
Abstract
Objectives:
In developed countries, community pharmacists are increasingly involved in clinical care. This study aimed to explore the acceptability to users of pharmaceutical care (drug therapy monitoring and management) provided in Portuguese community pharmacies, thereby informing future practice, policy and research.
Methods:
Qualitative semi-structured telephone interviews with a maximum variability sample of 21 service users. Interviews were audio-taped with permission of interviewees, transcribed verbatim and analysed using the ‘framework approach’ with the help of NVIVO® software.
Results:
A perception of convenient access is one of the key themes associated with acceptability to users. Four factors are central in understanding this perception: shorter waiting time; flexibility of appointments; service organization; and proximity to home. Data analysis suggests that these factors have different weights. Another key theme underpinning user acceptability is the formation of a therapeutic relationship with the pharmacist. Patients’ accounts provide evidence of a trusting and collaborative relationship where the pharmacist is seen as a health care provider. Recognition of interpersonal and technical skills were associated with the formation of this relationship. Although patients generally trusted the pharmacist's ability to help, patients were unable to voice clear expectations about the service, either in terms of the pharmacist's role or expected outcomes.
Conclusions:
Acceptability to patients is mainly determined by perceptions of convenient access and the development of a therapeutic relationship with the pharmacist. Patients’ expectations concerning the service are not well developed, but not necessarily low.
Introduction
In developed countries, community pharmacists are increasingly involved in clinical care through new services. Driven mainly by a professional body, Portuguese community pharmacists have implemented services to respond to unmet patient needs, 1 namely pharmaceutical care for patients with chronic conditions, such as asthma, diabetes and hypertension. Principal elements of the pharmaceutical care mandate are the provision of medication-related care directly to a patient to achieve specific outcomes, ultimately to improve the patient's quality of life, with the provider accepting personal responsibility for the outcomes. 2 The provision of medication-related care involves monitoring drug therapy in relation to need, effectiveness and safety, in collaboration with the patient and other health professionals.
Pharmaceutical care programmes were rolled out in 2003; they share a common structure and hence forward will be referred to as ‘the service’. Prior to service implementation pharmacists receive mandatory training to enhance their skills in monitoring drug therapy. Training also covers communication skills (with patients and physicians) and documentation. The service is provided autonomously from general practice; it is commonly advertised to the public in pharmacies with