
Abstract
We conducted a systematic review of the literature on telehealth in Asia. The Medline database was searched, together with three specialist journals, for peer-reviewed articles published in the ten years to June 2007 which were related to any telehealth application involving one or more Asian country. Out of the 1504 abstracts retrieved, 109 articles were selected by two independent reviewers for the final review. The number of published articles on telehealth in Asia increased during the review period. The largest number of studies were conducted in Japan (37%). Most telehealth applications were based on the store-and-forward modality (43%), with 35% using videoconferencing and 15% using a hybrid approach. Most of the studies were descriptive (75%) and only eight included a control group against which telehealth was compared. The most common means of telecommunication was ISDN lines, which were employed in 32% of the studies. Some 40% of the studies mentioned improved quality of health care; about 20% mentioned improved access to health care. Although most studies mentioned cost, only 13 of them assessed resource utilization and cost. The overall findings gave a generally optimistic picture of telehealth in Asia. However, there is a lack of good quality studies.
Introduction
Telemedicine and telehealth have been used in industrialized countries for a number of years, especially in North America, Australia and Europe, where a substantial body of literature has emerged about their successes and failures. 1 However, this literature cannot be generalized to the Asian region. Asia contains nearly 60% of the world's population 2 and has different demographics and problems from other regions. Moreover, the Asian literature on telehealth is scant when compared to the literature of the west. 1
We have attempted to gather all the literature on telehealth in Asia and to analyse it for evidence about the efficacy and utility of telehealth.
Methods
We conducted a systematic review as outlined in the Cochrane Handbook. 3 The review was performed in five steps:
Stage 1: Selection criteria for studies and the literature search. The search keywords were: telemedicine, telehealth, real time telehealth, store and forward telehealth, e-health, information and communication technology, developing countries, distant conferencing and Asia. The Medline database was searched using the PubMed search engine for the period January 1997 to June 2007. Three telehealth related journals were searched by hand: Journal of Telemedicine and Telecare, Telemedicine Journal and E-health and E-health International Journal. The inclusion criteria included articles in English, with humans as subjects, published between January 1997 and June 2007, and related to any sort of telehealth applications involving at least one Asian country where the intervention took place. The studies had outcomes in terms of administrative changes (management and policy), patient outcomes (i.e. increased access to health-care services and improved quality care) or economic effect. Duplicate articles were excluded.
Stage 2: Review of the abstracts (Level 1 review). Each abstract was reviewed independently by two reviewers. The selection of relevant articles was based on the information obtained from the study titles and the abstracts, according to the inclusion criteria mentioned in stage 1. We also confirmed that the research had been conducted in one or more Asian countries. Each reviewer independently screened the abstracts. If the two reviewers differed, a mutual agreement was achieved. If disagreements persisted, the full publication was obtained for detailed review.
Stage 3: Review of the complete articles (Level 2 review). The same reviewers extracted data independently and where there were disagreements, the differences were resolved by consensus. Data were extracted on the: (1) general characteristics of the studies; (2) telehealth technology; (3) methodological characteristics; and (4) main findings. Reference lists of included studies were also searched for other relevant studies. A number of studies were excluded during the level 2 review when they failed to meet the inclusion criteria on detailed examination.
Stage 4: Quality assessment. The quality of each study included in the review was assessed using the nine-level classification of Jovell and Navarro-Rubio. 4,5 The quality of studies was judged mainly by the study design and use of any controls. However, consideration was also given to the objectives of the study, approach and type of economic evaluation (in case of an economic study), results and conclusions. Any significant limitations of the studies, if mentioned by the authors, were also noted.
Stage 5: Syntheses of data and analysis. Assessment of the articles was done by grouping them on the basis of processes (management and policy), patient outcomes (i.e. increase access to health-care services, improved quality care) and economic effect.
