
Abstract
Ethnographic studies are valuable in studying patient safety. This is a narrative review of four reports of ethnographic studies of patient safety in UK hospitals conducted as part of the Patient Safety Research Programme. Three of these studies were undertaken in operating theatres and one in an A&E Department. The studies found that hospitals were rarely geared towards ensuring perfect performances. The coordination and mobilization of the large number of inter-dependent processes and resources needed to support the achievement of tasks was rarely optimal. This produced significant strain that staff learned to tolerate by developing various compensatory strategies. Teamwork and inter-professional communication did not always function sufficiently well to ensure that basic procedural information was shared or that the required sequence of events was planned. Staff did not always do the right things, for a wide range of different reasons, including contestations about what counted as the right thing. Structures of authority and accountability were not always clear or well-functioning. Patient safety incidents were usually not reported, though there were many different reasons for this. It can be concluded that securing patient safety is hard. There are multiple interacting influences on safety, and solutions need to be based on a sound understanding of the nature of the problems and which approaches are likely to be best suited to resolving them. Some solutions that appear attractive and straightforward are likely to founder. Addressing safety problems requires acknowledgement that patient safety is not simply a technical issue, but a site of organizational and professional politics.
Introduction
The importance of ethnographic studies of patient safety has been evident since a series of reports published in the US during the 1970s, including the classic texts by Charles Bosk and Marcia Millman.1,2 However, it is mostly only in the last decade that a coherent body of ethnographic work on patient safety has been begun to emerge in the UK, including work funded through the national Patient Safety Research Programme (PSRP).
This article presents a critical overview of the final reports3–6 of the four PSRP studies that included substantial ethnographic elements. The primary aim of this review was to identify key empirical findings from the studies, with a view to recognizing common issues across different settings, and offering an interpretation that could help deepen understanding of problems in patient safety.
A wide variety of techniques may be used in conducting such an overview. 7 In this article, a narrative review has been attempted. This allowed for use of traditional social science skills of organizing the literature into what appeared to be useful thematic categories, using knowledge of the wider relevant literature to identify aspects of the findings that seemed to be of special interest or value, and drawing on reflexive, interpretive skills to offer commentary. 8
The studies
The four studies that were the subject of the reports had been conducted in four separate settings, by different types of people, using different approaches (Table 1). Three were conducted in operating theatres3–5 and one in an accident and emergency (A&E) department. 6 The studies used different types of observers and methods of data collection and interpretation. The skills and backgrounds of the different observers meant that the studies attended to and emphasized different aspects of the clinical situations in which they were located. But all confronted the challenge of how to classify events as patient safety incidents, and how to determine the relevant contributors to these incidents. This is an important methodological challenge, but it also draws attention to how ethnographic work in patient safety is always likely to be engaged in normative judgements about how things ought to be, as well as describing how things are. Here, I present five normative aspirations that I felt the authors of the study reports were using to guide their judgements of what they saw, and comment on the implications of what the studies found.
Characteristics of studies included in review
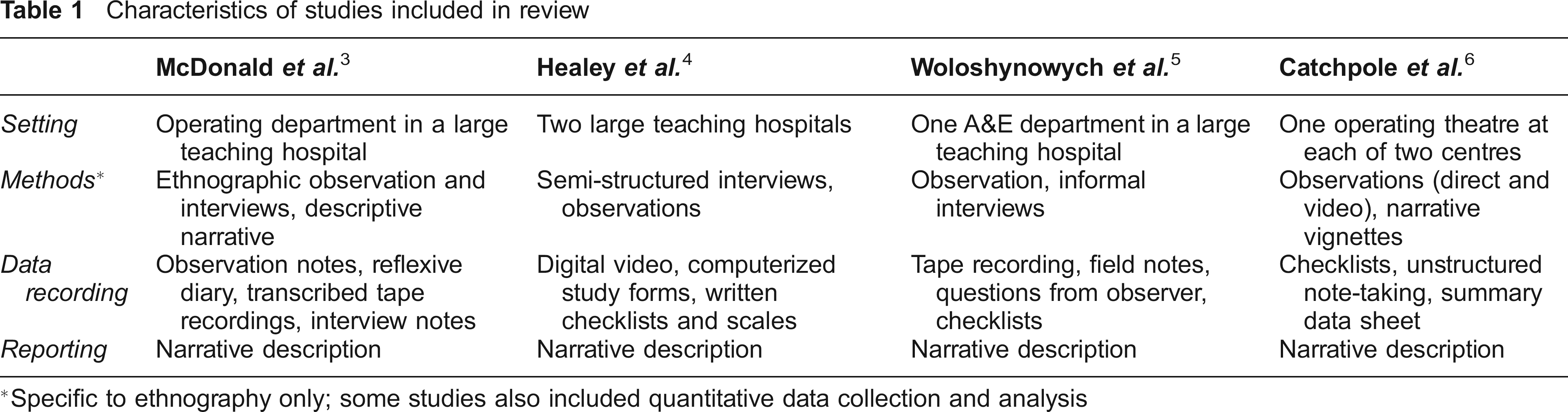
Specific to ethnography only; some studies also included quantitative data collection and analysis
Aspiration 1: The organization should be geared to promoting safety
The idea that health care organizations should be geared towards promoting safety lies at the heart of the ‘systems’ 9 approach to patient safety. In the study reports, there was considerable evidence that hospitals were rarely geared toward perfect performances; rather, organizational limitations functioned to continually erode the buffers of safety. Many activities that staff aimed to undertake were dependent on elaborate, complex, highly interdependent networks and processes.