accredited pharmacists and offered to patients, especially to those with uncontrolled conditions. It consists of regular consultations with the pharmacist in a community pharmacy private area. Since there are few mechanisms to share clinical data across settings in the Portuguese health care system, community pharmacists rely on their own resources (e.g. pharmacy dispensing records, measurements performed in the pharmacy) and on medication reviews, laboratory tests and other examinations for diagnostic or monitoring purposes in their possession. Interventions focus on both drug therapy management and lifestyle changes.
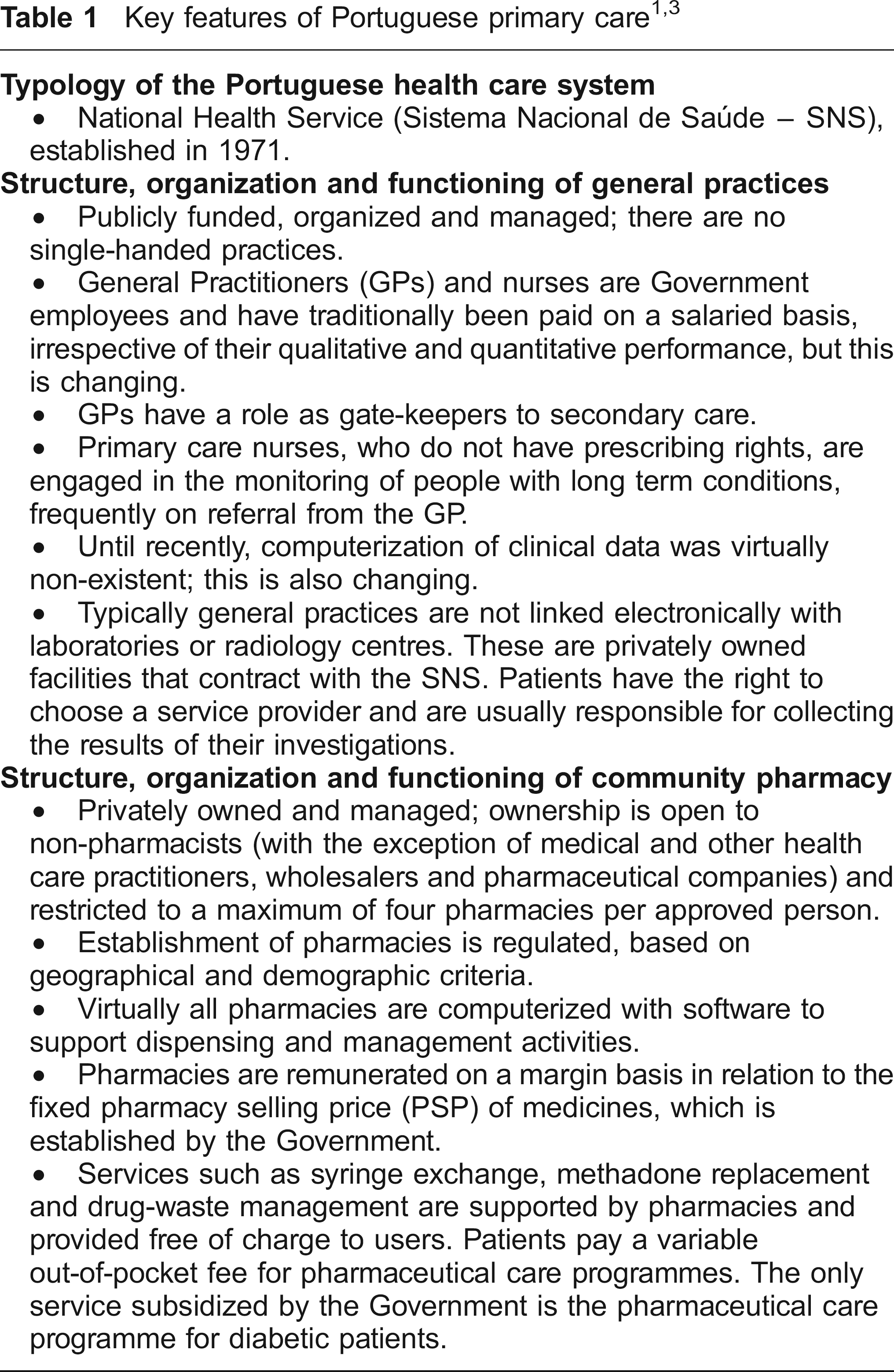
By November 2005, about a tenth of Portuguese pharmacies were following 2903 patients (mean of 8 patients per pharmacy). 1 Remuneration of the diabetes programme consists of a fee per patient per month, 75% funded by the Ministry of Health and 25% by the patient. The other programmes are not subsidized by the Government; patients may pay a variable fee. Table 1 sets the context by presenting information about the Portuguese health care system, with a focus on primary care.
Increased weight is being given to patients’ perspectives on the health care they receive. Therefore, understanding the acceptability of new pharmacy services to users is fundamental to inform practice, policy and research. However, little is known about users’ perspectives on new services implemented in their regular community pharmacies, especially when these services are independent of dispensing. Published research in this area4–6 has involved services delivered by pharmacists not previously known to patients and in other settings, such as general practice. Other studies investigated patients’ perspectives on initiatives in community pharmacy prior to their implementation7–10 or included subjects who were not service users.11,12 Contact with an initiative in a research context and lack of experience with a service may distort patients’ views. Additionally, the nature of the service is important, as acceptability may vary depending on the perceived cost (e.g. time, money) and patients’ beliefs about the benefits. Studies in the community pharmacy setting that researched users, such as Renberg et al, 13 focused frequently on services linked to dispensing.
This study aims to address this evidence gap by exploring the acceptability to users of pharmaceutical care programmes provided in Portuguese community pharmacies. It was hoped that this could offer insights into patients’ perceptions of the benefits of these services, their experiences and their expectations.
Methods
Patients were recruited from ten community pharmacies located mostly in urban areas of central and southern Portugal that took part in a larger research study 14 designed to develop and evaluate an evidence-based intervention to improve the quality and safety of medication use in community pharmacy. The research combined quantitative and qualitative methods. Acceptability to patients was one of the final qualitative studies.
