
Abstract
Summary
We developed an integrated care pathway for diabetes identified in pregnancy largely based on National Institute of Clinical Excellence (NICE) CG063 - Diabetes in Pregnancy (2008). As well as providing the integrated care pathway (ICP) for clinicians to consider using in their units, this article describes the process used, and the lessons learned, during the project. The ICP runs from the point of diagnosis to the early postnatal period. It covers glycaemic management, care of diabetic complications, obstetric care (antenatal and intrapartum), thromboprophylaxis and influenza vaccination. It is used by physicians, obstetricians, dieticians, specialist diabetes nurses and specialist midwives. An audit showed a high degree of compliance with a care bundle derived from NICE CG063 (2008). We felt that it systemized our clinical processes and reduced errors of omission. Alongside the production of the ICP, a patient information leaflet was written to support women in making choices during pregnancy and afterwards.
Introduction
Gestational diabetes is well known to contribute significantly to perinatal morbidity and mortality - resulting in high costs physically emotionally and financially. It is known that this contribution can be reduced by tight glycaemic control, monitoring of the fetal wellbeing and careful decision-making about mode and timing of delivery. This is best achieved through input from obstetricians with an interest in maternal medicine and endocrinologists, ideally in a combined clinic where other members of the multidisciplinary team including diabetic nurses and dieticians also provide crucial input. The National Institute of Clinical Excellence (NICE) published guidelines in 2008 to aid clinicians in providing care appropriate to women found to have carbohydrate intolerance in pregnancy. A number of integrated care pathways (ICPs) have been successfully introduced into our unit over the past few years. Recently, an integrated pathway had been developed for the care of women with diabetes identified during pregnancy to sit alongside our pre-existing diabetes ICP. The databases explored during this project were RCOG guideline database, Cochrane database of systematic reviews, Bandolier, SIGN, Clinical Evidence and Medline.
Reasons for and scope of ICP
Diabetes identified in pregnancy covers a wide range of clinical issues involving a large multiprofessional team. The primary purpose of our document was to identify best practice and then inculcate that into the everyday care of women with diabetes identified in pregnancy. One important aim was to provide easily accessible, clear guidance for the wider midwifery team, who might only see one woman each year with diabetes. Furthermore, it was seen as a means of supporting the training of junior obstetricians who have become less experienced with the implementation of the European Working Time Directive. The ICP was designed to aid accurate and comprehensive documentation with the facility for rapid audit.
The scope of the care pathway starts at the point of diagnosis of diabetes and runs until the time of discharge from the hospital. It includes maternity and general medical care and covers issues such as influenza vaccination, contraception and thromboprophylaxis. 1 We titled the document Diabetes Identified during Pregnancy to emphasize that some women might have type 1 or type 2 diabetes. It does not cover the screening programme, which is governed by a separate conventional clinical guideline. The ICP can be found on the International Journal of Care Pathways website (http://ijcp.rsmjournals.com).
Setting
Musgrove Park Hospital in Taunton is a busy district general hospital with 650 acute medical beds. The obstetric unit handles over 3200 deliveries a year ranging from low to high risk. Screening for gestational diabetes is risk factor based as recommended by NICE (2008). Women found to have diabetes during pregnancy are managed in a combined obstetric-endocrinology clinic by consultants with an interest in this field. The clinic is also staffed by diabetes specialist nurses, midwives, dieticians and trainee physicians and obstetricians. Care is complex with numerous facets and a large multiprofessional team. We developed an ICP to ensure care is offered consistently and documented well, according to the national guidance.
Development of the ICP
A small group with representatives of each of the main professional groups met to set out a development timetable. The development team included an obstetrician, a midwife, a diabetologist, a diabetes specialist nurse, a dietician and a sonographer. A trainee obstetrician was included for their own personal development in guideline and care pathway development.
The first task was to set out the care pathway from diagnosis to discharge into the community after delivery. NICE Clinical Guideline 63 (2008) 2 was used as a main reference tool but a search was undertaken of other key evidence-based resources,3-5 particularly with respect to thromboprophylaxis 1 and influenza vaccination. These sources included Cochrane and CEMACH.
