
Abstract
Objective:
To explore the maternity care experiences and expectations of United Kingdom (UK)-born ethnic minority women.
Methods:
Qualitative in-depth interviews with 34 UK-born mothers of Black Caribbean, Black African, Indian, Pakistani, Bangladeshi and Irish descent, recruited mainly from nine National Health Service (NHS) maternity units in England.
Results:
Overall, women felt that their ethnic background did not matter at all with respect to the care they received. UK-born women's familiarity with the system and the absence of language barriers were felt to be influential in getting treated the same as White women. Women stressed the need for professionals to be ‘sensitive’ and ‘delicate’ in their interactions and wanted ‘continuity of care’. In general, they were positive about the adequacy of the information given during their antenatal appointments, but some women found it difficult to get access to antenatal classes. Women valued good communication and consistent information, with their views acknowledged and their questions answered consistently. They also expressed the need for better physical environments in maternity units.
Conclusions:
Our findings contribute to the growing evidence about the need to improve maternity and postnatal care, and to develop more sensitive and women-centred care for all women irrespective of ethnic background.
Introduction
Policies for maternity services in the United Kingdom (UK) specify flexible services with a focus on the needs of individual women, especially those who are more vulnerable. In doing so, they call on maternity services to adopt a woman-centered approach to care that is accessible, efficient and responsive to changing local needs.1–3 Increasingly, health care policies emphasize the need to address ethnic diversity, while wider policy initiatives, such as the Race Relations Amendment Act 4 and the Department of Health's Race Equality Scheme 5 underscore the importance of creating a service responsive to diversity.
Research in the UK has shown that some women from ethnic minority groups have had poor experiences of maternity care6–9 and some groups are more likely than others to have poorer outcomes for mothers or babies,8,10 but most of the research has focused on women born outside the UK. Women born in the UK account for a substantial proportion of mothers in some ethnic groups, 11 but little is known about their experiences of care.
This paper describes maternity care experiences and expectations of UK-born women of Indian, Pakistani, Bangladeshi, Black African, Black Caribbean and Irish descent.
Key concerns of ethnic minority women in relation to access to maternity care
Most studies of foreign born ethnic minority women's maternity experiences in high-income countries, for example from Sweden and Australia, have reported language barriers and subsequent difficulties in communication.12,13 UK studies have often highlighted the linguistic concerns of recently arrived non-English-speaking women and the lack of adequate provision of language support services.7,9,14–16 For instance, a study of Somali refugee women in west London showed they did not get equal access to services because of inadequacies in interpreting services. 7 The prevailing assumption in maternity policies and practice in many parts of the UK has been that the population is White and English-speaking. 9
