
Abstract
Expert visual guidance (EVG) is computer assistance that displays to the examiner how the image plane moves towards (or away from) a desired anatomical location as the ultrasound probe is manipulated over the patient's body. We tested whether EVG by a remote expert could assist inexperienced examiners in acquiring abdominal ultrasound images. The inexperienced examiners were 20 medical students, who were randomly assigned to verbal instruction alone (Group 1) or to EVG (Group 2). The examiners were tested on their ability to visualize the abdominal aorta and the right kidney. Group 2 was more successful in identifying specified anatomy in longitudinal and cross-sectional views of the aorta (95 vs. 75%, P = 0.032) and kidney (98 vs. 88%, P = 0.09). The groups succeeded equally well in obtaining a true cross-sectional view of the aorta. Kidney length was also similar when measured by the two groups. The results demonstrate that an inexperienced ultrasonographer can be significantly assisted by EVG compared to verbal instruction alone. This could be useful for tele-mentoring in rural hospitals as well as for teaching, both in person and at a remote site.
Introduction
Providing rural health care has always been difficult due to the scarcity of local medical resources and the distances between patients, physicians and health-care facilities. In the case of ultrasound examination, the lack of trained examiners in isolated places with reduced medical facilities results in poor image quality, incomplete examinations and inaccurate diagnoses. 1–3 Ultrasonography is a difficult skill to learn and to maintain, because the only clue to the location and orientation of the image plane relative to organ is the appearance of the organ on the image. There is no positional feedback to show the examiner how far an image plane deviates from the true long axis or cross-section of a target organ. Consequently even experienced examiners commit errors in image plane positioning. 4
Expert visual guidance (EVG) is computer assistance that displays to the examiner how the image plane moves towards (or away from) a desired anatomical location as the ultrasound probe is manipulated over the patient's body. This anatomical information is provided in a real-time display that the examiner can monitor in addition to the ultrasound screen. The purpose of the present study was to test whether EVG by a remote expert can assist inexperienced examiners in acquiring abdominal ultrasound images. We hypothesized that EVG would produce adequate images more frequently than guidance by verbal instruction alone.
Methods
The protocol was approved by the appropriate ethics committees. All patients and volunteers gave informed consent.