Having laid out the care flow, we created a loose framework for the document and then each professional worked independently on their section. The whole document was then brought together. We chose to incorporate the evidence into the ICP in two ways. First, for most of the routine tasks, particularly for those that were repetitive and had fixed time courses, we choose to have formatted checklists and grids that prompted clinical actions and demanded documentation. As part of this approach, tips for best practice were included to guide the less experienced. This included teamwork issues such as instilling the notion for open access to senior doctors and midwives. The second approach, at the front end of the document, was to have a more conventional guideline for rarer clinical events that had no fixed time for action. In addition to formatted sections, we included free-text areas to allow more extensive notes to be written for documentation of variations from the expected pathway.
A patient-group representative worked with us on the document as a reviewer. She recommended having a check box for leaflets and a sticker for emergency telephone numbers. This document is not written in patient-friendly terms and so we worked to produce a six-page leaflet that provided women with a clear interpretation of the care pathway. A key aim of the leaflet is not to tie women into one route but to provide them with information to help them navigate their journey in a way that they wish.
After completion, the first draft was trialled. Team members were strongly encouraged to identify glitches so that new solutions could be found. One particular point that was identified was that postnatal tasks were often not identified before discharge. It seemed that these were simply lost at the back of the document, and the actions overlooked. Therefore, we moved those to the front end of the document. This worked well and we no longer make our ICPs rigidly follow in chronological order. This process continues and updates are made frequently.
One other clear issue we identified was engagement of the wider midwifery team. In future, we would choose to include a labour ward and a postnatal ward midwife to promote inclusiveness, and for them to act as champions during implementation.
Variance analysis and audit
We do not undertake conventional variance analysis. The document is audited on a three-yearly cycle. The first audit was undertaken during 2009 (seeTable 1). This was a case-note review against a care bundle taken from the National standards described in NICE CG063 (2008).
Results of case-note audit (n = 20)
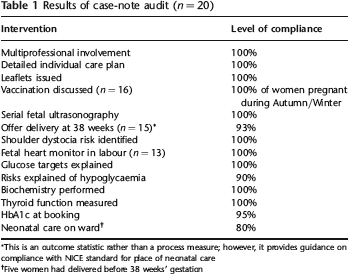
This is an outcome statistic rather than a process measure; however, it provides guidance on compliance with NICE standard for place of neonatal care
Five women had delivered before 38 weeks’ gestation
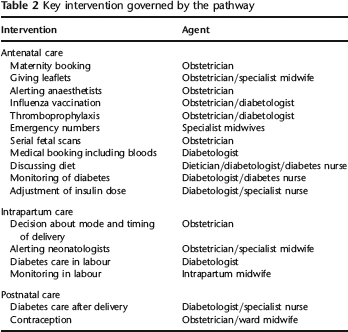
Key interventions
The main issues covered by the ICP are listed inTable 2. From the audit we learned:
The failure to comply with guidance on timing of delivery related to a change in the national standard after the ICP had been issued. This is a particular problem with preformatted notes;
The audit identified areas that we had not included in the original version - explaining risk of hypoglycaemia.
Key intervention governed by the pathway
Lessons learned about ICP production
The discipline of writing an ICP requires a rigorous approach both in terms of finding best practice and also in terms of formatting the document. A well-written document prompts good practice and potentially also makes clinical care more efficient by prompting an organized approach. It is essential that the care pathway guides healthcare workers without limiting the choice for individual patients, however.
There is no substitute for carefully organized ICP production meetings. These should aim to encourage all team members to contribute to practice development, and allow for the identification of simple practical solutions to effective documentation. The process appeared to be good for team morale and the promotion of a multiprofessional care.
Once written, the insertion of new practice guidance is simple and allows rapid adoption of key recommendations. Good notekeeping is promoted by the structure of the document. Sections on later pregnancy tasks were less complied with, possibly because of their placing at the end of the document. It is important to provide free-text for occasions when care diverts from expected pathway. The formatted structure facilitates audit by information being recorded in set positions.
Finally, once the ICP is introduced, it has to be updated in line with new national guidance. With the introduction of newer versions, there is a problem of existing patients continuing with earlier (out-dated) versions. Stickers can be used to highlight this.