Results
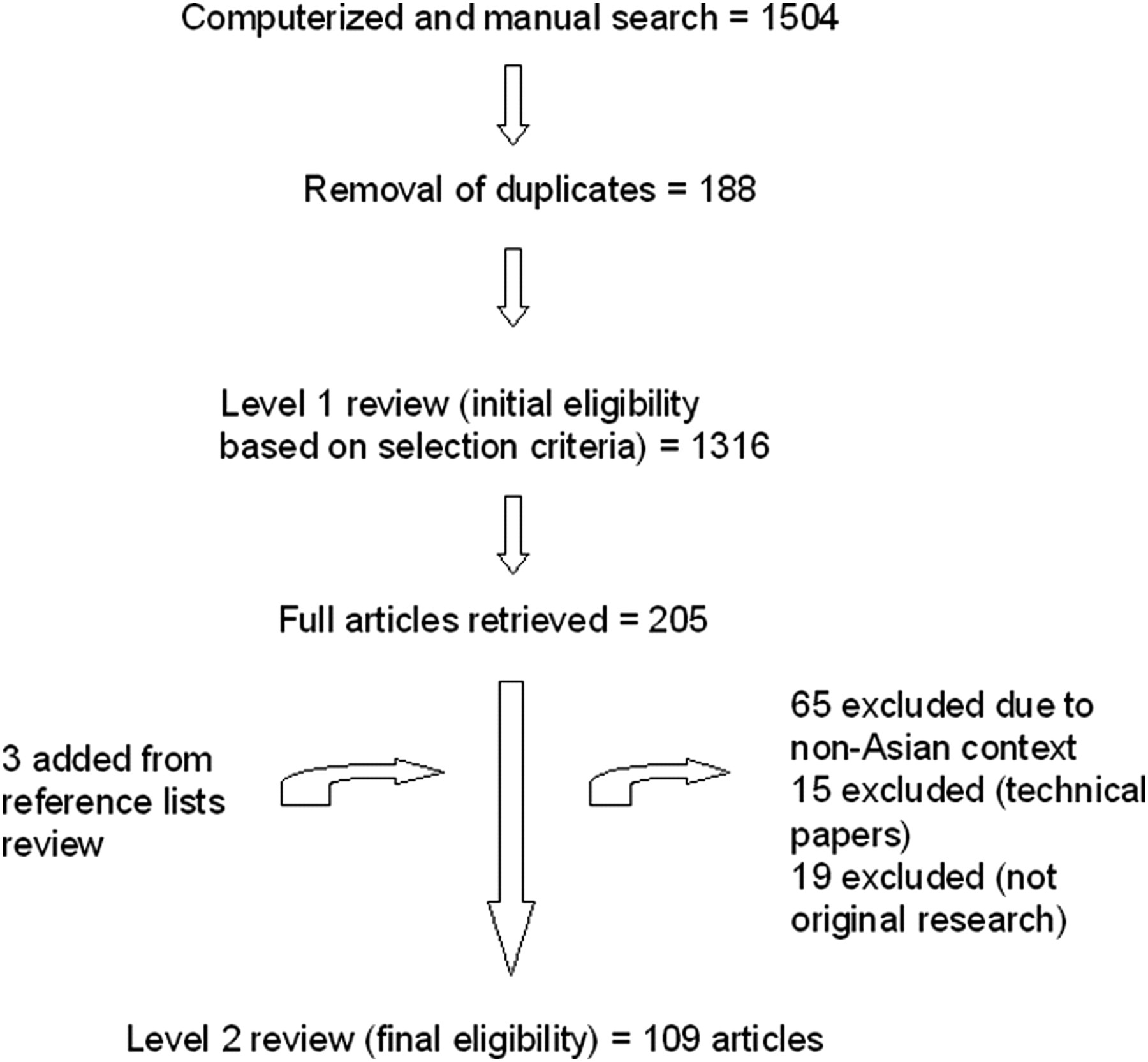
In total, 109 articles on telehealth in an Asian context were identified. The search and selection process is summarised in Figure 1. The results of the review are presented in the following three sections:
Descriptive information; Methodological characteristics; Content and outcome analysis. The search and selection process
(a) Descriptive information
The number of published articles on telehealth in Asia increased during the review period. The highest number of papers published was in 2006 (see Figure 2). The largest number of published studies were conducted in the Japan (37%), followed by India (9%) and Hong Kong (8%). Almost 30% of the studies were conducted in other Asian countries (see Figure 3).