Expert visual guidance system
The software for the EVG system was developed at the University of Washington and tested at the University of Vermont and Fletcher Allen Health Care, a major teaching hospital. We implemented four methods for EVG. The first method displays the current image plane's position as a line-of-intersection with one or more previously acquired ‘scout’ images (Figure 1). 5 The line-of-intersection display does not indicate whether the current image plane is tilted inappropriately in the out-of-plane dimension.
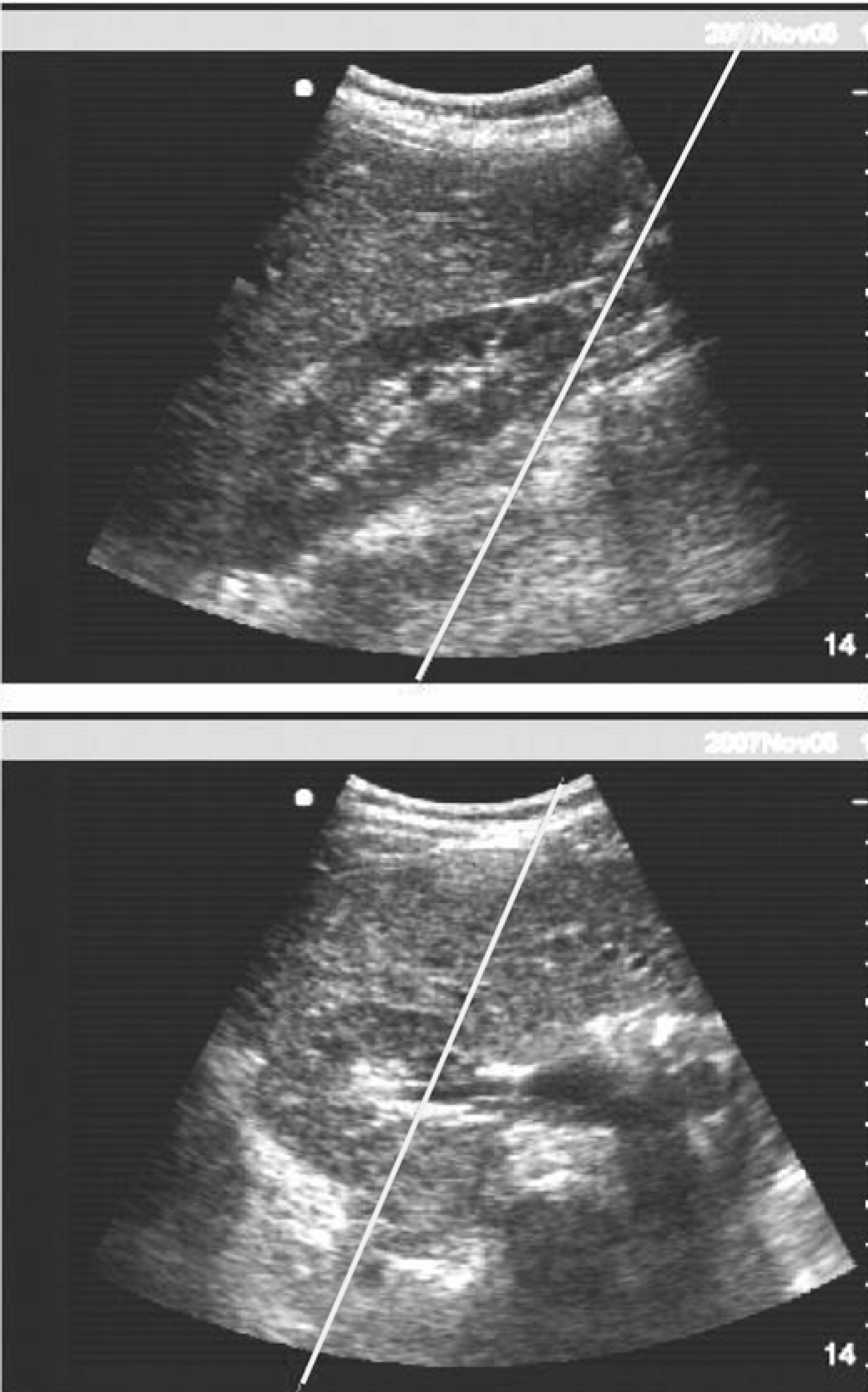
Right kidney. The line of intersection displays in real time the location of the current image plane where it intersects with previously acquired ‘scout’ images
The second method displays the current image as a translucent plane to show not only how it intersects with each scout image but also how it tilts relative to the plane of the scout image (Figure 2). This presentation helps the user to see the position and also the orientation of the current image relative to the target organ as revealed in the selected scout images. By reviewing the intersecting image planes directly, the user can appreciate quickly how well the target anatomy is being visualized. The angle between selected planes is displayed to assist the examiner in obtaining orthogonal views.
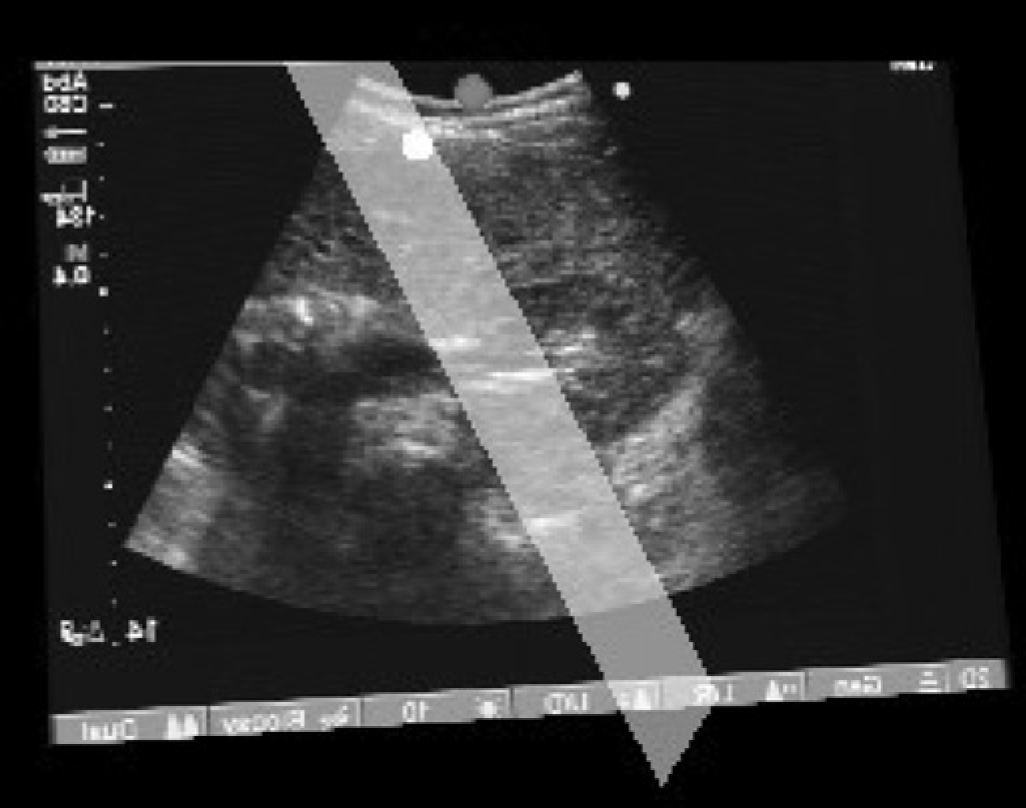
Visual guidance display of the current image as a translucent plane overlaid onto the scout image
The third method displays how the current image plane intersects a three-dimensional (3D) reconstruction of the target organ. This surface is generated after the examiner enters at least three landmark points from the images that have been acquired (Figure 3a–c). The 3D surface illustrates the anatomical position and orientation of the current image, so that the examiner understands when he/she is cutting a cross-section or a longitudinal view with the transducer. Thus the 3D surface acts as a map to assist the examiner in acquiring images that visualize specific anatomical features. Estimation of the 3D surface from sparse input data is facilitated by a database that embodies knowledge of the expected shape of the target organ. Briefly, a piecewise smooth subdivision surface is computed as a weighted sum of surfaces in the database. The weights are determined by shape similarity to the entered points using an optimization routine that minimizes the distance from the entered points to the surface. 6 Accuracy in 3D reconstruction requires an extensive database populated with studies spanning the range of human disease. For the present study, the 3D surfaces were used only as a visual guide, so that limited databases sufficed.