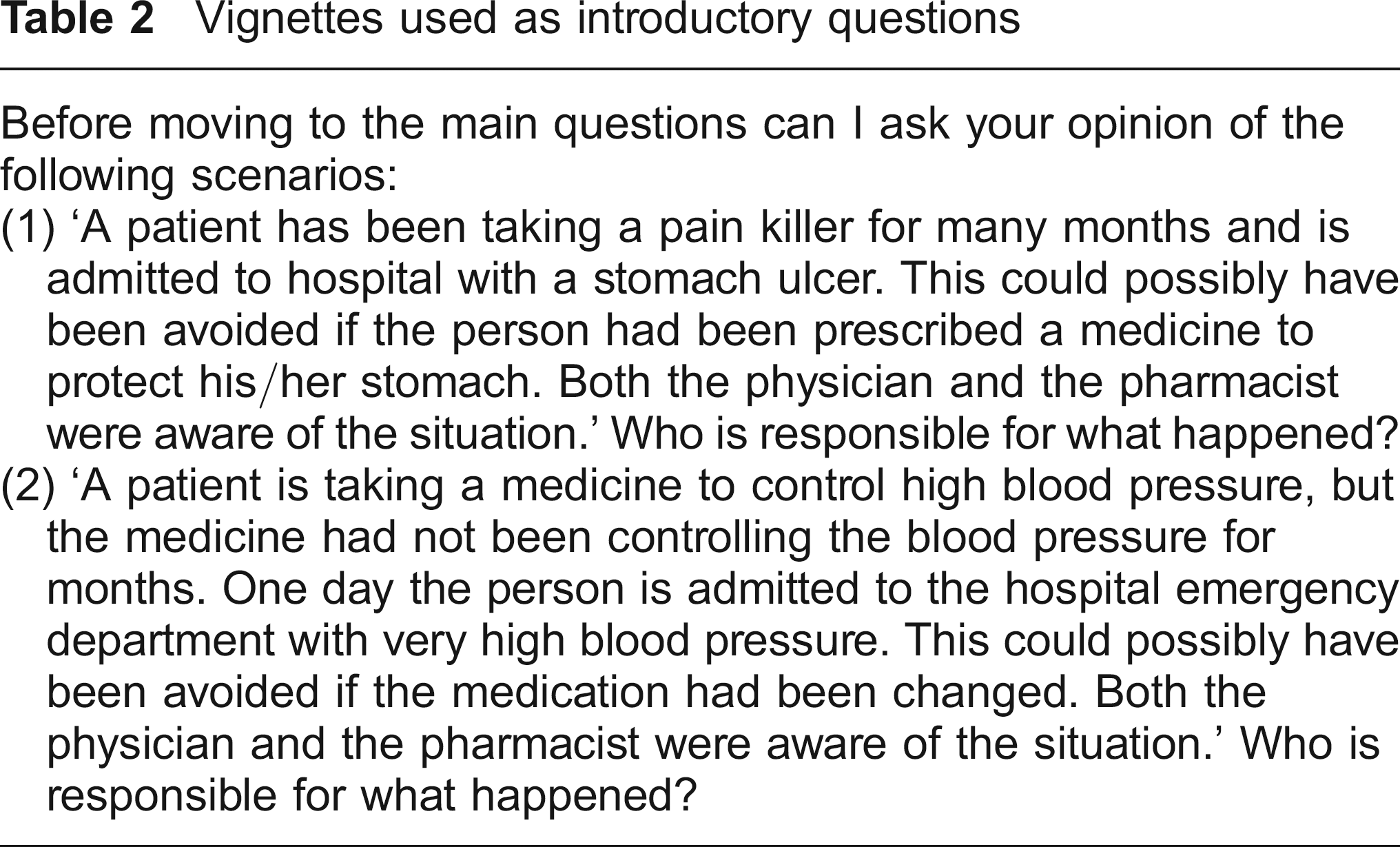
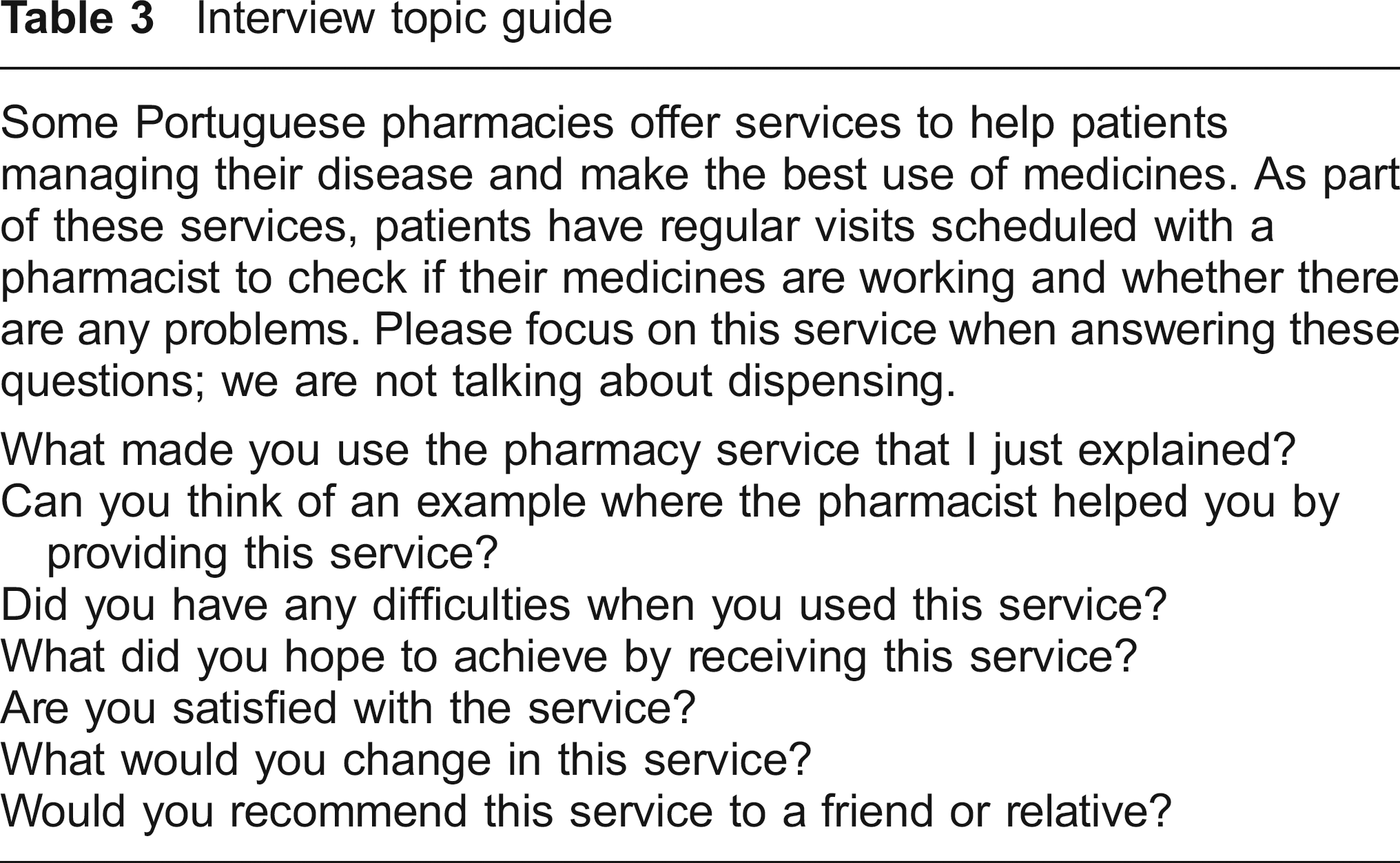
Qualitative telephone interviews were chosen, mainly due to the geographical dispersion of potential interviewees. Eligible patients had received the service for at least one year and had access to a fixed telephone line at home. Patients with hearing impairment and/or a history of a recent debilitating event were excluded. A sample framework, where patients’ identity was protected by a pharmacy ID code, was used to purposively select patients. Characteristics such as gender, age and education level were employed to ensure diversity within the sample, while avoiding dominance of interviewees from a particular pharmacy. At initial contact, all the patients were given an information leaflet supplemented with an oral explanation of the study. Written consent was sought from those who agreed to participate. The interview started with two general questions to elicit views on responsibility for drug therapy outcomes (Table 2), and then moved to more specific questions about the service (Table 3). Questions and probes were piloted with a service user selected on the basis of convenience, and revised throughout data collection in the light of emerging views.
Vignettes used as introductory questions
Interview topic guide
Interviews were conducted between February and April 2006 by one of the authors. The average duration was 30 minutes. Interviews were audio-taped with permission and anonymized during verbatim transcription. Recruitment ceased after the twenty-first interview, as no new information was forthcoming and the data were considered rich and informative. A profile of the sample is presented in Table 4.
Profile of service users interviewed
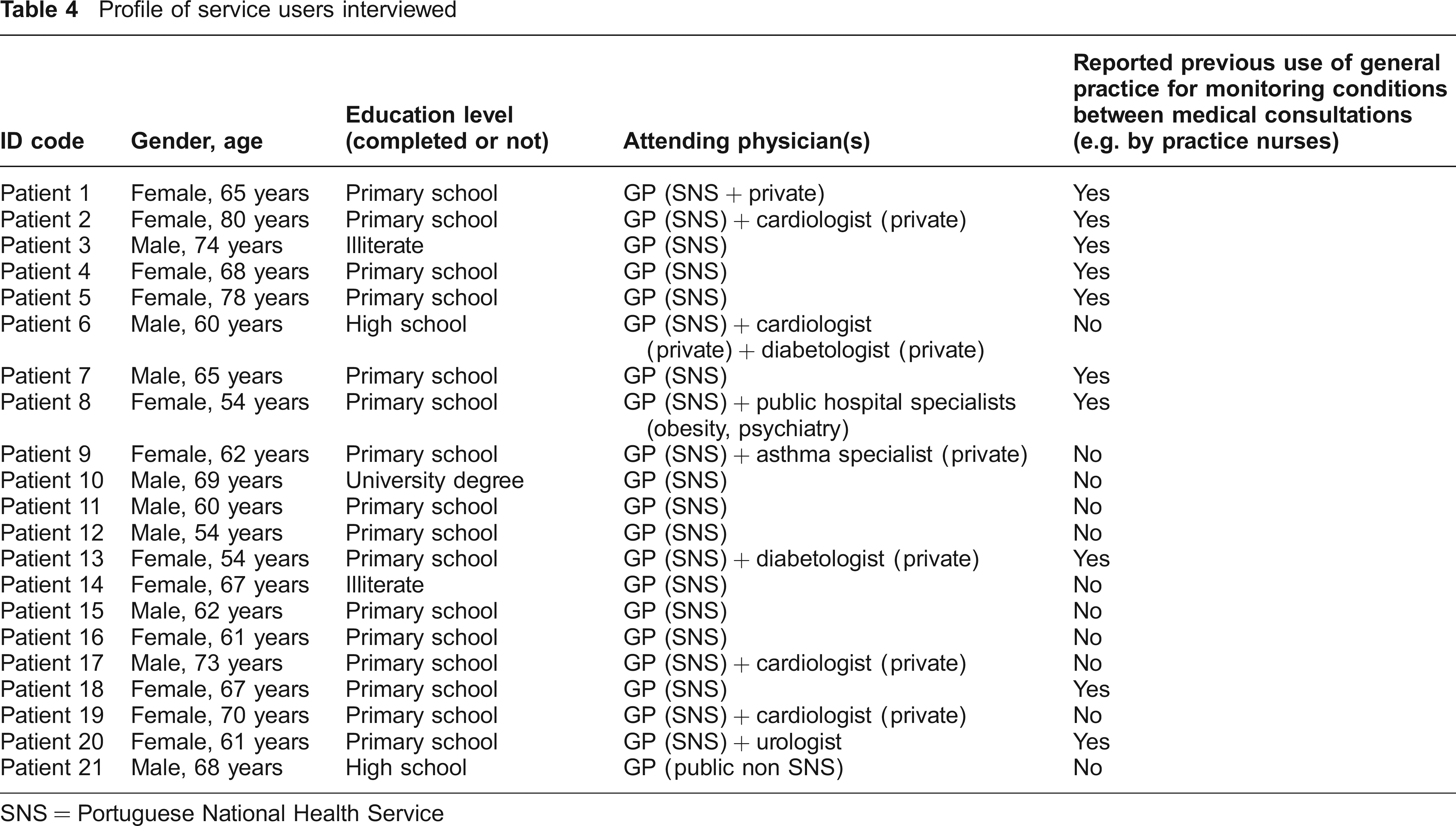
SNS = Portuguese National Health Service
The five-stage ‘framework approach’15,16 developed in the UK for applied qualitative research, was adopted to analyse data in the original language (Portuguese) with the help of QSR NVIVO® version 2.0. 