
Abstract
The U Special Kids Program (USK) at the University of Minnesota provides care coordination and case management services by telephone to children with special health-care needs. We measured the effect of the USK programme on hospital resource utilization using a retrospective record review. Information on hospitalizations was collected for children enrolled in the programme for at least two years and validated for accuracy against inpatient claims data. Hospitalizations were classified as planned, unplanned or due to lack of home care. A total of 43 children enrolled in the USK programme between July 1996 and December 2006 met the study criteria. The children had multiple, complex conditions. During the period of the study, there were 61 planned hospitalizations, 184 unplanned hospitalizations and 3 hospitalizations due to lack of home care. The number of unplanned hospitalizations decreased from 74 in the first year of enrolment to 35 in the second; this reduction was significant (P < 0.007). In the subsequent years, the rate of unplanned admissions stabilized. In contrast, the rate of planned hospitalizations was relatively constant over the five-year enrolment period. Telephone-based care coordination and case management is a promising approach for children with multiple, complex health conditions.
Introduction
Children with special health-care needs (CSHCN) represent a large (11 million) and diverse group, 1 encompassing children at risk of developing a chronic condition as well as children with multiple and complex health and social service needs. The latter group, who are referred to as CSHCN of high intensity, 2 are expensive to manage because the hospitalizations, equipment, home nursing and medication-related services all lead to high costs. 1,3
The Institute of Medicine has stressed that a central focus for improving the quality of health-care delivery should be the provision of care coordination services, especially for people with chronic illnesses. 4 Research on the efficacy of comprehensive care for CSHCN has shown a reduction in health-care costs, an increase in family satisfaction and an improvement in clinical outcomes. 5–8 These results led the American Academy of Pediatrics (AAP) to conclude that coordinated care is an essential component of health care for CSHCN and should be provided by the child's ‘medical home’. 9
Medical home models
Recently, two enhanced versions of the medical home model have been described in the literature. The Special Needs Program at the Children's Hospital of Wisconsin uses a tertiary care–primary care partnership model to ensure seamless inpatient and outpatient care for complex and medically fragile children. 10 The U Special Kids Program (USK) at the University of Minnesota focuses on planning, managing and coordinating the medical, nursing, educational, social and home health service providers that are necessary to meet the complex care needs of CSHCN. 2 Both programmes work in partnership with primary care providers, specialists and the child's family to develop a comprehensive and coordinated plan of care.
USK programme
The USK programme is based on Wagner's chronic care model. 11 A team of two advanced practice nurses provides telephone-based, comprehensive care coordination and case management to CSHCN in the state of Minnesota. Enrolment in the programme is limited to children with moderate to high intensity health needs based on the following criteria: (1) four or more significant chronic medical problems; (2) multiple medical specialists; (3) numerous medications or rare pharmaceuticals; (4) repeated hospitalizations and/or emergency room visits; (5) dependence on technology, i.e. feeding tube, tracheotomy, central line or oxygen; and (6) needs not being met by another service such as cystic fibrosis or bone marrow transplant programmes. At the time of the present study, 50 children were enrolled in the programme.
The USK programme does not replace a child's primary care provider. Rather, it coordinates the communication between the family, tertiary care services, social services, the child's primary care site and other local providers, specialists, the school system and health insurers. Parents are encouraged to contact the service whenever they have a question about their child's health and all interactions are documented in an electronic health record. When possible, acute, minor illnesses are addressed by telephone; when this is not possible, coordination of emergency services by local and if necessary, tertiary providers, is conducted by the USK team via telephone, fax and the electronic health record.
Outcomes
The effect of the Wisconsin Special Needs Program on tertiary care centre utilization was measured using a pre-enrolment/post-enrolment study. There was a significant decrease in tertiary hospitalizations after enrolment in the programme. 10
We have measured the effect of the USK programme on hospital resource utilization using a retrospective record review. The primary hypothesis was that children would experience a decrease in unplanned/emergency hospitalizations after enrolment in the USK programme.