Changes or delays to planned procedures were extremely common (occurring in 71% of cases in Healey et al.'s study). Critical information and supplies were not always there when needed. The surgeon and the anaesthetist, as well as other key characters, were not always available when the operation was scheduled to start, and they were sometimes summoned or diverted elsewhere even after it had begun. Much depended on the performance and integration of parts of the hospital external to the operating theatre. A tiny default somewhere along the line – a porter being unavailable at the right time to take a patient to theatre, for example – could easily have huge knock-on effects, disrupting schedule and flow for the rest of the day, and increasing risks for patient safety. Managerial attempts to deal with some of these problems sometimes seemed ineffectual or poorly fitted to the underlying difficulties – for example, providing data on over-runs in the operating theatre schedule did little to address the underlying difficulties, but may have reinforced the sense that staff at the sharp end were being left to put up with the consequences of a system that inadequately supported their work. But other problems, such as ensuring that equipment could easily be reached during surgery, were internal to the operating theatre, and at least in principle more directly within the control of the theatre staff.
An important consequence of the level of environmental strain was that staff evolved strategies and routines to work around problems, often coping by treating problems as ‘normal’. This supported the development of internal cultures that allowed workers to get jobs done. 10 But the tactics or shortcuts used were prone to causing other problems in the system – for example, surgeons turning up late, on the assumption that the operation would be delayed, could itself cause delays. Moreover, though staff learned to tolerate organizational turbulence, they were often, as a result, engaged in retrieving and rescuing situations that had gone wrong. These rescues were often (even usually) successful, and this may have four important consequences.
First, the ‘ability to rescue’ may become institutionalized as a way of adapting to environmental strain, but is a precarious defence against patient safety threats, and may be especially fallible when staff are inexperienced or poorly-skilled. Second, being able to repair problems as they occur may mean that staff came to tolerate and regard as ‘normal’ the kinds of conditions that are undermining of safety. There was evidence in the study reports of a culture of judging whether something was a patient safety incident not by whether the process had been optimally executed, but by whether any long-term negative consequences became known to the team. A third, rather perverse, consequence was that the ability both to tolerate adverse conditions and to rescue calamities became part of the performance of professional identities: it could, for example, become important to surgeons that they were recognized as heroic characters who could operate under trying circumstances but still pull back from disaster. These adaptations and tolerances contributed to problems being made invisible – unless problems erupted into catastrophe, there was little incentive to either recognize them explicitly or address them. Finally, lack of strong organizational support made available justifications for things going wrong; skipping checks, for example, could be blamed on the need to rush because of delays.
Aspiration 2: Communication and teamwork should be optimal
The study reports identified that surgical performance was heavily influenced by variation in teams, and that poor communication may lead to surgical error and poor coordination of tasks. Operating theatre professionals often complained that their colleagues did not understand their priorities or seemed to be pursuing conflicting goals, and there was disagreement between professional subgroups about the structure of surgical teams. Communication and teamwork problems meant that basic procedural information was not always shared. Operations often began before all the team members were ready (35% of cases in Healey et al.'s study) while verbal communication confirming antibiotics was observed in only 53% of cases. Frequent problems were observed to occur in the distribution of important information within the surgical team, and in the timely execution of procedural sequences requiring interaction between individuals, as did difficulties in the planning of operations and anticipation of problems. Catchpole et al., for example, found that teams often did not plan the required sequence of events, identify potential or expected threats, or agree in advance on avoidance or mitigation contingencies.