Effective communication, particularly between health care professionals and parents, is a fundamental prerequisite for quality in maternity care,3,1 but its importance seems to be underestimated in maternity care settings.8,15 Even without major language problems, poor communication can affect the care experiences of ethnic minority women. A study of the birth experiences of second generation South Asian Muslim women, educated in the UK, described the women being ‘muted’ by the midwives who neither listened to them actively nor gave them the opportunity to voice their needs. 16 Other difficulties reported by ethnic minority women include interpersonal issues with professionals arising from staff stereotypes, racism and cultural barriers.6,7,9,14,16,17
Methods
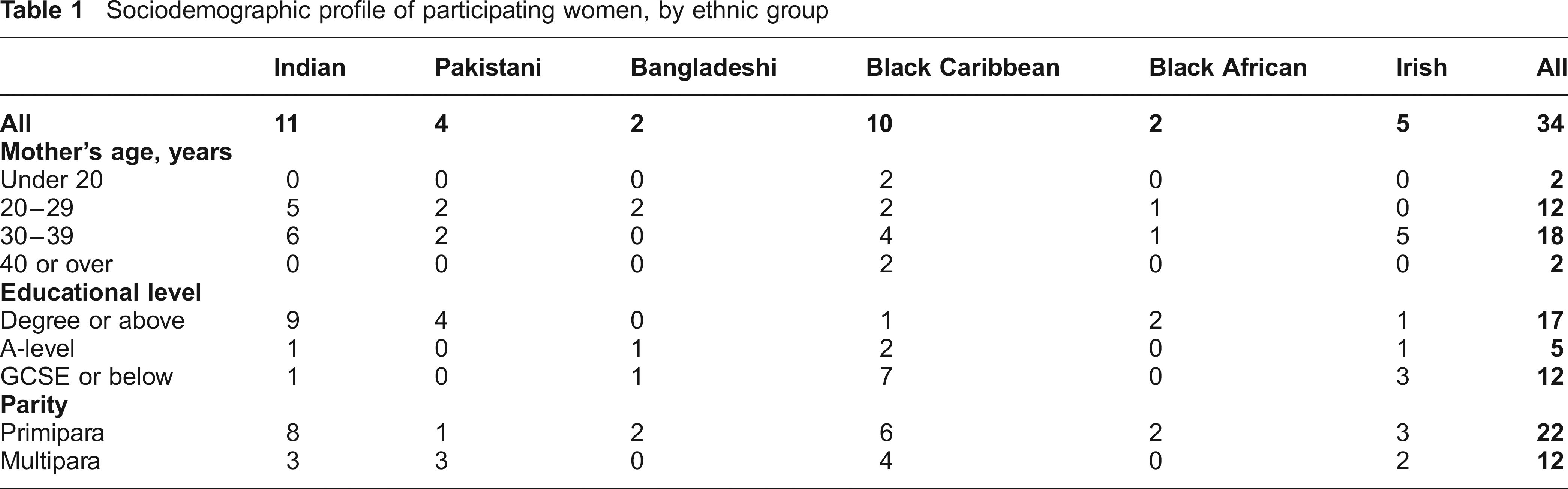
The data presented in this paper are derived from in-depth, semi-structured interviews conducted with 34 UK-born women of Black African, Black Caribbean, Indian, Pakistani, Bangladeshi and Irish descent. Women who were pregnant, or had recently become mothers were recruited mainly from six NHS maternity units in London and three units in Birmingham serving areas selected for their high proportions of residents from these ethnic groups. The recruitment was done mainly by midwives during antenatal appointments. The main inclusion criterion was that women were born in the UK and their parents were born abroad. The methods, recruitment strategies and problems encountered are described in detail elsewhere. 18 Inadvertently, this led to a possible over-representation of older, better educated women. As Table 1 shows, over half of the women were in the 30-39 year age group. Almost half of them were educated up to degree level or above, and a third were educated to General Certificate of Secondary Education (GCSE) or below. The GCSE is a set of exams taken in England and Wales by secondary school students around the age of 16 years.
Sociodemographic profile of participating women, by ethnic group
At the initial contact, all the respondents were given information about the study, about the length of the interview and the scope of questions. The women were interviewed by two of the researchers between three months and one year after childbirth and women who had had adverse physical or mental health problems were excluded.
A flexible topic guide was used for the interviews. Women were first asked in general about their pregnancy and childbirth, and then about the care they had received during pregnancy, childbirth and postnatally, interactions with professionals, family support, breast feeding and cultural practices. This included asking if they had ever felt that their ethnic background influenced their interactions with professionals. Interviews were tape-recorded, with permission from the participants. Written consent was also obtained before the start of the interview. The average duration of the interviews was one hour. Most of the interviews were conducted at the home of the mother, or in a convenient setting free from interruptions and where privacy was ensured. The study was approved by the South East Multicentre Research Ethics Committee and each NHS Trust's Research and Development Committee.
All the interviews were transcribed. The texts were then coded and analysed with the qualitative software package, NVivo. 19 The analysis was based on a grounded theory approach. This involved close reading of the interview transcripts and open coding. 20 The initial codes were then grouped into more abstract levels of codes or themes presented below.