Methods
The study was approved by the appropriate ethics committee and all data collected were de-identified to maintain confidentiality. The baseline was established retrospectively from hospitalizations of children enrolled in the USK programme for at least two years. Of the 50 enrolled children, 43 met this criterion. Data were extracted from each child's Summary of Critical Information. This document is created on enrolment after the nurses conduct a comprehensive review of the child's medical record. The information is verified with the parents/guardians. The Summary is maintained by the USK team and serves as a resource for diagnoses, active problems, pertinent health history including hospitalizations, medications, immunizations and allergies, and social and educational needs.
The accuracy of the hospitalization data collected from the Summary of Critical Information was checked prior to analysis. As the majority of hospitalizations (70%) occurred at the affiliated academic health centre, inpatient claims data for 40 subjects enrolled between July 1996 and December 2004 were requested. Manual validation between the paper claims data and the admission and discharge dates extracted from each child's Summary of Critical Information was conducted as part of another study. The validation process revealed that 208 inpatient claims were generated for the 40 children enrolled in the USK programme, and 100% of these claims had a correct corresponding entry in the Summary of Critical Information. Thus the data extracted from the Summary of Critical Information was deemed accurate.
The remaining 30% of the hospitalizations occurred outside the affiliated academic health centre. Reviewing the claims data for these hospitalizations, which occurred throughout the country, was not feasible and they were assumed to be accurate.
Data pre-processing
Children enrolled in the USK programme at different times, so the classification of when a hospitalization occurred required standardization. For each hospitalization, the number of months between enrolment in the USK programme and the hospitalization admission date was calculated and the result was divided by three to calculate a new attribute, ‘quarter since enrolment’, for the hospitalization (one quarter = three months).
Each hospitalization was classified as planned, unplanned or due to a lack of home care:
A planned hospitalization was scheduled in advance because of an anticipated need arising from the child's chronic conditions; An unplanned hospitalization was due to an unanticipated change in the child's health. This was due to acute illnesses and injuries (e.g. ear infection, pharyngitis, gastroenteritis, orthopaedic injuries) or to complications resulting from the child's underlying chronic conditions (e.g. mechanical device failure, kidney failure, blood disorder, seizure disorder); A hospitalization due to a lack of home care was in response to insufficient social resources to care for the child at home.
The classification was performed by the USK physician using a ‘think-aloud’ protocol. This methodology is based on the information-processing approach of protocol analysis,
12
and requires a participant to verbalize what they are thinking while performing a task, making the cognitive processes more transparent. In the present study, the think-aloud protocol was used to avoid bias during hospitalization classification: the physician was asked to explain the reasoning for classification if the free text reason for the hospitalization did not make the classification explicit.
Analysis
The hospitalization data was normalized by calculating the number of hospitalizations per quarter/number of subjects per quarter. Comparisons between year one and year two were analyzed by a paired t-test. A descriptive analysis was conducted using a spreadsheet (Excel 2003) and a statistical analysis was conducted using a standard statistical package (Intercooled Stata, Version 9).
Results
The analysis was based on 43 children enrolled in the USK programme between July 1996 and December 2006, and the hospitalizations that occurred during the first five years of each child's enrolment. The children had multiple, complex conditions that were categorized by their major diagnosis (see Table 1).
Characteristics of the subjects
During the period of the study, there were 61 planned hospitalizations, 184 unplanned hospitalizations and 3 hospitalizations due to lack of home care (see Table 2). The normalized rates of planned inpatient days were approximately constant during the five years, while the normalized rates of unplanned inpatient days declined during the study period (see Figure 1).
