
Abstract
We examined the agreement between diagnoses of pigmented skin lesions based on an in-person (face-to-face) dermatological examination and diagnoses based on the study of medical records and images transferred through the web (teledermatoscopy). Two experienced dermatologists examined and diagnosed 64 pigmented skin lesions, which had been surgically excised and undergone histopathology examination. Two years later, the same cases were studied and diagnosed once again by the same dermatologists via the web. There was 72% agreement between the in-person diagnoses and the biopsy results (the gold standard), and 66% agreement between the telediagnoses and the biopsy results. Telemedicine had high sensitivity (87%) and specificity (73%), although there were 4 false-negative diagnoses. A web-based dermatoscopic diagnostic service appears to be feasible and would meet the needs for access to specialized services in rural areas. However, further work is required to decrease the number of false negative cases.
Introduction
Dermatoscopy (epiluminescent microscopy or surface microscopy) is a non-invasive examination in vivo, frequently used to examine pigmented skin tumours. 1 The dermoscope has a magnifying lens which, aided by immersion-oil, allows improved visualization of skin structures. The immersion oil in contact with the skin reduces light reflection and makes the corneal layer of the skin more translucent. 2 In this way melanocytic lesions can be distinguished from non-melanocytic ones and can increase the diagnostic accuracy in cases of skin melanoma. 3 Dermatoscopy performed by an experienced dermatologist increases the diagnostic accuracy by 30% in cases of pigmented lesions. 4
In teledermatoscopy, dermatoscopic images are transmitted in order to obtain a diagnosis in pigmented skin lesions. Studies have been carried out to determine whether teledermatoscopy diagnoses are similar in accuracy to those obtained from clinical and dermatoscopic in-person examination. Piccolo et al. reported 91% agreement between in-person diagnoses from Italian dermatologists who examined 66 cases of pigmented skin tumours and those from Austrian dermatologists who analyzed the clinical and dermatoscopic images of the same lesions via the web. Furthermore, 86% of the image-based diagnoses agreed with the results of tumour biopsies. However, there have been few studies of the agreement between teledermatoscopic diagnoses. 5–8 The majority of published studies have evaluated the diagnostic concordance between in-person examination and teledermatoscopy of melanoma and atypical melanocytic lesions. Furthermore, in most studies, the examining team that performed the in-person diagnoses was different from the team who analyzed the images via the web. The present study involves face-to-face diagnostic analysis as well as web images of both benign and malignant pigmented skin lesions performed by the same team of participants.
The main aim of the present study was to determine the agreement between the diagnosis made by a specialist carrying out the clinical and dermatoscopic examination of pigmented skin lesions in person and the diagnosis made by studying the patient's data and images accessed through the web (teledermatoscopy).
Methods
The study was approved by the appropriate ethics committee.
Cases
The study was conducted on 64 cases. Two dermatologists, each with more than 15 years of experience in dermatoscopy, initially examined 300 cases of pigmented skin lesions in patients referred to the clinic of the Department of Dermatology of the Federal University of São Paulo School of Medicine (UNIFESP-EPM) in 2005. All these cases were photographed. The clinical photographs were taken with a digital camera (Nikon Coolpix 4300) and the dermatoscopic photographs were obtained with the same digital camera (image resolution of 2272 × 1704 pixels) attached to a dermatoscope (Heine Delta 20).
From the 300 cases, 80 cases were submitted to histopathology examination. The histopathology diagnosis (gold standard) was performed by a pathologist with more than 15 years of experience in dermatopathology.
An independent examiner, also a dermatologist with more than 15 years of experience in dermatoscopy, selected 64 cases from the 80 cases submitted to histopathology examination. The criteria used to select the 64 cases were the availability of clinical and dermatoscopic images of the same lesion, as well as its biopsy records. The cases were also selected according to biopsy samples so as to have a set including the main dermatoscopic diagnosis – melanocytic naevus, atypical naevus, blue naevus, melanoma, seborrheic keratosis, pigmented basal cell carcinoma and Reed's naevus – and occurrences in all anatomical locations. The patients (61% female and 39% male) were aged 5 to 86 years old.