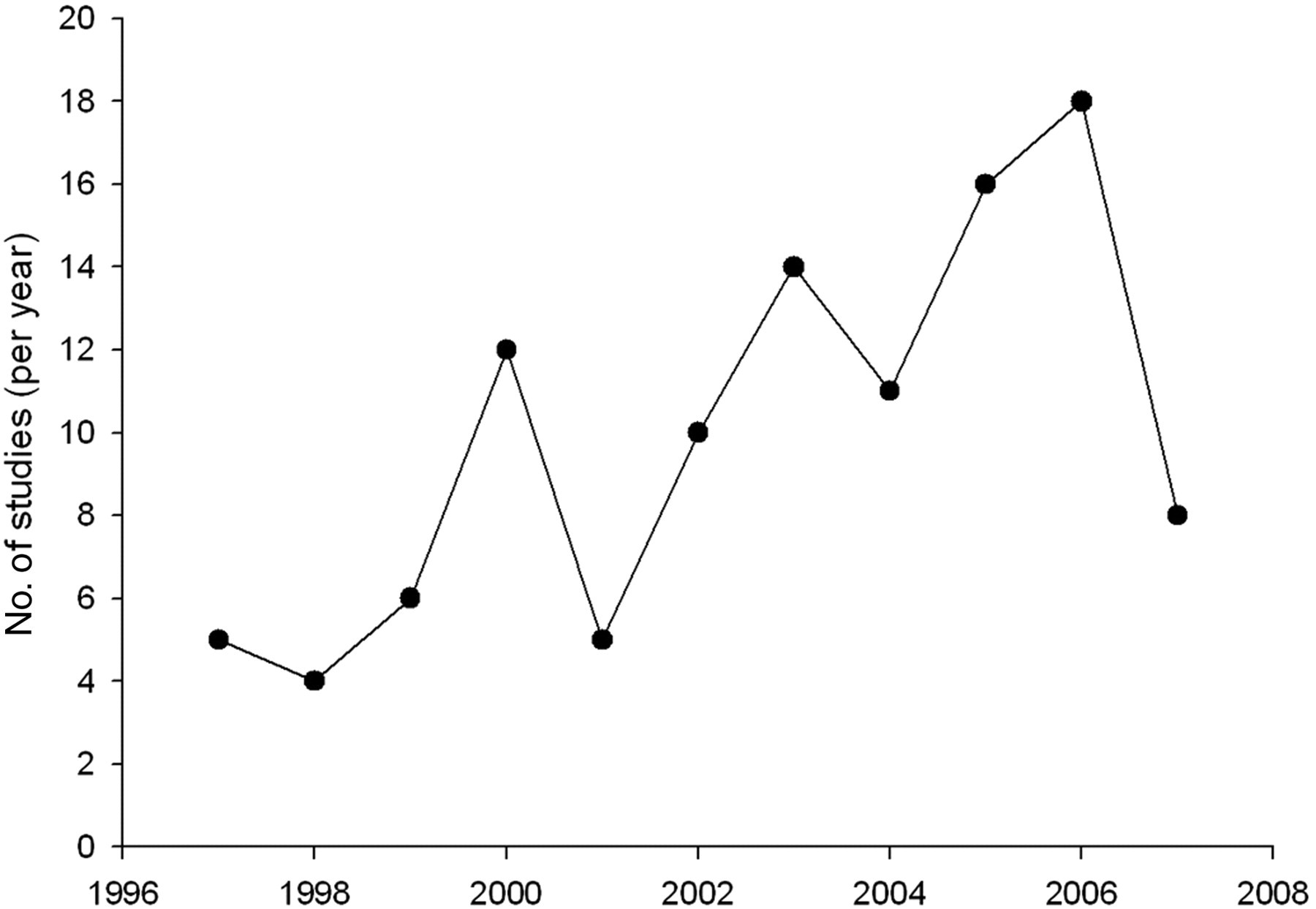
Number of studies
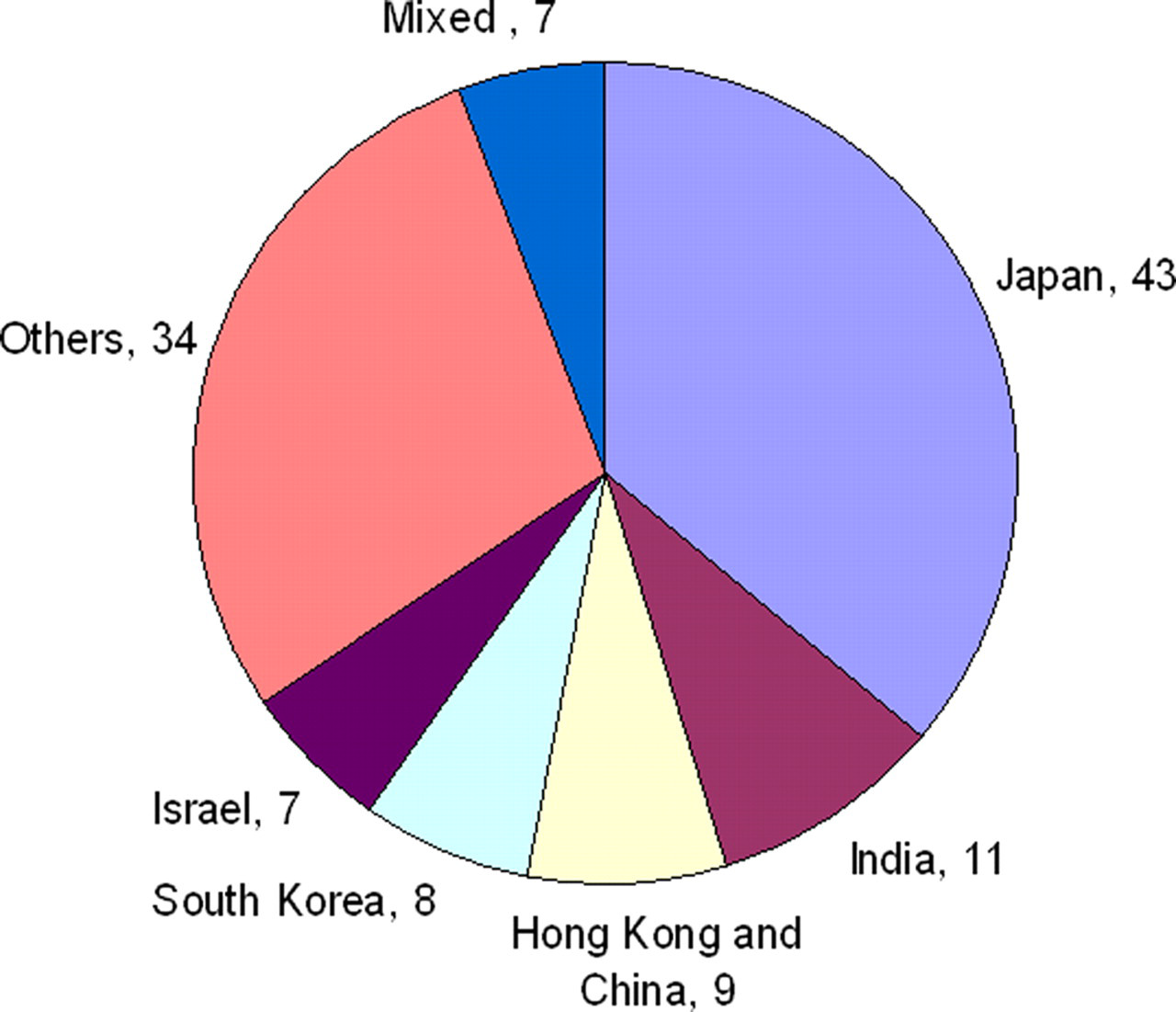
Countries involved in telehealth (n = 119). If two Asian countries were involved, they were placed in the mixed countries group
Study settings
Most of the 109 studies were in urban areas (63%); the remainder were in rural areas (26%) or in both urban and rural areas (11%). The majority of the studies were hospital-based (46%), followed by studies conducted in community settings and primary care level (31%), studies involving home-based settings (16%), ambulatory care settings (4%) and military settings (3%). All of the home-based studies took place in more developed countries of Asia, i.e. 13 studies were held in Japan, 6–18 two in Taiwan 19,20 and one in South Korea. 21
Medical specialty
Telehealth was more frequently used in disciplines such as radiology for orthopaedic and neurology problems (17%), home telehealth (12%), ophthalmology (7%) pathology (6%), emergency medicine (5%) and cardiology (5%). The other specialties (26%) included endocrinology, nephrology, dermatology, surgery, oncology, nutrition, nuclear medicine, rehabilitation, orthodontics and paediatrics. The remaining 22% of the studies involved two or more medical disciplines.