17 A coding frame was initially used based upon broad categories, such as choice, utility and satisfaction. Further codes emerging from data were then devised (e.g. access, interpersonal skills), with transcripts being re-read until all emerging themes had been coded. The analytical idea each code referred to was explicitly defined to ensure coding was carried out in a systematic and consistent fashion. Charts were then developed for key themes, by grouping relevant codes and entries for all interviewees. This enabled theoretical elaboration, by identifying patterns, examining associations and searching for disconfirming cases. For reporting purposes, quotations were translated into English, after discussion between the primary analyst (MPG) and a native English speaking researcher. They were selected to illustrate the analysis, while trying to give readers a feel for the people studied and avoiding dominance of a particular interviewee.
It was not possible to seek ethical approval for this study since Portugal does not have formal mechanisms to review health services research protocols. Nonetheless, the study was conducted in an ethically responsible manner, adhering to the same principles and procedures as studies approved by Research Ethics Committees in England.
Results
Positive characteristics of the pharmacy service
Patients were unanimously satisfied with the service, to the extent that some had recommended it to others, and could not think of aspects to be improved. Access to the service was considered convenient by all patients. Analysis of the theme ‘access’ was performed by dividing patients into two sub-groups, based on whether they had previous experience of an equivalent non-pharmacy based service.
Half the interviewees had previously received monitoring for their diabetes or hypertension from a practice nurse in Portuguese NHS (SNS) surgeries. In such cases, the decision to use the pharmacy-based service instead of the service offered by nurses was determined mainly by a perception of better access. A number of issues are central to understanding this perception: waiting time; flexibility of appointments; service organization; and proximity to home. The most frequently mentioned factor was the shorter waiting time for the pharmacy-based service:
