
Abstract
Hearing loss is the most prevalent chronic disability and a major contributor to the global burden of disease. Its effects are far-reaching and can lead to severely restricted developmental outcomes for children and limited vocational prospects for adults. The benefits of intervention are dramatic and can significantly improve developmental outcomes, especially in infants identified early. Hearing health-care services in developing regions such as sub-Saharan Africa are however severely limited, leaving affected individuals without access to secondary and tertiary intervention. Tele-audiology has potential for improved access to specialist hearing health services including identification, diagnosis and intervention. There has been limited experience so far with tele-audiology in industrialized countries. In the sub-Saharan region, the continued growth in Internet connectivity and general technological advances make tele-audiology an important approach to consider in the management of hearing loss. Pilot studies are warranted to investigate the potential obstacles to the widespread implementation of telehealth in the delivery of hearing health care in poorly-resourced communities, in line with World Health Organization initiatives.
Introduction
Hearing loss is the most prevalent chronic disability, and is present in almost 10% of the global population to a mild or greater degree. 1,2 More severe hearing loss (moderate to profound) affects 4.3% of the world's population. 2 The effects of hearing loss are far-reaching and apart from the negative consequences for socio-emotional wellbeing and participation, also result in severely restricted developmental outcomes for children and limited educational and vocational prospects for adults. 3 In developing regions such as sub-Saharan Africa (SSA) these consequences may be even more serious due to a vicious cycle where poverty predisposes to hearing loss and hearing loss predisposes to poverty. 4 Not only are the consequences serious, but the prevalence of hearing loss is greater due to increased environmental risk factors and poorer maternal health care. For example, congenital or early-onset infant hearing loss in developing countries is estimated to be twice as high at 6 per 1000 live births compared to 2–4 per 1000 for industrialised countries. 1,4,5
Hearing loss ranks as the third largest global contributor to the loss of healthy life due to disability and is one of only four non-fatal conditions among the leading 20 causes of the global burden of disease on the Disability Adjusted Life-Years (DALY) index. 1 These estimates only include adult-onset hearing loss, and the inclusion of childhood hearing loss will significantly increase the global burden. 5
Current approaches to hearing loss management
Interventions for hearing loss, such as the early detection of infants with hearing loss and the provision of hearing devices, offer developmental outcomes that are similar to those in people with normal hearing and integrated societal participation. 3 Unfortunately globally coordinated initiatives are still quite limited, particularly in developing regions such as SSA, which account for more than 80% of the hearing loss disease burden. 2 Global efforts to address hearing loss in this region have mainly focused on primary prevention to reduce preventable causes of hearing loss. As a result, most individuals with hearing loss remain without secondary and tertiary intervention services.
A major hurdle to the development of the necessary intervention services is the limited access to hearing health-care professionals and associated support. In most of SSA, services are either totally absent or extremely limited and constrained to specific areas. Hearing health-care professionals such as otolaryngologists and audiologists are in very short supply in SSA. In contrast to Europe, where there is typically one otolaryngologist for every 10–30,000 people, in SSA there may be 250,000 to 7.1 million people per otolaryngologist. 6 The number of audiologists may be even smaller: many countries in SSA have no audiologists and only one of the 46 countries offers tertiary training for a professional audiology qualification. Access to hearing health care, which is inextricably linked to the number of professionals providing the services, is wholly inadequate. This has prompted a reappraisal of the current approaches to the delivery of hearing health-care services.
Potential role of tele-audiology
Tele-audiology has a potential role in improving access to services. Currently its use is limited, despite initial reports of tele-audiology applications with test validity and accuracy equivalent to face-to-face services, e.g. video-otoscopy; pure tone audiometry; tympanometry; otoacoustic emissions; auditory brainstem responses; hearing aid verification and cochlear implant mappings. 7–11 Hearing can be assessed at a distance with portable tele-audiology devices and appropriate software, using low bandwidth telecommunication and without the need for sound booths which are not commonly available in SSA. Test compliance, during device set-up and calibration and testing can be monitored remotely through audio and/or video feedback and appropriate hardware and software. The need for expensive sound booths, can be largely overcome by using tele-audiology devices that integrate live monitoring of environmental noise, sound attenuation using insert and circumaural earphones, and active noise cancellation. 11 Available intervention options such as hearing aid fitting and verification can be performed remotely using appropriate software and application sharing. 10 Counselling, follow-up and rehabilitation services can be facilitated through videoconferencing facilities or interactive Internet-based programs.