Modality
The majority of the 109 telehealth applications were based on store and forward telemedicine (43%). The main equipment used in these non-real time consultations was a digital (still) camera and a PC. There were 39 studies using videoconferencing (35%). There were additional studies combining videoconferencing with store and forward technologies (15%). The remaining 8 articles (7%) did not describe the use of any system; they were either qualitative or economic analyses of the telehealth interventions.
We used the World Bank Atlas criteria 22 and divided the Asian countries into two groups according to their 2006 gross national income (GNI) per capita. The high income and upper middle income economies were classed as developed countries, and the lower middle and low income economies were categorized as developing countries.
Out of the 39 real time studies, 31 studies were conducted in developed countries, whereas the remaining 8 studies were conducted in developing countries. Out of the 47 store and forward studies, 22 studies were from developing countries, whereas the remaining 25 studies were from developed countries.
Technology
Only 30% of the 109 studies reported the name of the software used in teleconsultation. Open source software was used in 14% of studies, followed by proprietary software (10%) and in-house software (6%). The most common means of telecommunication was ISDN lines, which were employed in 32% of studies. Other means were conventional telephone lines (15%), satellite connections (14%), broadband (14%), mobile phone or other wireless methods (6%). The remaining 19% of the studies did not report the type of connection (see Table 1).
Countries and the use of technologies
*Others include Bangladesh, Kuwait, Nepal, Afghanistan, Iraq, Pakistan, Bhutan, Thailand, Jordan and Turkey
(b) Methodological characteristics
Study design
Most of the 109 studies were descriptive (75%). The studies included surveys, case reports, case studies, feasibility studies, cross-sectional studies and pilot projects. Only eight studies (7%) included a control group against which telehealth was compared. Three of these were randomized controlled trials (RCTs), 20,23,24 four were case control studies 14,21,25,26 and one was a non-randomized clinical trial. 27
There were also 11 studies (10%) with some economic or cost analysis, seven studies (6%) with some qualitative component and three validation studies.