There were several reasons why formal attention to issues of communication and teamwork seemed to be regarded as non-essential by staff. It was usually possible for staff to compensate and ultimately overcome the problems caused by teamwork and communication deficiencies. There was an apparent perception that communication and teamwork were non-technical skills that did not need to be formally learned, but rather would emerge naturally in the course of normal interaction. ‘Implicit teamwork’ describes the kind of team working that tends to rely heavily on local and individual familiarities, but this is a highly fallible defence against failings, especially when teams cannot be guaranteed to be identical from one procedure to the next.
Teamwork problems were also associated with professional boundaries and hierarchies. Professional allegiances and identities appeared at times to exert more influence over behaviour and practices than did team allegiances. This meant, for example, that it could be difficult for those junior or less privileged in the hierarchy to draw attention to problems; they were too deferential. On the other hand, as discussed later, those who appeared to occupy the same plane in the hierarchy sometimes refused to defer to colleagues, with other negative consequences.
Aspiration 3: Practitioners should do the right things
All study reports identified that that staff did not always do things as they should be done, and that patient safety risks were introduced as a result. Examples included: equipment not being prepared, checked or in the right place; failing to undertake blood loss analysis; not managing perfusion correctly; not wearing masks or eye protection during operations; not maintaining proper standards of hygiene; omitting key surgical steps; starting procedures without everyone in the team being aware or ready, and without all the equipment and supplies being checked and in place; not reading back during instrumentation checking; not completing swab checks; and violating aseptic procedures.
These different practices describe a wide variety of different deviations from what might be expected as the ideal. They include deviations which may be quite purposeful (such as not wearing masks even in response to a direct instruction) as well as those which are quite clearly mistakes (such as unintentionally omitting surgical steps). In between, there may be many actions that escape consensus as to whether they constitute patient safety lapses or legitimate differences in professional opinion. It was also evident that many practices or norms may evolve because they are adaptive, enabling groups to get things done in the face of organizational frustrations or other pressures, even if things are not done perfectly. When this happens, the risks to patient safety may increase, but the group may remain unaware of the problems, or may perpetuate social mechanisms that prevent it from acting on the problems (such as chiding people who appear to be causing delays by undertaking checks).
The studies provided important data on the troubles associated with deploying formal rules for patient safety in an effort to get staff to do the right things. Rigid and literal adherence to rules may sometimes be used by professionals as a way of displaying a ‘good’ professional identity or avoiding censure, but at the same time undermining the effectiveness of the rule in achieving the desired objective. McDonald et al. illustrate this with the example of the nurse who wrote everything used during the operation on a whiteboard – but after the operation had been completed, when the information was redundant. On the other hand, breaches of official rules such as protocols may sometimes be justified by practitioners (perhaps especially doctors) by appealing to the particular nature of professional discretion. Narratives of absurdity were often used to great effect in such arguments; McDonald et al. report an anaesthetist's story of delays in transferring a patient for urgent neurosurgery that occurred because a minor piece of equipment required by the protocol was unavailable.
Aspiration 4: There should be proper structures of authority and accountability
Having clear, well-functioning structures of authority and accountability is important for many reasons. The study reports suggested that responsibility for patient safety was, however, often confused, with much variation in levels of discipline. There was some evidence of a generalized laxness of control, evident in the high number of distractions that seemed to be routinely tolerated. Woloshynowych et al. reported that the nurse-in-charge in A&E was interrupted on 41% of occasions, while in Healey et al.'s operating theatre study, total counts of ‘interference events’ per case ranged from 1 to 39, with a mean of 13.56. Such events included door opening (occurring on average twice every three minutes), some of it associated with staff appearing to treat the operating theatre as a thoroughfare. The ‘theatre-in-use’ lights were never seen to be used, and people came in and out frequently. A lot of noise, including ‘case-irrelevant conversation’, phone calls and pagers, and interruptions by other staff occurred in the operating theatres. Other distractions in theatre included case-irrelevant reading material (such as newspapers) and (perhaps more legitimately) demands for teaching. Some interruptions occurred during parts of the procedure that were particularly vulnerable to interference, such as equipment counts and mixing of bone cement. Yet they seemed to be poorly controlled, and indeed there was evidence that senior staff themselves were major contributors to distractions.