Results
Equitable care
The women in our study felt that their ethnic background did not matter at all to the care that they received. They did not report any cultural barriers with the professionals who provided care, irrespective of whether the professionals came from a White or ethnic minority background:
No. It [ethnic background] didn't really matter at all, because their level of professionalism was really good and they were really friendly and they didn't make me feel that I was any different to them. (Pakistani mother, multipara, 30–39 years, carer)
I had an African woman, but no, it doesn't come into relevance, so I had no issues or problems there. (Black Caribbean mother, multipara, 30–39 years, occupation not recorded, educated to A-level)
[Did you ever feel that your ethnic background made a difference in the way you were treated?] Much of the staff [providing care] is [of] ethnic [background] … But even the non-ethnic staff were very nice. (Pakistani mother, multipara, 30–39 years, librarian)
Being born in the UK, the resulting familiarity with the system and the absence of language barriers were felt by the women to be influential in getting treated equally to White women. They also thought that separate services for ethnic minorities were not appropriate for those born in the country:
No. Absolutely not! Why should I be treated any different from Mary Smith who lives two doors away? … I have access to everything, English is my first language not my second language. Why should I get anything that [is different]? No. In fact I'd resent it if they did! I'd be very annoyed. (Indian mother, multipara, 30–39 years, accounts manager)
Sensitive care
Regardless of their ethnic background, women stressed the need for professionals to be ‘sensitive’ and ‘delicate’ in their interactions. This need for tender ‘loving’ care was the first and often the foremost concern in the interview accounts. Maternity was seen to be a particularly emotional time when women felt themselves to be ‘fragile’ and ‘vulnerable’, and they expected their care-givers to empathize with their individual needs:
When they're dealing with women who are going through the most painful and amazing experience of their life, they need that kind of sense of support and understanding from somebody who's going to be taking care of them throughout the whole process. The midwives need to change their attitudes and try to re-focus on their jobs and believe and be more passionate about it, not just do it as a job really. (African mother, primipara, 20–29 years, occupation not recorded, degree level education)
The perceived lack of sensitivity among the professionals led many women in our study to describe the staff as ‘unfriendly’ and the care as ‘impersonal’, leading to dissatisfaction with the services. This dissatisfaction was particularly obvious with the care that they received in the postnatal period. In general, women expected much more support in caring for the baby and in starting breastfeeding than they received. The mismatch between their expectations and experiences was reflected in some accounts:
Having no sleep, having no rest and thinking maybe the hospital staff will give the mother a rest by taking the baby away, for a couple of hours would be amazing, but there's none of that, there was no help, and I actually asked for the help… I think it was the second night I just broke down in tears, because I was so exhausted, in so much agony… And I asked for help and they said look, we don't do that. I was a bit surprised that, that help wasn't available. (Bangladeshi mother, primipara, 20–29 years, accounts clerk)
Women with additional needs, for instance, those who had a caesarean section, also reported less support than they expected in the immediate postnatal period:
I had to get up on my own, totally unaided, just after surgery, literally not that many hours after and stand there unaided while she changed the bedclothes. And I just thought this was ridiculous. (Black Caribbean mother, multipara, 30–39 years, recruitment consultant)
Compared to other ethnic groups, some Black African and Black Caribbean women expressed stronger dissatisfaction:
I will not have a baby in a hospital again… It's not worth going to hospital because the experience I had was just terrible (African mother, primipara, 20–29 years, occupation not recorded, degree level education)
You're just a number, you're like an animal. They just don't care … The service is there, but the care's not there (Black Caribbean mother, multipara, over 40 years, external relations manager)
Some women were left alone for extended periods of time after birth and this made them anxious. The women were aware of staff shortages, and described the problems as arising partly because of staff being ‘rushed’, but they also felt the staff were ‘remote’ and not interested. The women who received emotional support and reassurance from the staff clearly appreciated this:
But to be honest, the midwives that I had in the maternity suite, they were absolutely brilliant. Yeah. They were very supportive, kept my spirits up, they were there for me, egging me on, ‘you're nearly there, and you're nearly there'. They were very, very good. (Indian mother, primipara, 30–39 years, occupation not recorded, degree level education)
Continuity of care
Continuity of care emerged as a key element in the women's accounts. Most of the women would have preferred to have been cared for by the same group of staff throughout all stages of antenatal, labour and postnatal care:
One thing I always say is I would've preferred it if I had a, like a consistent person to see… . because you get so many, it was quite confusing … during my pregnancy, I must have seen about ten, fifteen midwives. Even during my labour there was like loads (Indian mother, primipara, 20–29 years, human resources advisor)