Phase 1
Two dermatologists examined the clinical photographs independently, and made a single diagnosis. When they disagreed, they discussed it with each other and reached a consensus.
The medical records of the 64 cases, as well as the respective level of difficulty in reaching a diagnosis ranked by the independent investigator (difficult, intermediate or easy) were entered into a database.
Phase 2
The second phase of the study took place 24 months after the first. A web system was set up (Figure 1) so that the medical records of the 64 cases, with images in JPEG format, could be presented for store-and-forward diagnosis. The same two dermatologists who had previously participated in phase 1 took part in phase 2.
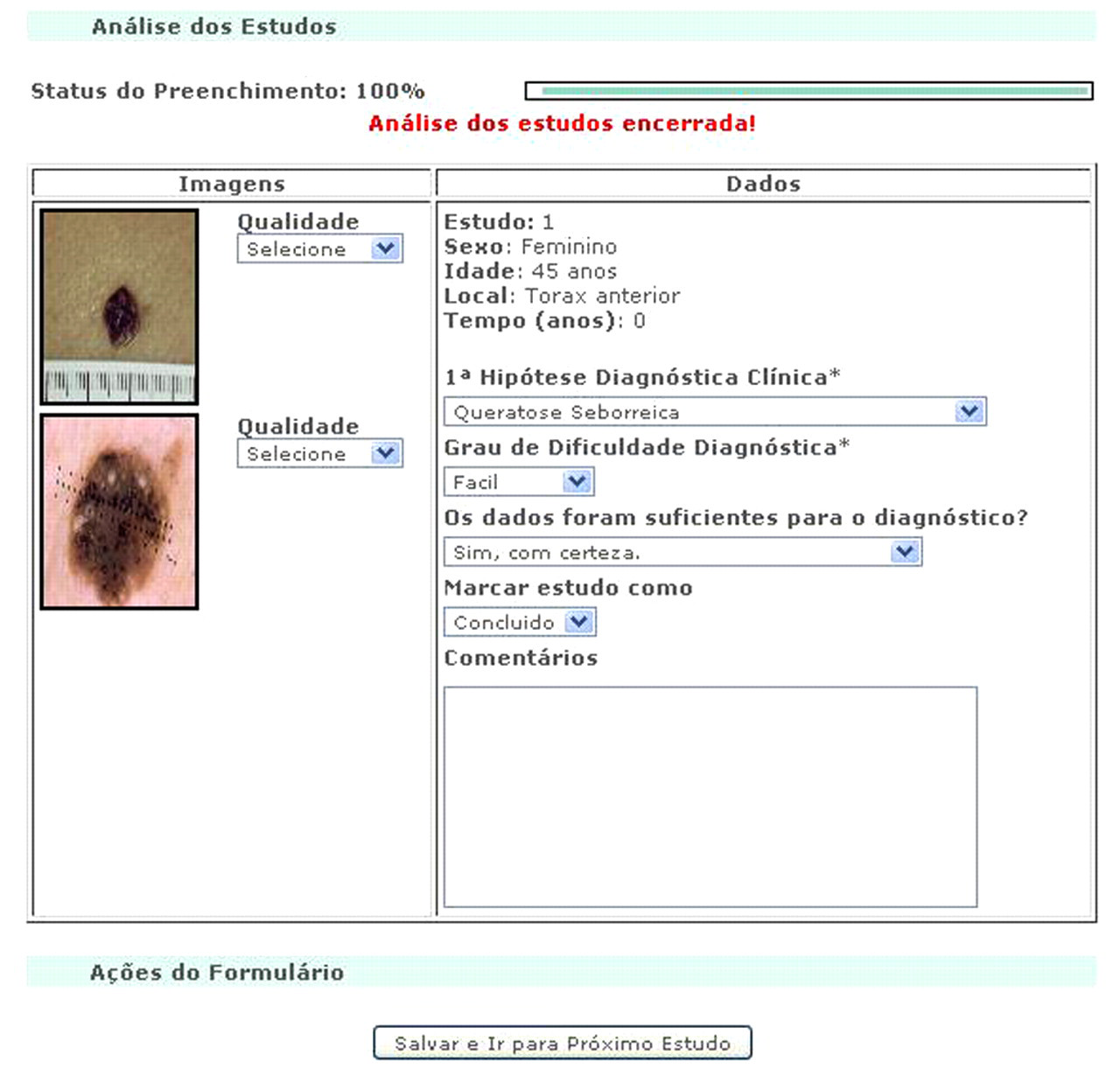
Web system for telediagnosis
A set of clinical data (age, gender, anatomical location and length of time the lesion had been present) and images (clinical and dermatoscopic ones of each lesion – a minimum of two and maximum of six and image resolutions ranging from 640 × 480 to 2272 × 1704 pixels) were assessed by the dermatologists.