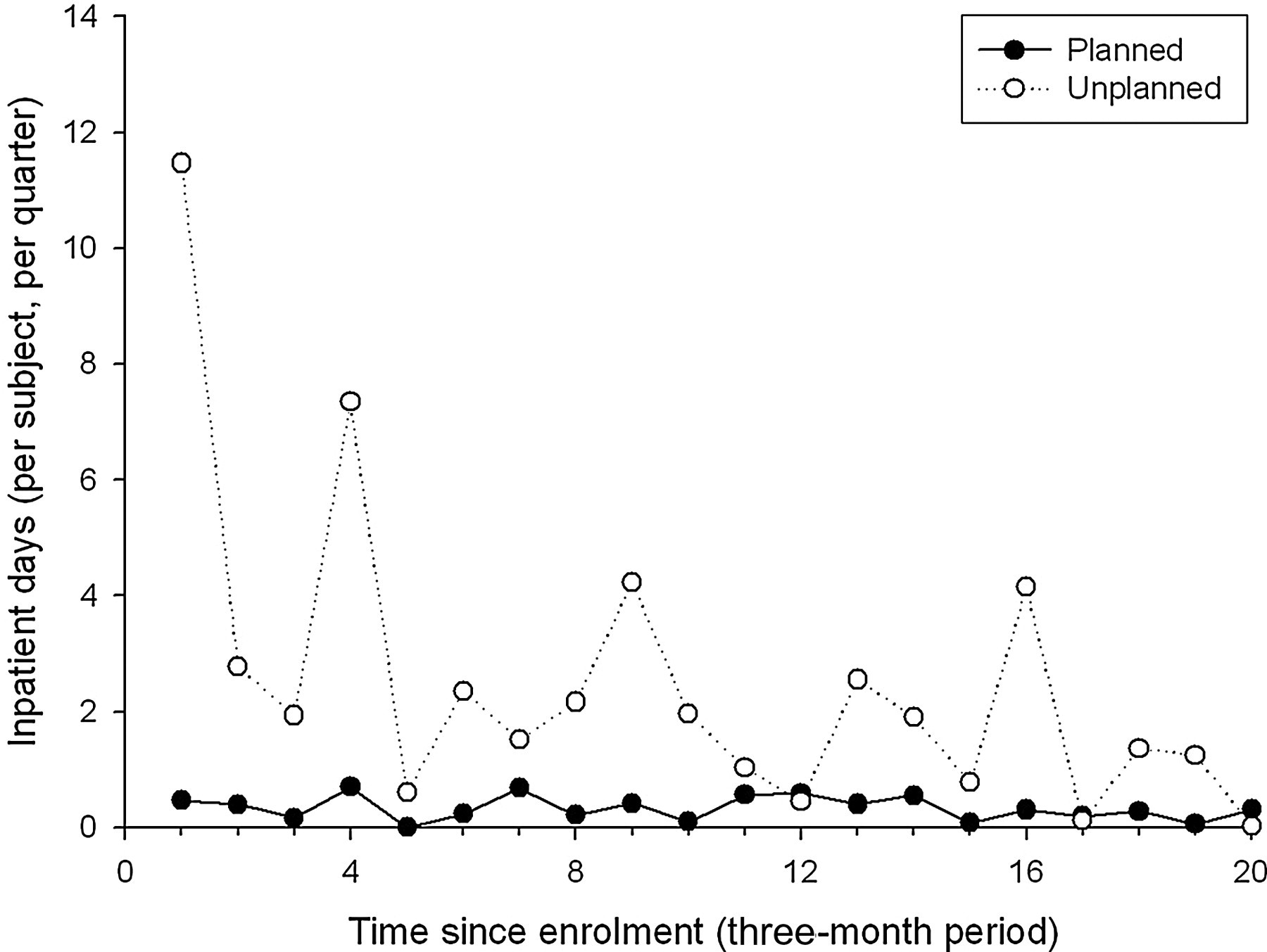
Planned and unplanned hospitalizations over five years (quarters 1–4 represent the first year of enrolment in the programme, quarters 5–8 the second year of enrolment, etc). Three hospitalizations due to a lack of home care are not included in the graph. The numbers of subjects for each quarter varied slightly
Hospitalization data for all 43 subjects over the first five years of enrolment
*Planned hospitalizations included admissions for device placement (e.g. tracheotomy, pacemaker), diagnostic procedures, surgical procedures (e.g. heel-cord lengthening, cleft palate repair), feeding problems (e.g. oesophageal dilatation), dental extraction
†Unplanned hospitalizations included admissions for fever or pain of unknown origin, viral or bacterial infection, equipment malfunction (e.g. ruptured gastro-jejunal balloon), allergic reaction, seizures, hypoglycaemia, gastro-oesophageal reflux disorder, major emergency surgery, respiratory distress, mental health crisis (e.g. suicide attempt, depression)
‡Hospitalizations due to lack of home care included admissions for family respite, fire/smoke damage in apartment, no home care staff available
During the period of enrolment used for the study, which ranged from two to five years, nine children (21%) had no hospitalizations, six children (14%) had only one hospitalization and the remaining 28 children (65%) had two or more hospitalizations. Of the nine children with no hospitalizations, four left the programme as they did not require the service.
