
Abstract
There is a high prevalence of leprosy in the Amazon region of Brazil. We have developed a distance education course in leprosy for training staff of the Family Health Teams (FHTs). The course was made available through a web portal. Tele-educational resources were mediated by professors and coordinators, and included the use of theoretical content available through the web, discussion lists, Internet chat, activity diaries, 3-D video animations (Virtual Human on Leprosy), classes in video streaming and case simulation. Sixty-five FHT staff members were enrolled. All of them completed the course and 47 participants received a certificate at the end of the course. At the end of the course, 48 course-evaluation questionnaires were answered. A total of 47 participants (98%) considered the course as excellent. The results demonstrate the feasibility of an interactive, tele-education model as an educational resource for staff in isolated regions. Improvements in diagnostic skills should increase diagnostic suspicion of leprosy and may contribute to early detection.
Introduction
Leprosy is an infectious disease caused by Mycobacterium leprae. It is endemic in several regions of Brazil and represents a high priority disease for the Ministry of Health. Of the 66,079 cases of leprosy recorded in 2006, 25,223 cases (38%) were in the Amazon region. This represents about 20% of all world cases. The disease is often difficult to recognize in the early stages and a large number of patients remain undiagnosed. 1
Health professionals are unevenly distributed in Brazil. The northern region has about 17,000 doctors to meet the needs of over 14 million inhabitants. This ratio is more than seven times lower than in Sao Paulo City. As a way of improving health care, the Brazilian Ministry of Health has developed Family Health Teams (FHTs), involving multidisciplinary cooperative groups with doctors, nurses and nursing technicians/assistants. 2 However, in a large country such as Brazil, it is difficult to provide continuing education and ensure properly qualified staff. Even though diagnosis and treatment are medical actions, anyone could be trained to recognise early leprosy, including non-medical FHT professionals.
We have developed a distance education course in leprosy for training FHT staff. The main objectives of the course were to improve early diagnosis/suspicion of leprosy.
Methods
