise patient safety. In the interests of everyone concerned, we should work towards establishing a single standard throughout health care.