The study reports further identified that how commitments to safety might be demonstrated or enforced was uncertain. There appeared to be some difficulties in identifying who was in charge in the operating theatre, on what authority and with what powers. Senior team members appeared to experience challenges in getting some colleagues to adhere to protocols and standards. Again, the extent to which practitioners felt they had to comply with formal protocols seemed directly linked to issues of professional identity. Problems in securing compliance seemed especially likely to occur between senior doctors of the same rank. Catchpole et al., for example, describe an individual entering a theatre during a procedure, having a loud argumentative phone call and then leaving again while violating mask protocol, without being corrected. Similarly, consultants in anaesthesia sometimes defied protocols on mask use, even when explicitly asked to do so by consultant surgeons.
Aspiration 5: Patient safety incidents should be reported
The idea that patient safety incidents should be reported is widely promoted in order to promote organizational and individual learning. The National Patient Safety Agency (NPSA) defines such an incident as any unintended or unexpected incident which could have or did lead to harm for one or more patients, and seeks notification of such incidents (including near misses). Across the studies there was considerable evidence that only a minority of incidents were reported. The reasons for this were multiple and complex. First, the formal NPSA definition may fail to capture the ways in which people classify and respond to risks and actions at the sharp end of practice. McDonald et al., for example, found that staff agreed on the importance of safety in principle, but a shared perception of what constitutes safe practice was lacking; different groups had different views about adverse events, risk and error reporting. Second, there was evidence of a fatalistic approach to some types of error; some types of problems were seen to be unavoidable and/or specific to individuals. Reporting mistakes was therefore not regarded as a valuable exercise, since, as one surgeon put it, there was nothing for anyone else to learn from his being distracted by the scrub nurse's legs. Third, some errors were considered too minor (and possibly ‘too normal’) to be reported. Fourth, organizational support for the process was often deficient. Procedures for managing reported incidents were poorly enacted by both management and practitioners: data were not always collected in the right form; it was not clear to staff how the information would be used by the trusts, directorate, or management; and there were concerns that reporting incidents would have negative consequences for individuals. In the A&E study, there were some examples of positive action in response to incident report, but there was also evidence of inconsistent use of categories, incomplete reports, missing information, and feedback not being given to the person who reported the incident. In the other studies, there was a view that little happened even when complaints were reported. Fifth, other reasons for not reporting incidents in the operating theatre included the ‘heroic’ model of surgery discussed earlier, where surgeons believed they should be able to cope with anything. They may therefore resist efforts to examine problems, especially when their own rescues repeatedly compensate for any failings. Finally, it was unclear who should do the reporting; issues of professional scope and role may influence who feels they may legitimately report or act on a possible incident. It was difficult to individuals to suggest or facilitate improvements, or even to identify a forum in which this might take place. There was also evidence that subordinates in the hierarchy could be fearful of questioning senior members of teams.
Discussion
Ethnographic studies in hospitals provide valuable insights into why patient safety is so hard. Considering as a corpus the four study reports from the ethnographic studies conducted as part of the PSRP yields perspectives and insights into the challenges of patient safety that are less evident when the reports read separately. The reports identify the multiple interacting influences on safety, and demonstrate the need for solutions to be based on a sound understanding of the nature of the problems and what kinds of approaches are likely to be best suited to resolving them. Such an understanding requires insight into the complexities of the networks in which hospital workers are embedded, and of how alternative conceptions of what is ‘safe’ or ‘good practice’ may prevail, conditioned by coping with competing priorities, clinical uncertainties, organizational pressures, resource inadequacies and efforts at professional boundary maintenance. The studies also show how easily pathologies that threaten safety can emerge in such circumstances, but be rendered invisible or ‘normal’. Efforts to improve safety need to be designed to take account of the realities of practice and based on an understanding of the logics people are using to inform their practices.
It is especially important to recognize the extreme complexity of these systems and the risk that ‘solutions’ that appear straightforward and appealing may themselves cause problems. The anaesthetist who refuses to wear a mask requires a different approach to the team rushing to catch up on delays, but all solutions need to be highly sensitive to context, fitted to the problems they are trying to solve, unlikely to result in unwanted consequences and accepted as legitimate. Interventions need to enjoy broad organizational support rather than being targeted solely at the sharp end; there are real dangers in assuming that professional rule-breaking is necessarily the result of failures of docility – though it may be sometimes. Only a small number of the patient safety problems reported in these studies are capable of being easily defined and (relatively) easily addressed.