If I go to the surgery to have my blood pressure measured … first I need to get a ticket, and then I have to wait my turn. It's a lot easier to go to the pharmacy (…) I don't spend as much time and effort because often it's not only time, sometimes one gets irritated when kept waiting for hours for such a little thing (…) [Patient 20]
Flexibility of appointments was another recurrent issue. Patients perceived the pharmacy as offering more flexibility than general practice. This was often related to the time during which the service was available and the ease of changing appointments or being consulted outside scheduled appointments:
(…) I go at a time that suits me, they (pharmacists) don't have any problem. They ask me for a day when I can go but if I can't go on that day I'll go some other day and at some other time (…) thank God, I'm very well taken care of [Patient 1]
Service organization also seemed to influence patients’ preferences for the pharmacy-based service. In a few cases, the service offered by SNS surgeries was regarded as ‘full of bureaucracy’ [Patient 13]; i.e. having rules that, from the patient's perspective, hindered access:
(…) at the surgery I have to ask for a referral form from the GP (to see the nurse). Since I can go to the pharmacy by paying a small amount, I'm a regular customer there. I'm well taken care of (there), they look after me, thus I continue (to go) there [Patient 2]
In another surgery, what was regarded as staff management problems discouraged the patient from using the service provided by the nurse; this patient showed how he would use the pharmacy service as an alternative:
(…) The appointment is booked for a particular day, you get there and the nurse has been sent to some other place ‘cos another nurse is sick (…) it gets weary… you go there once, and then again and again and it's the same old story (…) Hence I go there (pharmacy) (…) [Patient 4]
In addition, proximity to home was acknowledged by some patients. However, analysis suggested that proximity on its own is insufficient for the service to be deemed accessible. This contention is supported by the fact that proximity was often mentioned together with other factors:
[Patient 7] It's further away (surgery), you have to drive and then look for a place to park the car, all that stuff and it takes longer.