The dermatologists had only blind access to the cases, which could be done randomly. Their previous diagnoses, level of difficulty ranked by the independent observer and biopsy results were not visible to these specialists, who, in addition to entering their diagnosis for each case, were asked to rank the difficulty of their task and the quality of the images, as well as state whether additional data would help to reach or improve a diagnosis. The dermatologists examined each case and provided a single diagnosis.
Besides the diagnosis, they rated the diagnosis according to its level of difficulty, quality of the image available through the web and whether the data were sufficient for definite diagnosis.
Statistical analysis
Agreement between in-person diagnosis and biopsy results and between the teledermatoscopy and biopsy results were measured using the kappa statistic. 9 The sensitivity and specificity of in-person diagnosis and teledermatoscopy were determined using the biopsy results as the gold standard.
Results
The percentage of diagnoses made in-person, by teledermatoscopy, and according to the biopsy results are shown in Figure 2. Basal cell carcinoma and melanocytic naevus were the most frequent telediagnosis and biopsy results.
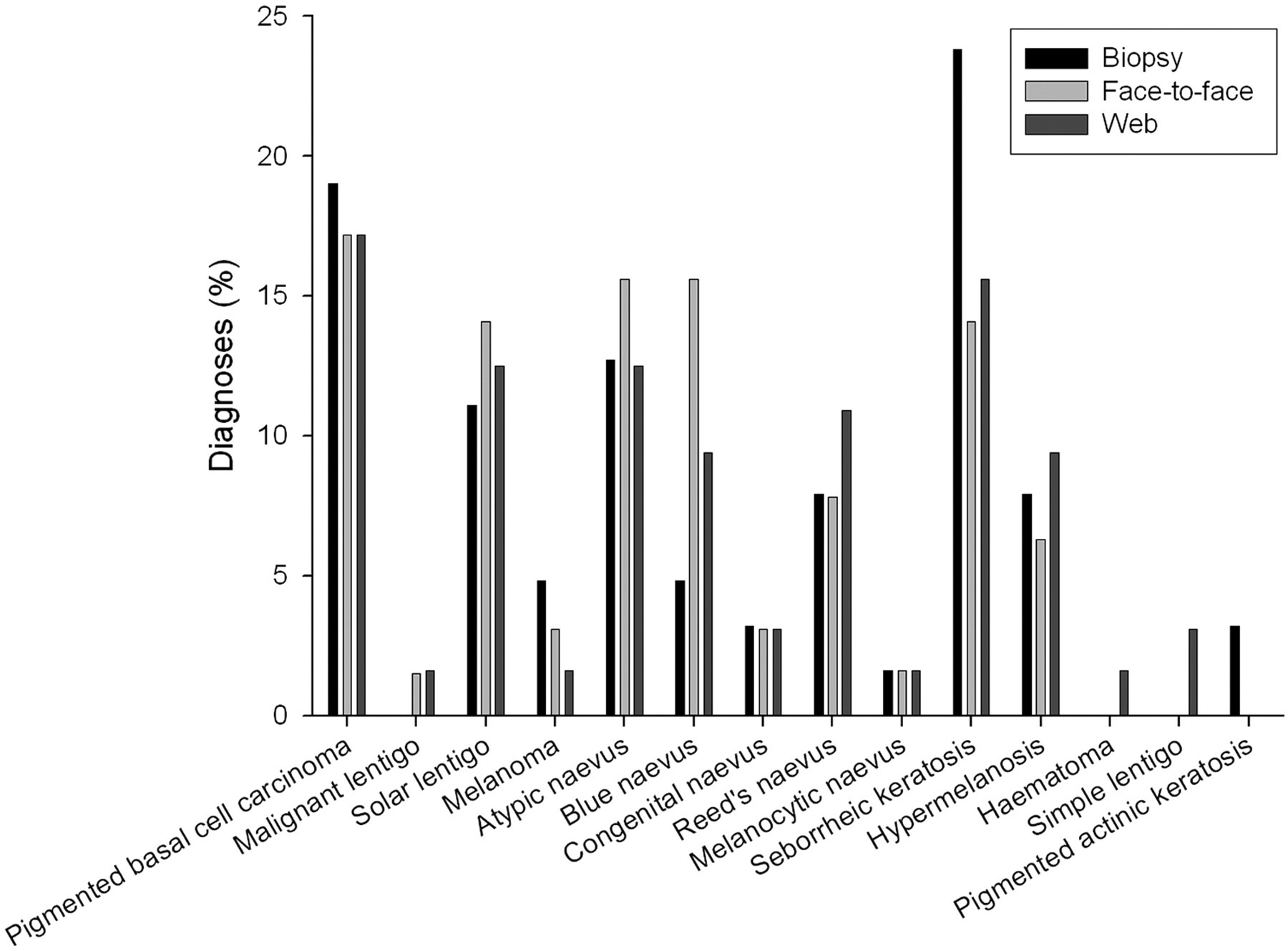
Percentage of diagnoses made face-to-face, by web and by biopsy (n = 64)
Kappa statistics