The women wished for continuity of care, as they valued knowing and being known by the carer and having a trusting relationship. More than wanting to see a familiar face, they wished for carers who knew them with their diverse histories and backgrounds:
There was no common ground really. You just had to start all over again … You know, just that comfort zone. Liaising with, because it wasn't like you had one midwife who knew you, who knew your problems, who knew you from the beginning, it wasn't like that … And that would have helped. (Indian mother, primipara, 20–29 years, dispensing optician)
The lack of continuity from antenatal care to birth and postnatal care by the same group of professionals left the women with the view that the care overall was fragmented and that they were being hurried through a system which counted them more as a number than as a person with specific care needs:
I mean it wasn't a bad relationship but no continuity, it's just the fact that you are with different people at every appointment … you don't really build up a relationship with any of them, you're just another patient and another number really … That would be my main criticism of the way it's run. (Irish mother, primapara, 30–39 years, clerk)
Access to information and communication
All the women in our study spoke English fluently or as a first language. Overall, they sounded positive about the adequacy of the information given during the antenatal appointments, but they also felt that they needed to be assertive and ‘forward’ to be able to communicate their information needs. Some women recounted experiences which made them feel that they were causing a ‘nuisance’ to professionals by asking for more information:
To be honest, OK, information-wise, in terms of when it was asked, it was given … The general sort of, at one point it did feel like, here's your book, now go away and read it, it did feel like that at one point. (Indian mother, primipara, 20–29 years, dispensing optician)
It's like they're just talking over you and you're not there… It just makes you feel really nervous and distracted… But once you let them know that they needed to directly explain things to you then you're all right <laughs> (Black Caribbean mother, primipara, 20–29 years, sales assistant)
There were also women who felt strongly about the inadequacy of the information that they received:
No, she [midwife] didn't, she didn't tell me anything to be honest. I never had much support from her at all. When I went to see her, she was very nice but she didn't give me any information, she didn't talk about a birth plan, I had no support like that … I think a lot of the time, with both pregnancies, I felt that sometimes the midwives expected me to know things that I didn't know (Irish mother, multipara, 30–39 years, nurse)
In general, women considered the antenatal or parentcraft classes conducted by NHS maternity units as important sources of information on pregnancy, birth and postnatal care. The majority of the women in our study attended these classes and spoke positively about the information that was given. Some women faced difficulties in getting access to the parentcraft classes as they were overbooked. Women also noted receiving inconsistent information about the sessions and as a result confused them with antenatal appointments. Women also sought information through sources like television programmes, the internet, books and the National Childbirth Trust, a UK-based voluntary organization that provides information and support for pregnancy, birth and post-natal care. They felt that being born in the UK in general put them in a better position to secure information through alternative channels, but, even so, they expected authoritative information from professionals. Although not frequent, there were instances where the level and manner of communication by professionals left the women anxious and worried:
And I remember there was one thing the midwife said, ‘Oh, we think you might have diabetes, pregnancy diabetes’, and when I left the surgery I was in tears, she really frightened me, you know? But when I went for the tests they said everything was fine. You know, she really made me panic, like the way she was explaining it to me, basically, by how she said it to me. (Black Caribbean mother, multipara, over 40 years, mental health worker)
Women also recounted instances when they felt they were ‘unheard’ or not taken seriously:
I said ‘I'm really not well'. And they said ‘you look fine. Everything's normal'. I said please, there is something going on. And it was just unbelievable how they didn't take it so seriously and within … my baby was born at 4.30 so within such short time it all happened. (Bangladeshi mother, primipara, 20–29 years, accounts clerk)
Care environment
All the women, except one, gave birth in a hospital maternity unit or a birth centre. While most commented that they perceived hospital delivery as safe, they expressed the need for a better physical environment and facilities in maternity units:
I would have liked the whole thing to have happened in a much nicer environment. [Name of the Maternity unit] is grim to say the least, it's Victorian-looking, it's grey, it's dark and dull and, having said that, the staff, the midwives, were fine, were great…but the place itself was quite a depressing place to give birth in and a bit frightening really. (Irish mother, primipara, 30–39 years, clerk)
It also appeared that due to the lack of space, some women were not admitted to the delivery suite despite being in labour, or were sent home against their wishes when they felt it safer to remain in the labour ward. There was also an impression that the ‘internal atmosphere’ of some maternity units was ‘stressed’ with women listening to ‘arguments’ among the staff related to staff shortages. The lack of a supportive environment apparently led to a sense apprehension. The prevailing impression was that the hospital stay was ‘frustrating’ and they often felt like ‘walking out’ of the hospital.