The number of unplanned admissions and unplanned inpatient days was significantly lower in the second year of enrolment than in the first year (see Table 3). For planned hospitalizations, there was no change in admissions or inpatient days between years one and two.
Planned and unplanned hospitalizations in years 1 and 2
*Paired t-test
Discussion
In the present study, we used hospitalization frequency to test the primary hypothesis: that unplanned hospitalizations would decrease as the length of time enrolled in the USK programme increased. The results showed that during the second year of enrolment, the number of unplanned admissions and inpatient days dropped significantly. There was a relatively constant rate of planned hospitalizations over the five-year period. These results are similar to those from the Maryland Rare and Expensive Case Management Program, which is designed for vulnerable children with rare, chronic and expensive conditions. An evaluation of this programme found that case management had a significant effect on lowering costs, particularly inpatient costs, despite an increase in outpatient costs. 13
Although hospitalizations due to a lack of home care (1% of total) were not included in the present analysis, their implications warrant discussion. These hospitalizations are the result of social service needs (i.e. child neglect, lack of housing, lack of home care help), not health needs. Care coordination and case management that focuses on traditional health-care interventions will not prevent this type of hospitalization. Incorporating a social services framework into the care coordination and case management model could eliminate these unnecessary hospitalizations.
A limitation of the present study is the lack of a cost analysis. During the review of inpatient claims to validate the accuracy of hospitalization data on the Summary of Critical Information, the hospital charge information was collected. However, an analysis was not conducted for several reasons. First, claims were obtained only from the affiliated tertiary hospital, and these claims represented approximately 70% of the hospitalizations. Second, the hospitalizations occurred over a 13-year time span, from 1996 to 2008, and would require adjustment for inflation. Last, the amount charged for a hospitalization is rarely the amount reimbursed; often the reimbursement is much smaller.
A primary focus of the USK programme is working with a child's parent or guardian to develop a comprehensive plan of care. It can be hypothesized that adhering to this plan of care increases a parent's ability to care for their child and reduces the number of emergencies. The use of telephone contact provides parents with easy access to the USK programme. This helps parents and nurses to detect the subtle changes that foreshadow a child's illness.
The retrospective and non-random nature of the present study raises the question: was the reduction in unplanned hospitalizations the result of regression to the mean? This phenomenon occurs ‘in situations of repeated measurements when extreme values are followed by measurements in the same subjects that are closer to the mean of the basic population.’ 14 The children enrolled in the USK programme do not represent the general population. Instead, they represent financial outliers – they have life-long conditions, are technology-dependent and are heavy users of health-care resources. It can be argued that the fall in unplanned hospitalizations was not the result of regression to the mean because both unplanned admissions and inpatient days stabilized after the second year of enrolment in the programme (Figure 1).
We conclude that telephone-based care coordination and case management is a promising approach for children with multiple, complex health conditions. The low cost and universal availability of the telephone are distinct advantages of the telehealth utilized by the USK programme. Despite the intensive nature of the care provided, unplanned hospitalizations will still occur. It can be hypothesized that minimizing unplanned admissions will reduce family stress, improve the child's wellbeing and reduce the utilization of health-care services. Evaluating programmes like the USK in randomized studies is needed to measure their efficacy in terms of the child's health, and both inpatient and outpatient utilization.
Footnotes
Acknowledgments
We thank Nancy Hoogenhous and Laurie Snively for their help with data extraction and explanations regarding the USK programme.