A common response to the discovery of the kinds of problems described in the reports is to propose the introduction of formal rules (such as checklists and protocols) to render practice more orderly and accountable. But while it may be relatively easy to identify normative aspirations for safety at the level of broad principle, converting them into formal standards in such a way as to deliver on the desired objectives is very hard for some types of problems. 11 The challenges can be illustrated by examining the problem of distractions. Distractions are problematic not just because they interfere with the proper execution of procedures, they can also be seen as degrading the overall environment for safety. Just as the broken window hypothesis argues that criminal behaviour is encouraged when even very minor infractions are tolerated, 12 it might similarly be argued that even trivial distractions are consequential for the overall climate of safety. Tolerate personal mobile phone calls, newspaper-reading, and people wandering in and out of the theatre, the argument might go, and the overall commitment to a perfect performance, and the sense that the process is well-controlled, are diminished. Formal rules on reducing distraction are, however, likely be extremely difficult to design in such a way that they are sufficiently inclusive, precise, and regarded as legitimate, and are also likely to be difficult to enforce. For example, a rule that the doors to operating theatres should not be opened more than once every five minutes on average provides a clear standard, but one that is unlikely to be effective. Such rules may be prone on the one hand to the problem of either over-compliance, with staff preoccupied with making ritualized displays of compliance, and on the other hand to being ignored or subverted because they get in the way of getting things done.
Formal rules are also most likely to be effective if they are supported by professional norms. The evolution of social norms oriented to safety is, however, prone to being obstructed by a number of distinct but overlapping problems. The studies showed that organizational fitness has a major impact in both obvious and more subtle ways. Risk-related reasoning and practices at the sharp end 13 were institutionally structured and heavily influenced by what was happening at the blunt end. Organizations that were unable to provide orderly, supportive environments, and that made staff at the sharp end balance too many competing priorities, shifted the emphasis to ‘getting on with things’. Sloppy practices tended to occur when practitioners were under pressure. Faced with much that was outside their control, teams functioned as communities of practice 14 that constructed safety from cultural referents, artefacts, rules and constraints that originated both inside and outside the formal boundaries of their organizations. 15 They controlled what they could control, got used to compensating, making do and taking shortcuts. This, combined with non-reporting of patient safety incidents, obscured recognition of problem seriousness both by staff themselves and by organizations. Checklists may then contribute to, rather than addressing, problems: if time and resource are diverted to checking and protocol routines, but the pressure is unrelieved, it is possible that problems will be displaced elsewhere in the system, and the consequences of this would need to be studied carefully. Moreover, the underlying problem of organizational fitness remains unresolved: checklists are likely to be properly effective only when organizational fitness is addressed at the same time.
The study reports also vividly identified problems of professional boundaries and teamwork. A reliance on tacit knowledge was evident, but for the uninitiated is risky 16 and prone to causing problems of coordination and communication. Teams continued to express a hierarchical logic, with doctors the dominant group 17 by virtue of their institutional positioning and their professional expertise. Training is proposed as a solution in some of the reports, but the overwhelming imperative to ‘just get on with it’ suggests that there may be considerable challenges in trying to encourage some staff to engage authentically in formal teamwork training.
The reports further suggested that claims of ‘clinical judgement’ are used strategically to legitimate nonconformity with rules. The role of clinical judgement in patient safety presents significant dilemmas. On the one hand, clinical expertise and discretion are clearly needed to avoid stupidities and risks associated with rigid rule adherence. On the other hand, claims of special knowledge and immunity from standardization can be self-interested. Generalized non-conformity can be understood as a way of performing a particular kind of professional identity and reinforcing occupational boundaries. Doctors may be especially prone to resist externally or managerially imposed protocols, and seek to display their autonomy and seniority by demonstrating that they are not docile, but rather are creative, intuitive and individual. A view that ‘rules do not apply to us’ may, however, easily become dysfunctional, extending to all kinds of areas where variations in professional judgement are irrelevant to the matter at hand, and used to legitimate or obscure poor practices. Thus, inertia about patient safety may serve certain professional interests: the most insidious form of power ‘consists of letting people whose business it is define what that business includes, which versions of it are serious and important, and which don't matter much'. 18
These are all hard problems. Addressing them will require an acknowledgement that many safety issues represent the working out of institutional logics that are often unrecognized by the insiders in organisations, yet external scrutiny may be resented and resisted. Patient safety is not simply a technical issue, but a site of organizational and professional politics.
Footnotes
Acknowledgements
The work on which this paper is based was funded by the National Patient Safety Portfolio and Mary Dixon-Woods' Fellowship under the ESRC's Public Services Programme RES-153-27-0009.