The dissatisfaction with the facilities in the postnatal wards was more explicit. The shortcomings perceived included a poor state of equipment and furnishing, lack of privacy, background noise, lack of cleanliness and hygiene. Some women gave disturbing accounts about the state of facilities in some postnatal wards:
So they moved me to another ward, not another ward, just another area of the ward, but there was no light. And they gave me like a pen like yours … a pen-torch, and that's what I needed to use to see my baby to feed my baby. (Black Caribbean mother, multipara, 30–39 years, recruitment consultant)
Women also stressed the need for a balanced and healthy diet in the hospital. As a result of their dissatisfaction with the facilities and the environment, some women were considering home birth options in future. The accounts from a few women who gave birth in a ‘pleasant environment’ demonstrated the influence of the care environment in colouring women's maternity experience:
Yeah, the care was very good … they've got a birthing centre there and it's quite new, it's only two years been opening, and I thought I'd have the baby there ‘cause it's got a really nice setting … you know, nice rooms and stuff (Pakistani mother, primipara, 20–29 years, unemployed – degree level education)
Discussion
As this was a qualitative study of the views of UK-born women from selected ethnic groups, our findings are not necessarily representative of all UK-born ethnic minority women. We were successful in accessing women from Indian and Black Caribbean backgrounds, but less so in recruiting from the other ethnic groups in spite of focused recruitment strategies. 18 The initial study design included triangulation with both focus group discussions and in-depth interviews, but focus groups were dropped due to logistic issues. This might have affected the reliability of the findings, but in-depth interviews were found to be more suitable for exploring the complex subjective dimensions of personal experiences. As few studies have focused on UK-born ethnic minority women's maternity experiences, it is difficult to compare these findings with those from previous studies.
Perceptions of equity and woman-focused care
The perceptions of equity reflected in the interviews are a departure from previous research findings that have suggested that direct as well as subtle racism is experienced by women from ethnic minority groups.6,7,9,14,16,17 The women perceived their UK-born status and their language competence as influential in being treated equally. Larger studies using representative samples and standardized measurement tools would be needed to be able to generalize about whether the perceptions of equitable care of UK-born women corresponded to the care they received. Maternity care professionals interviewed in the other component of our study also noted that UK-born women's language competence and familiarity with the system were key advantages in care provision. 21 This reinforces the view that the provision of effective language support services can promote equitable care to non-English-speaking women.7,9,14
The professionals interviewed felt that the needs of UK-born ethnic minority women were largely similar to those of their White counterparts. 21 In part, this corresponds with the views of the women reported here. As evident in some interviews and as is increasingly true in the NHS as a whole, the professionals in the maternity units included in the study were very diverse ethnically, but the study was too small to explore how this might have influenced the women's experiences. Further, the NHS has been focussing increasingly on the development and application of policy guidelines and programmes for improving cultural competency of the staff and for promoting equity. It could be argued that these have given professionals the knowledge and skills to enable them to recognize and value similarities and differences within and between culturally diverse groups. There is some evidence from mental health care, however, that cultural competency training has had a limited impact on service delivery. 22
The women valued sensitive care combined with good communication and access to information. These concerns reflect the fundamental hopes and wishes found in many other studies of maternity care in England, irrespective of women's ethnicity.1,15 It has been pointed out that it is important not to regard minority ethnic women's self-defined needs as ‘special’, but rather as ordinary needs which, in the current organization of care, are not being met. 14 The strong expressions of ‘unmet’ care needs that surfaced in our study could also be partially explained in terms of the fact that most of the women attended maternity units which were subsequently rated by the Health Care Commission as being among the least well performing in England. 23 Although our study was not designed to study associations between experiences and outcomes, it is interesting to note that some of the most critical accounts came from Black Caribbean and African women, two groups which experience particularly poor maternal and infant outcomes. 8