Sample size
Determining sample sizes for individual studies/projects/pilot projects was complicated, as it was often unclear whether the reported sample size referred to: (a) the number of patients offered/receiving telemedicine service; (b) the number of referrals made; (c) the number of images/cases sent; (d) the number of teleconsultations done; (e) the number of institutions where telehealth initiatives were taken. Response rates were frequently omitted from the reports. Sample sizes ranged from a single subject to 511 patients; less than 10 to 1503 teleconsultations made; 20 to 1708 images and from 8 institutions to 622 institutions (both public and private) (see Table 2). 6,28–32
Sample sizes used in different study designs
Quality of studies
As no meta-analysis was done in any of the studies, none of the studies met the criteria of Level 1 evidence (see Table 3).
Strength and level of evidence, based on the criteria of Jovell and Navarro-Rubio 5
(c) Content and outcome analysis
The review attempted to categorize outcomes in five groups, i.e. access, quality, cost-effectiveness, change management and policy issues. It was difficult to separate outcomes into definitive subgroups. Some studies defined good quality of care as rapid provision of care (i.e. rapid access), while others considered that consultation from a specialist doctor represented access to care. Similarly quality of health care was judged on the basis of patient satisfaction, on provider satisfaction or on accuracy of diagnosis. A brief synopsis follows.
Improved quality of care
Approximately 40% of the 109 studies mentioned improving the quality of health care provided. The perceived ability of telehealth to provide for patients' health-care needs and also from the provider's point of view was an important predictor of patient/provider satisfaction. 6,11,25,29,33–35 Telehealth was useful for providing high quality care to patients through consultation, diagnoses, on-time hospitalization, changing patient care, increasing patients' knowledge and maintaining good health, but not for curing disease. 36–41 Some of the reports, however, did not draw definite conclusions, and recommended further studies involving larger samples and longer duration of investigation. 42–47
Improved access to care
About 20% of the 109 studies mentioned improved access to health care and health-care services, i.e. decreased travel, time saving to obtain the required quality care or gaining access to a specialist.
Store-and-forward techniques were found to be easy to implement as all necessary images for discussion could be transferred easily and quickly. 10,29,39,41 This was acknowledged as a potential method of redistributing and sharing medical resources between two countries. Store-and-forward email consultative support for mobile non-physician health-care workers was seen as a feasible method of delivering care in the developing world. Real- time technologies like videoconferencing were found to be expensive, although the costs involved in any project were small in relation to the potential health benefits. 46,48–54
Cost-effectiveness/minimization
Although most studies mentioned cost, only 13 of them (12%) assessed explicitly the effect of telehealth on resource utilization and cost.
In real-time telehealth, higher costs were associated with videoconferencing compared to audio conferencing. The element of cost in any telehealth initiative was also found to be the main concern for most of the countries (especially developing ones) in Asia. 6,11,25,55,56 Even in better developed countries like Japan and South Korea, the high costs associated with the new techniques raised serious questions about the sustainability of telehealth. 56 Most of the studies concluded that for telehealth to enter into widespread use, its benefits must be proven in monetary terms. The question about who should bear the costs of a telehealth service was largely unresolved. A study conducted in Japan 31 addressed the question as follows: if the effects give rise to individual benefits, then the individual users should be willing to pay. On the other hand, if telehealth affects society more generally, then society should bear the cost. 57–61
Change management
Seven of the studies discussed the change management required for successful telehealth implementation. Changing the mindset of the people involved was found to be essential. The success of a telehealth programme depended not only on good technology but on effective management of human and organizational change. 31,61–66
Policy issues
The review found that only 4% of the 109 studies mentioned policy matters related to telehealth in particular and e-health in general. 42,57,63,66 Telehealth is a relatively new field for many Asian countries and policy development was found to be slow. However, there were countries like China, Indonesia, Malaysia, Singapore, South Korea, Taiwan and Thailand where national policies were designed to include telehealth as a component of larger development objectives. 63 The impact of these policies has not yet been evaluated, as they require time for implementation, with regular revisions and refinement. The literature suggested considerable thinking at the national and global level on making telehealth policies that would be incorporated into a country's e-government strategy. It was also concluded by some studies that the legal aspects (i.e. reimbursement, malpractice and privacy) of any telehealth project will depend on clarifying the logical steps involved in remote diagnosis or consultations. 63–66
Barriers to the implementation of telehealth
The barriers to the implementation of telehealth were:
19,33,44,45,48,53,54,57,67
Software incompatibility between two or more countries or institutions; Internet congestion causing delays or a low frame-rate of the video pictures and interruptions and delays in voice transmission; High communication charges and equipment costs; Other communication problems like a change of IP address and configuration of the receiving network, a broken cable at the host network and alteration of the cabling at the host site without authorization; Untrained service providers including physicians and staff; Small sample size and lack of follow up; Poor infrastructure and other logistical challenges.