The course was developed in accordance with the requirements for University Extension Courses at Sao Paulo University. The course was managed by the Discipline of Telemedicine at Sao Paulo University's School of Medicine (DTM-SPUSM) as part of the Telehealth Primary Care Project of the Ministry of Health. It was developed in conjunction with Amazonas State University and the Alfredo Matta Institute (Northern Region Leprosy Reference Institution) in Manaus, and the Parintins Municipal Health Secretary, in Parintins, all in Amazonas State.
The course was made available through the Sao Paulo Telehealth Portal (
Access portal to the course (
Tele-educational resources were mediated by professors and coordinators, and included the use of theoretical content available through the web, discussion lists, Internet chat, activity diaries, 3-D video animations (Virtual Human on Leprosy), classes in video streaming (Figure 2) and case simulation. Supplementary literature was suggested to students, and included government recommendations on treating leprosy patients and relevant scientific articles.
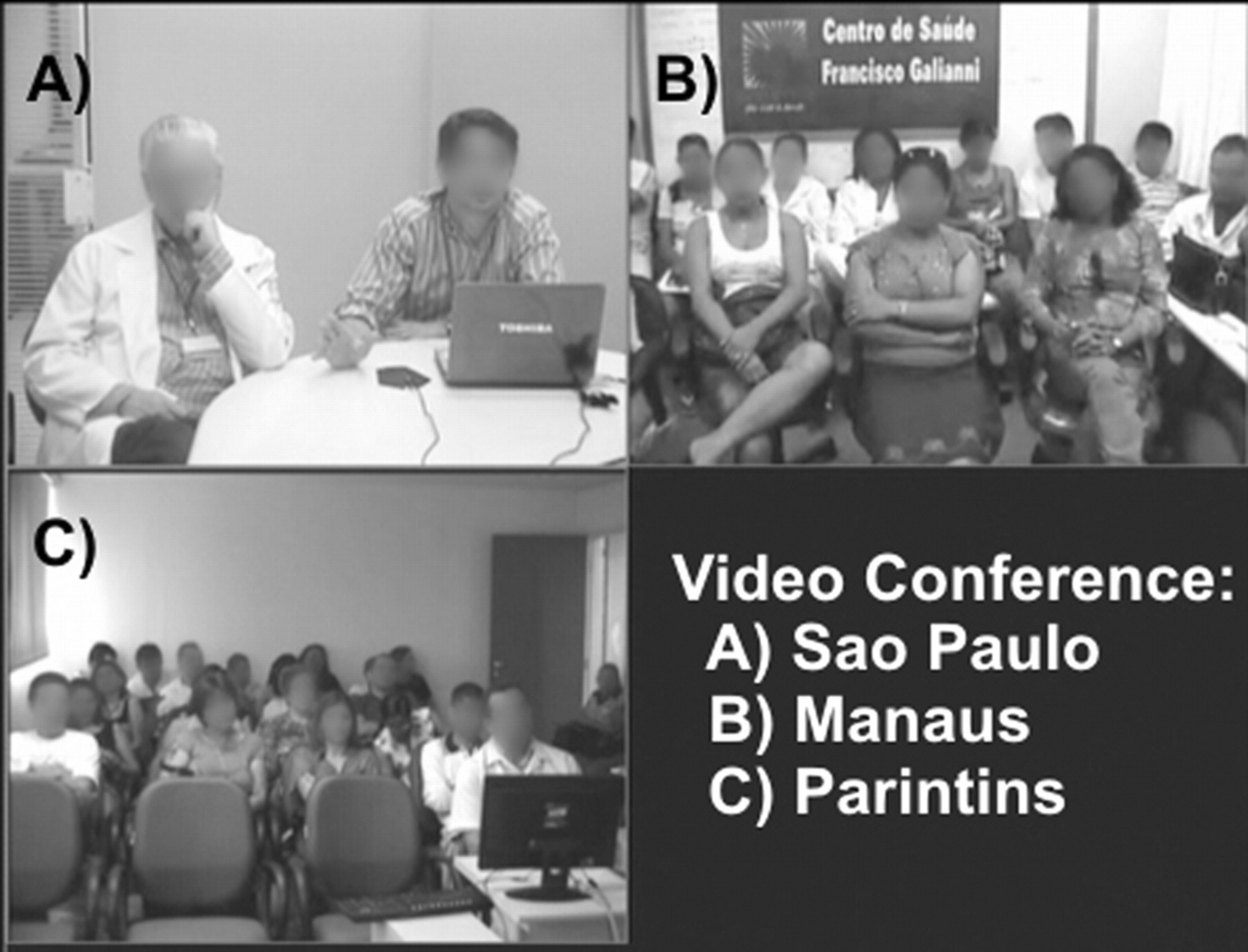
Videoconference between Sao Paulo, Manaus and Parintins
Discussion lists and Internet chat rooms were divided into four leprosy themes: aetiological agent and transmission, epidemiology, clinical aspects and treatment. The discussion lists were designed to be accessed periodically. Students recorded their participation in activity diaries.
The Virtual Man is a learning object that uses 3-D computer graphics. The video, which lasts for about 4 min, emphasizes early signs and symptoms of leprosy. During the course, this could be accessed using video streaming or via a CD. Important aspects for the suspicion of the disease were shown, such as hypopigmented patches with impaired sensation, loss of sweating and hair loss.
A Leprosy Case Simulator (LCS) was developed, based on the concept of clinical cases. It emphasised suspicion and diagnostic assessment of the disease. Information from ten experienced dermatologists was categorized by relevance, forming the Nucleus of Essential Information (NEI) in the LCS. Half the content in this nucleus gave particular attention to suspicion and diagnosis, and included presentations on the indeterminate and polar forms of leprosy. The LCS contained 20 multiple choice questions about aspects of professional practice, which was answered at the end of the course. The flow chart of the LCS is shown in Figure 3. An overall participation of more than 70% in course activities was expected, including in the LCS. If this occurred, the student was awarded a certificate of completion.