The agreement levels were κ = 0.73 (95% CI, 0.61 to 0.85) when comparing in-person diagnosis and biopsy results, and κ = 0.66 (95% CI, 0.53 to 0.79) when comparing teledermatoscopy and biopsy results.
Sensitivity and specificity
The biopsy results determined 30 malignant and 33 benign lesions. The in-person diagnosis determined 40 malignant and 23 benign lesions. Teledermatoscopy determined 35 malignant and 28 benign lesions (Tables 1 and 2).
In-person diagnoses compared with the biopsy results (gold standard)
Teledermatoscopy diagnoses compared with the biopsy results (gold standard)
Compared with the gold standard (biopsy results), the in-person diagnoses included one false benign and 11 false malignant tumours, whereas teledermatoscopy included 4 false benign and 9 false malignant skin changes. In accordance with the level of diagnostic difficulty two false positive cases were classified as difficult via the web and the remaining two as easy and intermediate.
Both in-person diagnosis and teledermatoscopy determined a malignant atypical naevus as a Reed's naevus. The other three false benign teledermatoscopy diagnoses were a malignant lentigo on the scalp, a melanoma on the posterior aspect of the trunk and a plantar malignant atypical naevus, and were determined as seborrhoeic keratosis, congenital naevus and melanocytic naevus, respectively (Figure 3).