[Interviewer] It takes longer?
[Patient 7] Of course, in the pharmacy I may be taken care of after five minutes while in the surgery I have to wait one hour (…) in the pharmacy I have to pay while in the surgery it's free. But I'd rather go to the pharmacy than to the surgery.
Approximately half the patients reported not having used SNS surgeries in the past to have their conditions monitored by the practice nurse between medical consultations. There were a number of reasons for this, such as a poor impression of how surgeries functioned:
(…) the surgery (…) can be very good but I've never used it (for monitoring). People say they go there and this and that but I don't have time to spend a morning there (…) I prefer the service in the pharmacy with (pharmacist) [Patient 15]
There was general agreement in this sub-group that the pharmacy-based service was easily accessible, with the same access issues emerging as for those who had used SNS surgeries in the past.
There was no evidence of difficulties in accessing the pharmacy-based service for any of the sub-groups of patients. Additionally, the fact that the issues emerging from the analysis were the same in both sub-groups further supports the notion of convenience, as even those patients without prior ‘worse’ experiences acknowledged ease of access to the pharmacy-based service.
Relationship between the patient and the pharmacist
Data indicating the formation of a patient-pharmacist therapeutic relationship was common. This relationship is probably best described along a spectrum from ‘not formed’ to ‘strongly formed’, as patients varied in the extent to which they described this relationship. This is designated ‘therapeutic’ as there was evidence of both trust and collaboration with the pharmacist as a health care provider.
Overall, patients showed they trusted their pharmacist to help them manage health problems while displaying a collaborative attitude, by taking pharmacists’ advice:
(…) I've been looking (for an appointment with the GP) since January and I still haven't got one (…) meanwhile the pharmacist has counselled me on what to do (lifestyle management) and as a matter of fact my diabetes has got better, ‘cos she tells me what to do and I've done it [Patient 16]
It is also possible to discern this collaborative attitude in the keenness to share with the pharmacist personal information, such as laboratory and diagnostic data, expressed by some patients:
(…) when I attend hospital consultations I always show (them) my investigations and I tell (them) what had happened there, what the consultant told me, and the pharmacist writes it all down [Patient 1]
In a few cases, it was clear that familiarity with the pharmacist or pharmacists providing the service, based on regular contact, facilitated the development of this relationship: ‘they (pharmacists) have known me for a long time; I can even have a joke with them’ [Patient 7].
Recognition of interpersonal and technical skills emerged as reasons to explain the formation of this relationship. Pharmacists were described as ‘kind’ [Patients 2, 3, 8, 9], ‘very nice’ [Patient 7, 11] and ‘almost like family’ [Patient 17]. In a few cases there were implicit or explicit comparisons with other health professionals, in an attempt to demonstrate pharmacists’ care and attention:
(…) (the pharmacist) talks more to me (than the nurse), she takes better care of me (…). Now I have a new GP, who seems a bit more attentive, I've only been there once though, but the other GP would rush me from the moment I got in, while the pharmacist listens (…) [Patient 8]
This quote also offers evidence of the importance attached to having time with an apparently unhurried health care professional, an aspect echoed by other interviewees. Moreover, the view that it was easy to discuss medication and health problems with the pharmacist received unequivocal endorsement by patients.
In addition to interpersonal skills, evidence of recognition and appreciation of pharmacists’ technical skills recurred throughout. Firstly, patients acknowledged that pharmacists’ education gave them knowledge. This was sometimes expressed in terms of a patient-pharmacist knowledge gap, with the pharmacist being regarded as more knowledgeable than the patient: ‘we should have a bit of trust in our pharmacist, because they ought to be a bit more educated than us, shouldn't they?’ [Patient 20]. In other cases, pharmacists’ knowledge was discussed in relation to physicians’, which suggests a perception of hierarchy between the two professions: ‘he (pharmacist) gives good advice and sort of knows what he's doing, although he's not a physician’ [Patient 4]. Secondly, there was a sense of health improvement as a result of pharmacists’ input. For example, two patients reported having lost weight. One patient showed he accepted responsibility for not having made a greater improvement; he explained how he ‘did not comply (…) rigorously with what’ the pharmacist had advised, as ‘if I had complied (…) I think I'd have been fine’ [Patient 12].
Reassurance following advice either on lifestyle or drug therapy management was also voiced: ‘we feel more reassured. Many times the pharmacist says, “If this medicine does this or that, (then)…”, therefore one is aware of what the medicine could do'’ [Patient 13]. A third piece of evidence supporting the case that patients valued pharmacists’ technical skills was that patients would attend the pharmacy in spite of having self-monitoring devices for blood pressure and/or blood glucose. About half the interviewees were in this situation, but chose to attend the pharmacy regularly, mainly due to the advice they could get from the pharmacist:
(…) there is a person who assists me, a person who knows about the subject (…) for example (if) I have a high reading or something and don't know what to do, I think the pharmacist will tell me… to take another medicine or to consult with the physician… I'm better assisted (there) (..) [Patient 21]
A final argument that supports the case of valued technical skills is patients’ acceptance of a referral role for pharmacists. This aspect, which is illustrated by the previous quotation, came up in other interviews. This suggests that patients believe the pharmacist has the ability to judge whether medical consultation is the most appropriate course of action.