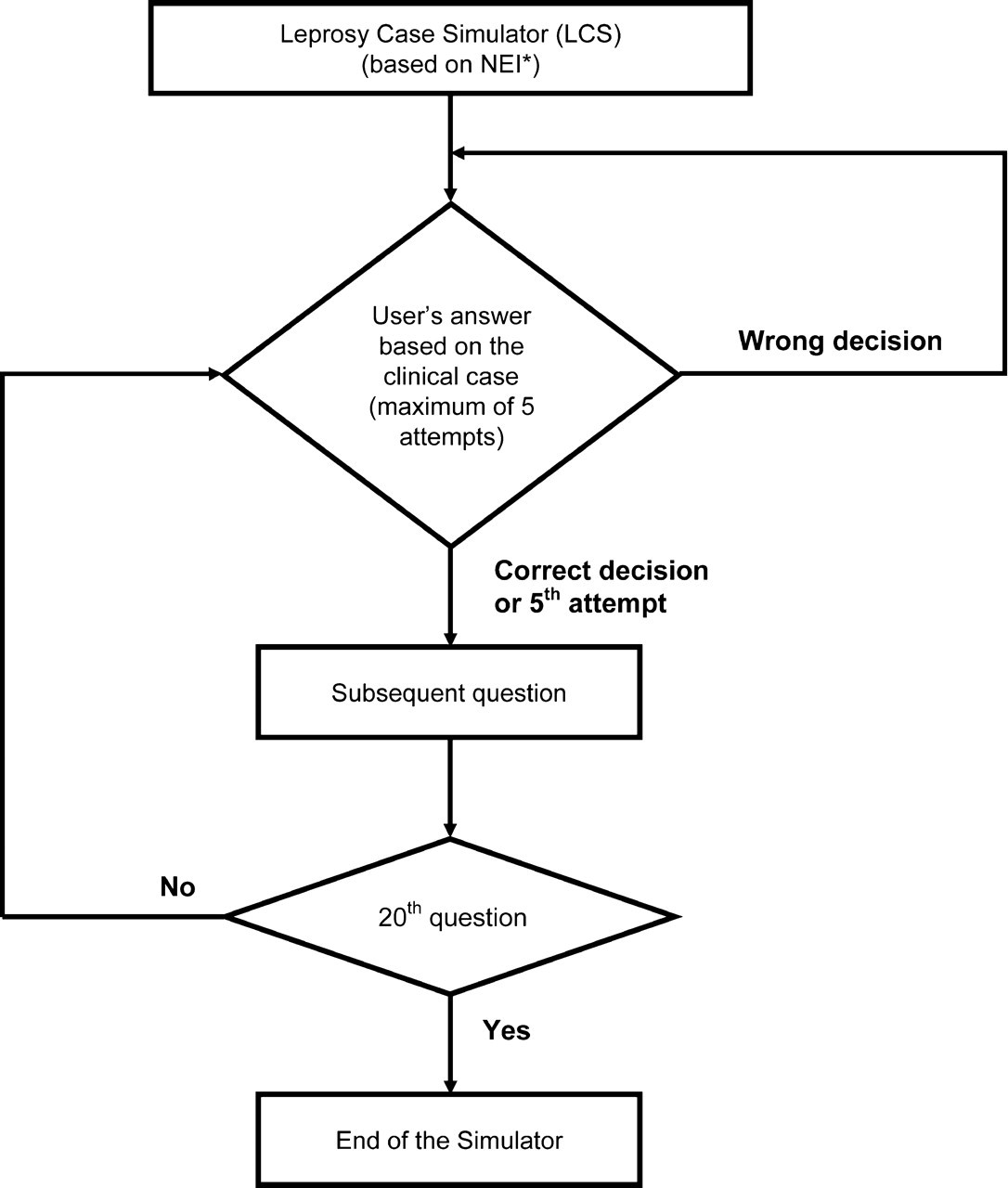
Flow algorithm for using the Leprosy Case Simulator (LCS)
After a period of one year, 32 participants re-answered the same LCS to verify their long memory.
An instrument was designed to evaluate motivational aspects of the course. It was based on the validated questionnaire called the Web Site Motivational Analysis Checklist (WebMAC). 3 With the permission of the authors, some questions were adapted for the tele-education course. Standard statistical software was used for analysis (SPSS 15, SPSS Inc., Chicago and Bioestat 4, Sociedade Civil Mamirauá, Belém).
Results
Sixty-five FHT staff members were enrolled. All of them completed the course and 47 participants received a certificate at the end of the course. Table 1 shows the occupations of the participants and their interaction activities during the course. Of those who were not approved, 10 were nurses (63%), 7 (33%) were nursing assistants/technicians, and 1 (14%) was a doctor.
Participation in discussion lists, Internet chat sessions and activity diaries. There was no significant difference (P > 0.05) between participation of the professionals in the activities using the G test (Willians)
aOthers: 1 biochemist, 1 physiotherapist, 1 biologist
bMean participation in the interactive activities represents the total participation for each professional group divided by the number of participants in that group
The 108 questions posed by the students on the discussion lists were answered within 48 hours. The Internet chat sessions were held at weekends. A total of 16 hours were dedicated for videoconferences between Manaus, Parintins and Sao Paulo. The conferences were supervised by the course coordinator and teachers. During the final videoconference, the students stated that the videoconferences were extremely important to the course's success, giving them the opportunity to interact in real time.