With improving connectivity in developing countries, where service providers are rare and hearing evaluations are primarily equipment-based, the prospect of tele-audiology to provide remote services for screening, early detection and intervention of hearing loss and education is particularly appealing. Educational applications may include interactive online modules to facilitate continued professional development and training of paraprofessionals, parents or patients themselves. Support may also be provided remotely via online interactive or on-demand training and second-opinion services. Tele-mentoring of local professionals or para-professionals is another valuable application which may serve to develop local skills and expertise.
System architecture for tele-audiology
The basic infrastructure for tele-audiology comprises both hardware and software with Internet connectivity. A typical system architecture is illustrated in Figure 1. Clinical hearing evaluation and intervention can be performed in real-time (i.e. synchronously) through devices operated remotely, using computer application sharing combined with videoconferencing. The software can be desktop- or laptop-based, utilizing voice-over-Internet and webcam applications that are inexpensive and easily accessible.
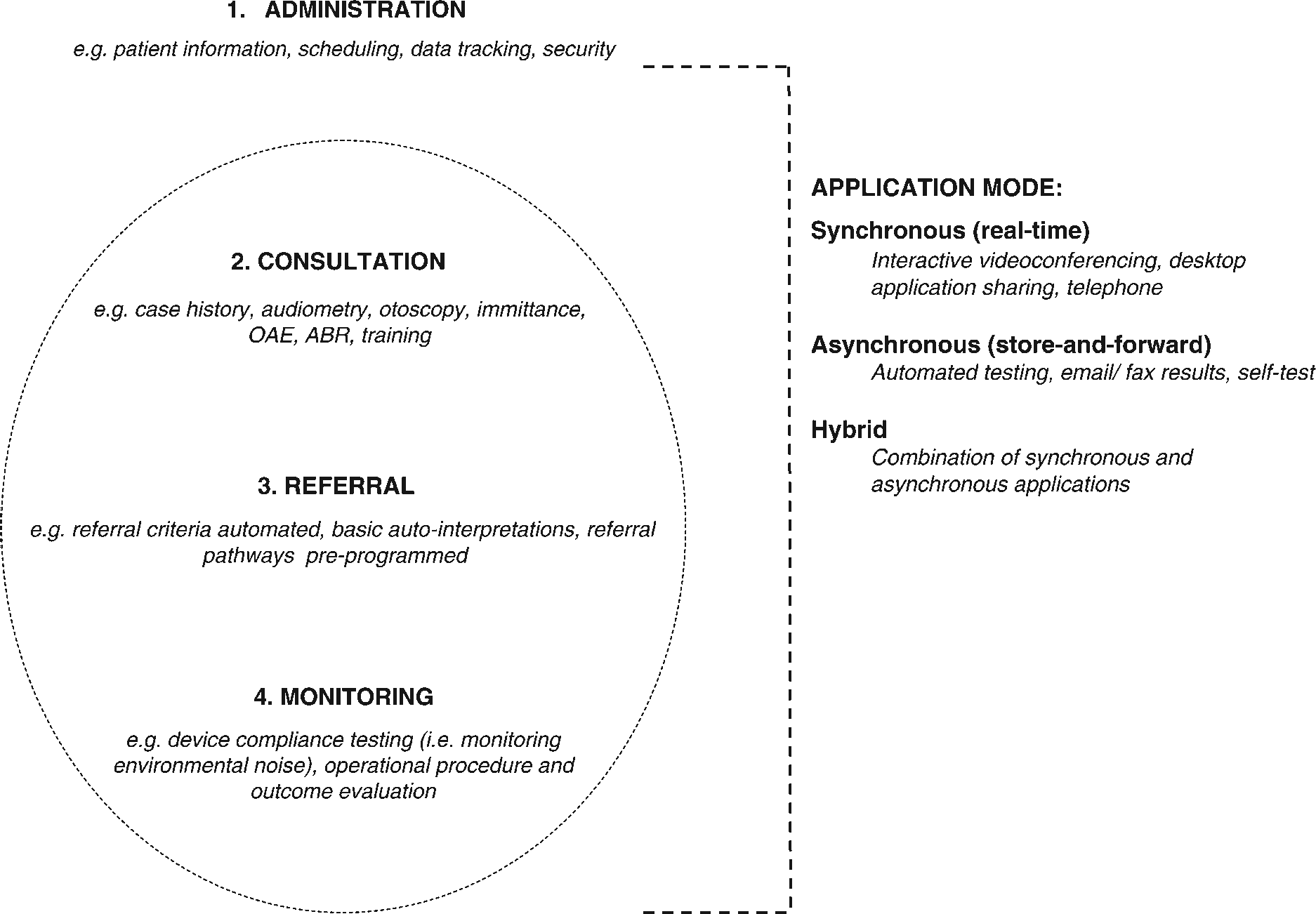
Teleaudiology system architecture and application modes
In SSA, the use of store and forward applications with automated testing and calibration procedures may be the most appropriate model for providing tele-audiology services. This approach can enhance time- and cost-efficiency by reducing the requirement for face-to-face health-care service by a specialist and by reducing the requirement for costly Internet bandwidth. For example, automated computer-based hearing screening and threshold tests, facilitated by a paraprofessional, can be conducted at remote locations. This reserves the need for real-time tests by a specialist, for difficult cases. Other clinical procedures, like an otoscopic examination, can be performed by a trained paraprofessional using a video-otoscope, with digital images referred to a specialist by email, for diagnosis. A combination of both synchronous and asynchronous approaches may also be useful in some settings.
Potential drawbacks and challenges