Although the majority of patients demonstrated the existence of a therapeutic relationship with their pharmacist, one case appeared to differ though this could be explained (Box 1).
Disconfirming case analysis – therapeutic relationship
Patient 18 showed she accepted the existence of the patient-pharmacist knowledge gap: ‘she (pharmacist) differs from a person who doesn't know anything’, but perceived little utility in receiving the pharmacy-based service. Underlying this perception was a feeling of how the service ‘is just measuring the blood pressure, nothing else (…) she (pharmacist) gives little advice’. When probed as to why she was still attending the pharmacy, especially since she owned a self-monitoring device for blood pressure, she voiced appreciation for the attention she received: ‘I like them (pharmacy staff) all, they befriend me and I like going to that pharmacy and measuring my blood pressure there, nothing else'’. This patient is probably close to the end of the spectrum of ‘therapeutic relationship not formed’. The reasons are two-fold. There was no evidence of recognition or appreciation of the pharmacist's interpersonal skills, but rather of the pharmacy staff in general. This suggests that the patient considered the pharmacy staff as part of her social network, and not as health care professionals. Moreover, there is little recognition of technical competence, as the patient was clear about not perceiving any benefit for her health from the relationship with the pharmacist.
Patients’ expectations about the pharmacy service
Although patients generally displayed trust in the pharmacist's ability to help them, patients’ answers on what to expect from the service were elusive, both in terms of outcomes and the pharmacist's professional role: ‘(…) she listens to my complaints. (…) and she sorts out whatever she has to sort out’ [Patient 8].
Analysis suggests that interviewees are unable to conceptualize a professional role for pharmacists as advocated by the pharmaceutical care mandate. Two arguments support this contention. Firstly, there is no evidence that patients recognize a role for pharmacists in monitoring drug therapy. All but one patient (Box 2) considered that they would or had discussed concerns about the safety or effectiveness of their medication with the pharmacist, either as a first port-of-call or as an alternative to the general practitioner. This suggests acceptance of an advisory role for pharmacists in response to patient driven-concerns, which is distinct from a monitoring role, in which the pharmacist pro-actively checks drug therapy. More importantly, patients appeared unaware of the need to monitor drug therapy. They described the service in terms of monitoring their disease, and not their medication: ‘(…) (to) know how this (blood pressure) is doing (…)’ [Patient 4]. This aspect is also illustrated by patients’ descriptions of consultations with the pharmacist, which were recurrently centred on measurements, such as blood pressure and blood glucose, and what was perceived as advice offered as a consequence of these.
Disconfirming case analysis – patients’ expectations
Patient 19 offered a different perspective in relation to discussing concerns about her medication with her pharmacist, reflecting the belief that this is not the pharmacist's role: ‘I don't think it's their (pharmacists') responsibility’. An apparent lack of previous experience of discussing her medication with the pharmacist may help to explain this stance. Firstly, the patient did not appear to perceive a need for such discussion since she had been on medicines prescribed by a cardiologist ‘for many years and I feel just fine’, which contrasts with other interviewees. Secondly, she was the only diabetic patient in the sample managed exclusively with lifestyle changes; therefore the pharmacist's attention was probably less focused on medicines in her use.
Secondly, patients do not seem to recognize pharmacists’ shared responsibility for drug therapy outcomes. In their responses to the hypothetical scenarios, patients believed that such responsibility rests with the physician. Their unanimous perspective was that a ‘physician's slip’ [Patient 1] was the cause of the adverse outcomes presented, as ‘the physician should have prescribed an additional medicine (gastroprotective agent) with their other medicine (pain killer)'’ [Patient 16] or changed the antihypertensive medication. These accounts illustrate that prescribing rights seem to be integral to understanding patients’ perceptions of responsibility for drug therapy outcomes. Yet, the division between prescribers and non-prescribers appears to remain well-rooted, with only two patients challenging the status quo: ‘I wouldn't change anything (in the service) (…) except perhaps giving more authority or something to (pharmacist) (…) so that she could change or reduce the tablets’ [Patient 15].
Discussion
Little is known about patients’ views of enhanced community pharmacy services independent of dispensing. Our study offers novel insights into why a pharmaceutical care service is acceptable to users, as well as data on patients’ expectations. However, two key limitations should be noted. Firstly, some patients were aware of the professional status of the interviewer as a pharmacist. It is possible that this may have influenced the data obtained. Nevertheless, what can be seen as less favourable views on pharmacists were expressed, as attested by the disconfirming cases, which suggests that this bias, at least in part, was minimized. Secondly, the users’ views and experiences are not intended to be representative of users nationally. Patients were recruited from a self-selected group of pharmacies participating in a larger research study; 14 these pharmacies may differ from others delivering the same service. It is possible that their pharmacists are more committed to patient care and have higher job satisfaction, 18 aspects that may influence acceptability for patients.