Students requested a larger number of videoconferences and Internet chats, and the number of hours provided for the course had to be doubled (extended to 60 hours with an average of 1.4 hours per day). There were no difficulties in understanding the content mentioned during the videoconferences, regardless of the participants' education level. At the end of the course, 48 course-evaluation questionnaires were answered. Most participants (98%) considered the course as excellent.
Table 2 shows the performance according to professional group. The doctors had the lowest mean number of attempts to complete the LCS and the nursing assistants/technicians had the highest. Using the Kruskal-Wallis and post-hoc Student-Newman-Keuls tests, showed that the nursing assistants/technicians had an inferior performance compared to doctors and nurses. More than 75% of the LCS questions were answered correctly at the first attempt, with a significant difference (P < 0.01) from two or more attempts. There were 15 participants who required all five attempts to complete the LCS.
Mean number of attempts at the LCS by the different professional groups
After a period of one year, the participants re-answered the LCS. There was no significant difference from the results obtained at the end of the course.
Discussion
Improvements in diagnostic skills should increase diagnostic suspicion of leprosy and may contribute to early detection. These are considered critical by the WHO. 4 Improved care quality is also important to eliminate this endemic disease. 5,6
Subjects like student autonomy, collaborative participation, interactivity and dialogue were encouraged during the course. High attendance in Internet chat sessions, discussion lists and activity diaries demonstrated the course's interactivity. These resources enabled deeper exploration of the theory, and encouraged valuable discussions that generated essential reflections on the learning process for both students and tutors. In addition, the videoconferences were very important for clarifying goals in each of the activities, course realignments, date and deadline adjustments, as well as promoting dialogue which directly motivated the participants. 7
The Virtual Man conveys knowledge in a very rapid and simple way. 8,9,10 This leprosy title was developed with the Brazilian Ministry of Health via the Pan American Health Organization and is freely available. The CD-ROM only requires translation from Portuguese. Following the course, this learning object can be used by students themselves for teaching purposes. Therefore its availability to the whole community will promote health education.
The theory of andragogy was developed by Malcom Knowles. 11 In a different way from pedagogy, it represents the process of engaging adult learners in the structure of the learning experience. The LCS represents an environment for knowledge evaluation with strategic questions about the disease, where a practical emphasis was given and defended by andragogy. Thus, it allows a contextual approach focused on diagnosis/suspicion. Relevant points, such as the prevalence of leprosy, importance of early treatment and population awareness, were highlighted by the NEI. In addition, a perspective of patient care 4,5,6 was also considered when developing the case simulations.
Unfortunately, not all students met the criteria for approval. Difficulty in understanding content did not appear to explain the different levels of failure among the groups, as it was not mentioned by the students.
Participants were divided into two professional groups. The graduate group was represented by doctors, nurses and other professionals. The undergraduate group was composed of technicians/auxiliaries. After the course, doctors and nurses had a better knowledge performance.
The learner's motivation has direct effect on learning. 12,13 Moreover, receiving of a university's certificate was an additional stimulus for students. Another important motivational factor was the possibility of interacting with experienced teachers. These were reported in the students' comments during videoconferences. High satisfaction reached in the course was confirmed with the modified WebMAC questionnaire.
Medical, public and paramedical educational strategies can contribute to early and correct diagnosis of leprosy, and assist with the demystification of the disease. Disease eradication is an action that depends on multiple actions, regarding better basic sanitation, effective primary health care, good nutrition and hygiene. These produce an overall improvement in population life quality.
It is important to follow a planned strategy, including teaching fundamentals and educational evaluation. Our course was planned based on key pedagogical fundamentals and the LCS represented a useful evaluation tool. The feasibility of this educational model for FHT staff was proved, providing knowledge through the use of interactive technologies and involving long distances.
Currently, all states of Legal Amazon are able to use this strategy. Current developments, such as the National Telehealth Programme and improvements in the communication infrastructure of the Brazilian University Telemedicine Network Project, will facilitate delivery of the leprosy and other distance courses for continuous health education.
Footnotes
Acknowledgements
We thank the students. We are also grateful to Luiz Jorge Fagundes, Maria Angela Trindade, Cyro Festa Neto, Cleinaldo de Almeida Costa, Francisco Tussolini and Marcelo Minoru Onoda.