Provider aspects, continuity and care environment
The other common thread running through the women's accounts is their emphasis on the importance of the client-provider relationship. Our findings and those of others 7 suggest that a having a culturally diverse workforce in itself is not sufficient to ensure that professionals are sensitive to the expectations of individual women in their care. The women had clear expectations about their interactions with care providers. They valued warmth, support, effective reassurance, and the resultant feelings of trust and confidence, and wished for professionals who ‘care about’ as well as ‘care for’ them. Delivering health care with compassion, that acknowledges the person beyond their need for treatment, is a key aim of current policies. 24 The notion of dignity-conserving care, while emerging primarily from palliative care, applies across health care. It has been argued that health care providers can positively influence the experience of individual clients by showing true compassion, leading to the right behaviour and an effective dialogue. 25
Our findings reinforce the view that core values such as kindness, respect and dignity are indispensable if maternity services are to provide women-centred care. As some of the interviews show, however, maternity professionals, working under pressure, tend to perform habitual and ritualized tasks that depersonalize caring. The analysis of professionals’ views in the other component of our study suggested that improving interpersonal and communication skills, active listening skills and self-awareness among professionals could be promising in promoting women-focused care in maternity services. 21
Women in our study also greatly valued personal continuity from care providers which they deemed as necessary to build a trusting relationship conducive for sharing their intimate experiences. Reviews of maternity services have recommended continuity of midwifery care1,3 and it has been argued that such issues are particularly important to ethnic minority women. 26 Some authors have suggested, however, that issues like ‘continuity’ of carer or ‘knowing’ the carer were less important than the attitude of the carers and the philosophy of care, together with a calm environment.27,28 Although we found continuity as an important factor for women, our study design could not produce definite conclusions about the association between continuity of carer and women's satisfaction with their care.
Wherever women choose to give birth, they prefer a pleasant and safe birth environment which is quiet and relaxed with comfortable ‘home-like’ surroundings. 2 While the women in our study had similar expectations, there was little congruence between their expectations and their experiences. The sense of disempowerment and apprehension arising from the lack of supportive environments reflects findings from other studies about the effect of the surroundings and facilities on the process of childbirth28,29 and women's concerns about birth environments in England.15,30
Conclusions
Many of our findings on maternity care expectations and experiences of UK-born ethnic minority women are consistent with those of all child bearing women. An encouraging finding from our study is that the women did not feel discriminatory behaviour or experience cultural barriers related to the professionals who provided care. They appreciated the equitable treatment they received, but they wished for more sensitive care characterized by humane values. They also felt the need for more personal continuity in their care to enable them to develop feelings of trust and confidence in the professionals. Women valued good communication and consistent information, with their views acknowledged and their questions answered consistently. They also wished for a more pleasant and conducive caring environment for maternity and postnatal care.
We found little congruence between women's expectations and their experiences of maternity services despite attempts to change and improve services over the past few decades. Our findings point to the need for maternity services to move further from knowledge-based cultural competence towards a greater focus on each woman as an individual with her own needs. Policy makers, commissioners and health care professionals working in maternity care may reflect on this evidence while designing services and caring for women at an important time in their lives.
Footnotes
Acknowledgements
The project was initially funded by the Community Fund, now known as the Big Lottery, through a grant to the Maternity Alliance. After Maternity Alliance went into insolvency, the funding was transferred to Women's Health and Family Services. The authors would like to thank the former staff of the Maternity Alliance especially Christine Gowdridge, Ruba Sivagnanum, Ros Bragg and Mary Makoni, colleagues at City University London, especially Shamoly Ahmed and Carol Dossett, and the staff at Women's Health and Family Services, especially Joyce Grandison and Jo Weller and the Chair Pam Schickler for their support. We would also like to thank all our participants for giving their time and energy to this project.