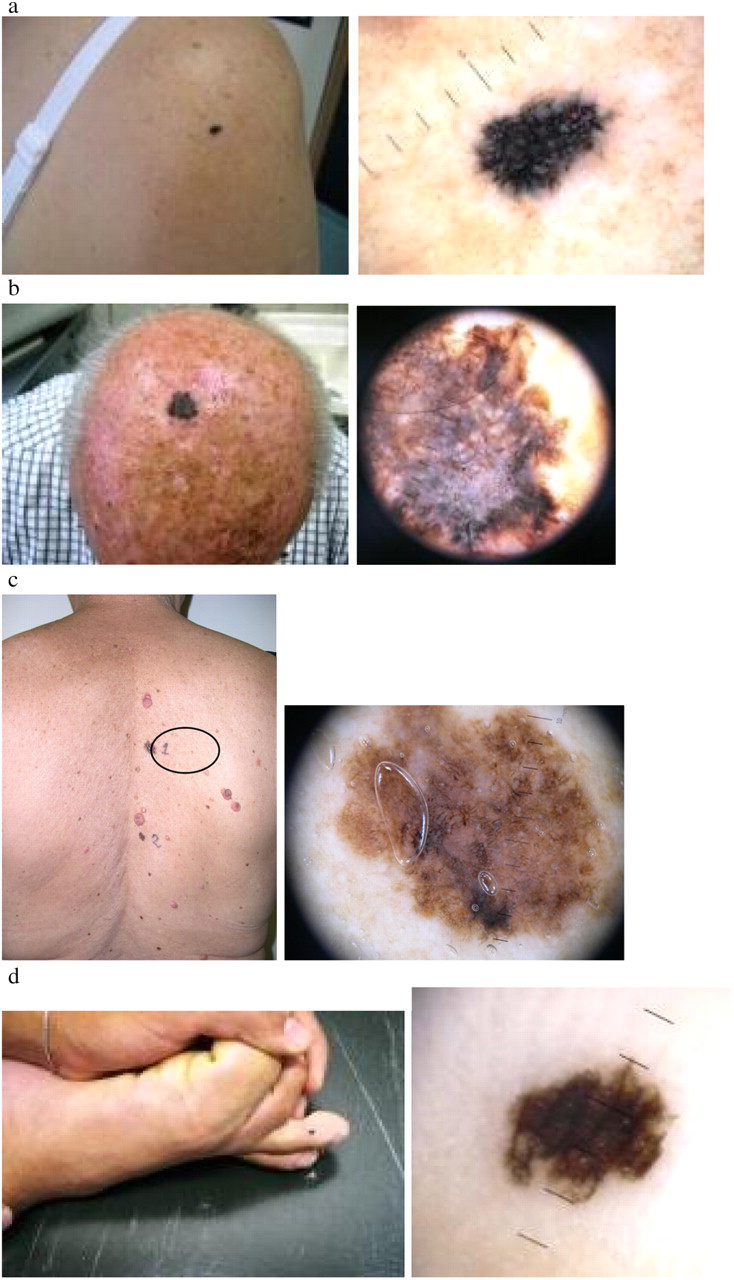
Web false negative cases: (a) atypical naevus on the right shoulder, diagnosed as Reed's naevus on both patient examination and web assessment; (b) malignant lentigo on the scalp, web-diagnosed as seborrheic keratosis; (c) melanoma on the posterior aspect of the trunk, web-diagnosed as congenital naevus; (d) plantar atypical naevus, web-diagnosed as melanocytic naevus
The sensitivity and specificity for in-person diagnosis were 96.7% and 66.7%, respectively. The sensitivity and specificity for teledermatoscopy were 86.7% and 72.7%, respectively. There were no significant differences between the corresponding rates (Table 3).
Statistical measures for in person examination and the web assessment of pigmented skin lesions (n = 63) when compared with the biopsy results (gold standard)
Task difficulty
Table 4 shows the percentage of cases rated difficult, intermediate and easy to diagnose ranked by both the independent observer and the diagnosing panel at the time of teledermatoscopy.
Levels of difficulty in reaching a diagnosis by in-person examination and by web assessment (n = 64)
Teledermatoscopy was more frequently rated as difficult in cases of atypical naevus. It was rated as intermediate in cases of basal cell carcinoma. Malignant lentigo and melanocytic naevus were rated as easy.
There was an excellent agreement (κ = 0.96) between teledermatoscopy and biopsy results in cases rated as easy (see Table 5). There was less good agreement in cases rated as intermediate or difficult (κ = 0.40 and κ = 0.38, respectively).
Agreement between teledermatoscopy and biopsy results according to diagnosis level
Only 5% of the images accessed through the Internet were considered to be of bad quality. These images were out of focus. The set of clinical records available on the web (gender, age, site of the skin lesion, length of time the lesion had been present) was considered to be satisfactory for diagnosis by both examiners.
Discussion
In the present study, the agreement between in-person diagnosis and teledermatoscopy was 73%. Similar rates were reported in previous studies, with higher rates when the diagnoses were made by more experienced dermatologists. 6–8,10,11 A multi-centre study including 11 professionals with different levels of dermatoscopy skill obtained an average score of 85% for correct diagnosis of 43 images of pigmented skin lesions sent via email. The less experienced participating dermatologists obtained lower scores, 77% on average. 11
As observed in the current investigation, higher scores for correct diagnosis were attained in sets of cases considered easier to diagnose. Piccolo and colleagues reported decreased teledermatoscopic accuracy for cases of increased difficulty.