Tele-audiology in SSA offers the general population and in particular children, improved access to specialist hearing health services. It is likely to facilitate a greater awareness and knowledge of hearing health care among primary care providers, most of whom will never have a chance for formal training. However, tele-audiology is not a panacea, especially in low income countries. For example, it may distract from the pursuit of expertise in audiology through formal training, ultimately producing a group of uncertified audiologists or ear care specialists who are only proficient in the use of the supporting technology. Challenges for the widespread implementation of tele-audiology will be technical, organizational/infrastructural and socio-cultural in nature. For example, connectivity may be hampered by the lack of a reliable electricity supply, even in urban areas in some developing countries. The economic implications and the cost-effectiveness of tele-audiology in different settings are not yet known. Concerns about data security, patient privacy and cultural inertia to modern gadgets or technology-driven care, even among health workers, also need to be addressed. Internet penetration in SSA, although growing rapidly, remains low, with only 3.5% of the population having access to the Internet. 12 Furthermore, very few countries have any e-health policy, strategy or legislation. These challenges are not limited to tele-audiology, of course. For example, one report on the World Health Organization (WHO) African Region cited low school enrolment, high illiteracy rates, low per capita incomes, widespread poverty and weak ICT connectivity as posing major challenges to the effective utilization of e-health services. 13 The current efforts led by the WHO to promote e-health globally, in collaboration with national governments, are likely to benefit hearing health-care delivery as well.
Conclusion
The increasing global burden of hearing loss, largely unaddressed by present global health funders, NGOs and governments, demands a critical reappraisal of traditional approaches to hearing health-care delivery in developing countries. The global revolution in connectivity and the continuing advances in technology mean that tele-audiology is becoming an important approach to bring hearing health care to the underserved in SSA. Pilot studies are warranted to investigate the potential obstacles to the widespread implementation of telehealth in the delivery of hearing health care in poorly-resourced communities, in line with WHO initiatives.