Discussion
The results of the ten-year systematic review of the literature on telehealth in an Asian context indicate that the number of peer-reviewed publications about telehealth is rising. Most of the 109 studies were conducted in Japan. The review also showed that real time telehealth modalities were preferred by better developed countries like Japan, South Korea and Israel (39 real time studies). Our results showed that many studies were hospital-based (45%), with teleradiology, (involving images from neurology, orthopaedics and dermatology) being at the top of the list among medical specialties (12%), followed by home telehealth (12%). Nearly all of the home telehealth studies took place in Japan (12%).
The most commonly-used telehealth modality was store and forward (42%), suggesting the preference of developing countries for technologies which are low-cost, easy to use and require little bandwidth. Most of the developing countries preferred conventional telephone and ISDN lines for connectivity. Satellite connections were only used in remote and rural areas where the communication infrastructure was not well-developed, because of the high cost associated with such connections. None of the studies included in the review used any broadband or wireless connection. This might be because of the cost of equipment, or because of lack of awareness.
The methodological quality of most studies was poor, when judged according to the inclusion criteria. Most of the studies (57%) were descriptive in nature, not specifying any particular study design. This emphasizes the need for research-based studies with sound methodologies to generate reliable evidence for policy makers.
To appreciate the outcomes of any telehealth service, time is required for conceptualizing, planning and assessing the needs of the telehealth intervention on small or large scale, along with appropriate emphasis on change management. In contrast, most telehealth projects have not focused on measuring health-related outcomes, which should be the main and ultimate aim of any health project. Telehealth projects need to measure long-term, health-related outcomes, i.e. morbidity and mortality.
The results also showed that telehealth programmes cannot work in isolation. There needs to be a concentrated effort from professionals, departments, institutions and governments. Sustainability of an e-health or telehealth project will result only if a structure is in place from the start of the project, which integrates all the telehealth processes into the existing health-care system. If not, telehealth will remain alien to the system of health-care provision, jeopardizing its benefits and longevity.
Limitations
The present study had certain limitations. For example, no ‘grey literature’ or articles in non-English languages were included. Moreover, studies were included only from the last ten years of published peer reviewed work. A meta-analysis could not be performed due to a lack of homogeneity among the studies, which had different study settings, varying sample sizes and forms of samples used. The generalizability of the studies was also low.
Conclusion
The overall findings of the present review provide a generally optimistic picture of telehealth in Asian health care settings. Studies on telehealth applications have been useful, but there is a lack of good quality studies and in some cases the generalizability is limited to specific settings. Store and forward modalities have been used by developing parts of the Asian continent, while both real-time and store and forward modalities have been employed in the more developed countries. ISDN and conventional telephone lines, with a few satellite connections for remote areas, were preferred in the poorer countries, while broadband connections, wireless technologies and ISDN were used in the richer ones. The literature demonstrates the value of telehealth applications to decision makers, in developing countries generally and Asian countries in particular.
Footnotes
Acknowledgements
We thank the International Development and Research Centre, Canada (PANACeA Project) and the University Research Council of the Aga Khan University, Karachi for funding the review. We are also grateful to Gregory Pappas, Sajid Ali, Zainab Hussain and Musa Khan for their assistance.