In the present study, only 5% of the images accessed through the Internet were considered to be of bad quality, although they were converted into JPEG format for storage, and made available in varied sizes. These images were out of focus. In a study comparing paper photographs and reduced-size digital images, Provost et al. (1998) reported good agreement between the diagnoses from four observers concerning atypical naevus and incipient melanoma. 12 This indicates that a good diagnosis can be achieved even with small digital images (460 × 640 pixels) provided they are of good quality.
No significant differences between in-person diagnosis and teledermatoscopy for sensitivity and specificity were found in the present investigation. However, it is important to point out that, despite the only false negative in-person diagnosis – a malignant atypical naevus diagnosed as Reed's naevus – being reproduced in teledermatoscopy, three other false negative teledermatoscopy diagnoses were made. Carli et al. determined a sensitivity of 81% for diagnosis of melanoma based on photographs sent through slides, and a sensitivity of 98% based on the dermatoscopic examination of the lesions. The same study determined nine false negative cases in assessing slide photographs and only one false negative case based on dermatoscopic examination, thus providing evidence that patient examination is a more reliable assessment of melanocytic lesions. 13
Moreover, the three-dimensional aspect of dermatological lesions, for instance, seen under the dermascope, is not reproduced in digital images sent through the worldwide web. This seems to reflect a lower level of diagnostic accuracy. When comparing the diagnoses based on digital imaging with the diagnoses from a specialist who performed the physical and dermatoscopic examination of the patient, their agreement in cases of papulosquamous, infectious, pre-malignant or malignant, and pigmented skin lesions was nearly 100%. However, it fell to 22–46% for skin changes involving papules. 14
In the previous studies, the observers performing in-person diagnoses were not the same ones doing the teledermatology. In the present study, however, the participating dermatologists who performed the in-person diagnoses also did the teledermatoscopy of the same cases. Furthermore, both specialists examined all cases optically and digitally in (combined) panel fashion. This was intended to avoid bias due to differences regarding individual skill and knowledge on the part of the observers involved. The authors are aware that the panel work may have led to higher levels of diagnostic accuracy as compared with independent observation. Bias associated with memory was unlikely as 24 months had elapsed between optical and digital observations.
The set of clinical records made available on the web in this study (gender, age, site of the skin lesion, length of time the lesion had been present, with an average of 2.6 images per case) was considered to be satisfactory for dermatological diagnosis, although the accuracy of the teledermatoscopy offered in this study was found to be inversely associated with the complexity of the skin lesion aspect.
Conclusion
In the present study we found that it was possible to obtain a high rate of diagnostic accuracy of pigmented skin lesions by teledermatoscopy. Digital imaging is a low-cost technique, which contributes to the follow-up of various pathologies. Telemedicine can provide access to specialized medical services in areas which lack them. Web consultation on pigmented skin lesions can improve diagnostic accuracy and the quality of medical care delivered in a private clinic.
Teledermatoscopy is an effective, reliable and low-cost diagnostic aid. However, further studies concerning the telediagnosis of false benign pigmented skin lesions should be carried out. Although the participating dermatologists were familiar with digital image exchange for second opinion purposes, this was the first time they had conducted a teledermatoscopy study. Teledermatoscopy of malignant or benign pigmented skin lesions offers good diagnostic accuracy when compared with face-to-face diagnosis and histopathological diagnosis and should be used by dermatologists with a high level of experience in dermatoscopy. Both dermatological clinical examination and dermatoscopy performed in person offer higher diagnostic accuracy and should not be substituted for telediagnosis. Nevertheless, teledermatoscopy is extremely useful in areas where there is no specialist available or to obtain a second opinion. Teleconsultation of clinical and dermatoscopic images via the web represents a valuable tool for the diagnosis of pigmented skin lesions when expert counselling is not available for face-to-face diagnosis.