Implications for practice and policy
Our research found that this service meets patients’ priorities in terms of access, which was considered convenient and better than access to general practices. Problems with service organization and waiting times in Portuguese general practices have been confirmed by a number of surveys. 3 No literature was found on accessibility to pharmaceutical care services in community pharmacies; our study provides useful insights as to why the service is considered accessible. For current service management and further implementation, it should be borne in mind that waiting time and flexibility of appointments, which are perhaps more easily modifiable by service providers than location, appear to be necessary for patients to form a perception of convenient access. Wider implementation (both in terms of increasing the number of pharmacies and number of patients monitored per pharmacy) is necessary for the service to be considered a realistic alternative to general practice. Such implementation will have to address a number of factors internal and external to the pharmacy environment, including interprofessional relationships between pharmacists and physicians. 14
Our study indicates that patients were unable to voice clear expectations about the pharmacist's role and the anticipated outcomes, which is in agreement with Renberg's findings for a patient medication record service. 13 Nonetheless, patients’ accounts of the service demonstrated that they expected professional input, in the form of advice, reassurance and/or referral. Thus expectations should not necessarily be considered low. The novelty of both pharmacists’ role expansion and the service may explain this apparent mismatch, as patients may not yet have enough experience of these new services to reflect on how they would affect them.
A significant finding is the development of a therapeutic relationship between patients and their pharmacist. Rovers et al. 2 cite trust and cooperation as attributes of such relationships, while stressing that pharmacists’ contribution includes ‘maintaining an appropriate attitude of caring’. Our study offers evidence of these elements from the patients’ perspective. Interpersonal skills were highly valued, which suggests that the pharmacists who embraced a new professional role were succeeding in effectively interacting with patients. In particular, time with an apparently unhurried professional was appreciated, which is in accordance with previous findings. 10 ‘Using their professional knowledge and skills on the patient's behalf,’ is also cited 2 as a pharmacist's contribution to the therapeutic relationship.
Our study indicates that while most patients perceived their pharmacist as a health care provider none showed awareness of the need for monitoring drug therapy. This is consistent with the findings of a US survey 19 and suggests that it is paramount to inform patients about the risk of medication-related problems and how monitoring by pharmacists may reduce that risk. Raising awareness about these aspects coupled to patients’ experiences of service provision may shape patients’ expectations about the pharmacists’ role. It is unlikely that community pharmacists will achieve an established clinical role if patients fail to recognize the nature of pharmacists’ skills and their relationship to their medication use.
A recent study 10 of patients’ experiences of a community pharmacy medicines management service found that many patients still regarded their doctor as the health professional ‘in charge’ of their medicines. Our results further support this notion, while suggesting that this is intrinsically linked to prescribing rights. In spite of the influence of the health care division of labour on patients’ perceptions, also highlighted by Bissel et al. 10 it is possible that sustained experience with this service may lead to an understanding that responsibility for drug therapy outcomes is shared between health professionals involved and patients.
Implications for research
The patient-pharmacist therapeutic relationship is an integral component of the practice of pharmaceutical care2,20 and future studies need to address pharmacists’ and patients’ beliefs, expectations and attitudes with respect to relationship roles. Our study showed that, in general, patients trusted pharmacists to provide advice to help them manage their health problems. This contrasts with a recent British study, 6 which researched 29 home medication reviews performed by seven community pharmacists previously unknown to patients. The lack of a therapeutic relationship may be a key factor in explaining this discrepancy, as our findings suggest that patients form their impressions of utility in the context of a trusting and collaborative relationship. This reinforces the notion that caution should be exerted when generalizing findings on patients’ perspectives from one service to other (albeit relatively similar) services.
The lack of well developed expectations is also a finding that warrants further research, especially if patients’ expectations about the roles and outcomes of services provided by other health care professionals are also explored. Additionally, it has implications for the evaluation of satisfaction with pharmaceutical care. For example, a recently validated questionnaire 21 asks patients to assess items such as, ‘How frequently the pharmacist checks with you about how well your medications are working’, ‘How your pharmacist uses information about your previous conditions/drugs when assessing your drug therapy’ and ‘The responsibility that the pharmacist assumes for your drug-therapy’, using a five-point scale. However, our findings suggest that patients do not conceptualize a role for pharmacists in accordance with these statements. A possible strategy to deal with this issue is developing questionnaires based more closely on patients’ conceptions of the service.
Footnotes
Acknowledgements
We are very grateful to all the patients who made this study possible. We are also indebted to community pharmacists that helped recruiting patients. Dr Sarah Crowe's help with quotes translation was instrumental. CEFAR (Centre for Health Evaluation and Research, ANF group) provided valuable logistical and administrative support to this study.