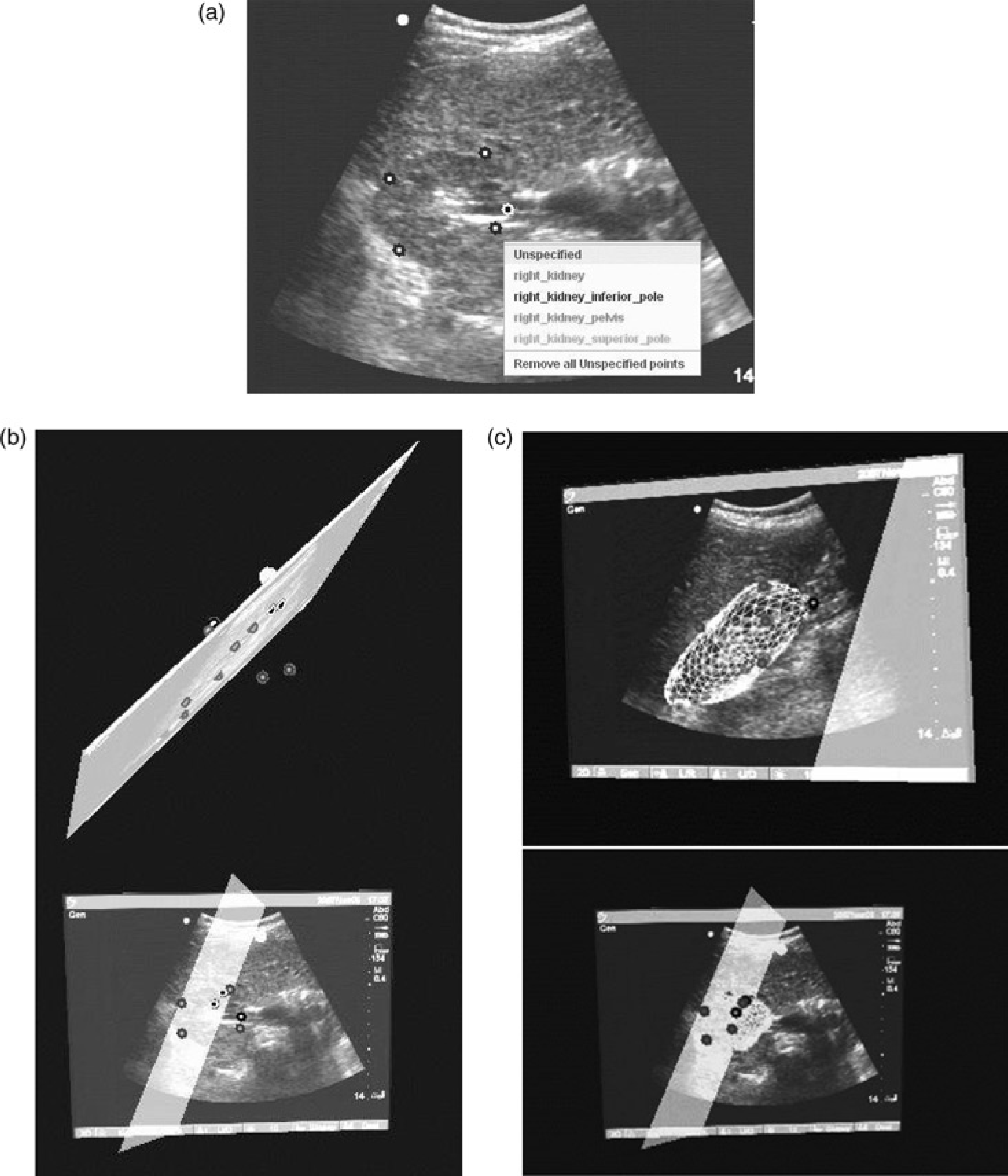
Rapid reconstruction of the right kidney from sparse points for guidance. (a) Cross-section of kidney with traced points. Each point's anatomical origin is labelled from a menu. (b) The spatial position of traced points is displayed relative to the scout images. (c) After reconstruction, the surface is displayed as a triangular mesh overlaid on the scout images
In the fourth mode of assistance, a remote expert positions a differently coloured plane on the computer screen to indicate the anatomical location of the desired image (Figure 4). To acquire that image, the examiner needs to manipulate the transducer to superimpose the current image plane on the plane of the desired view.
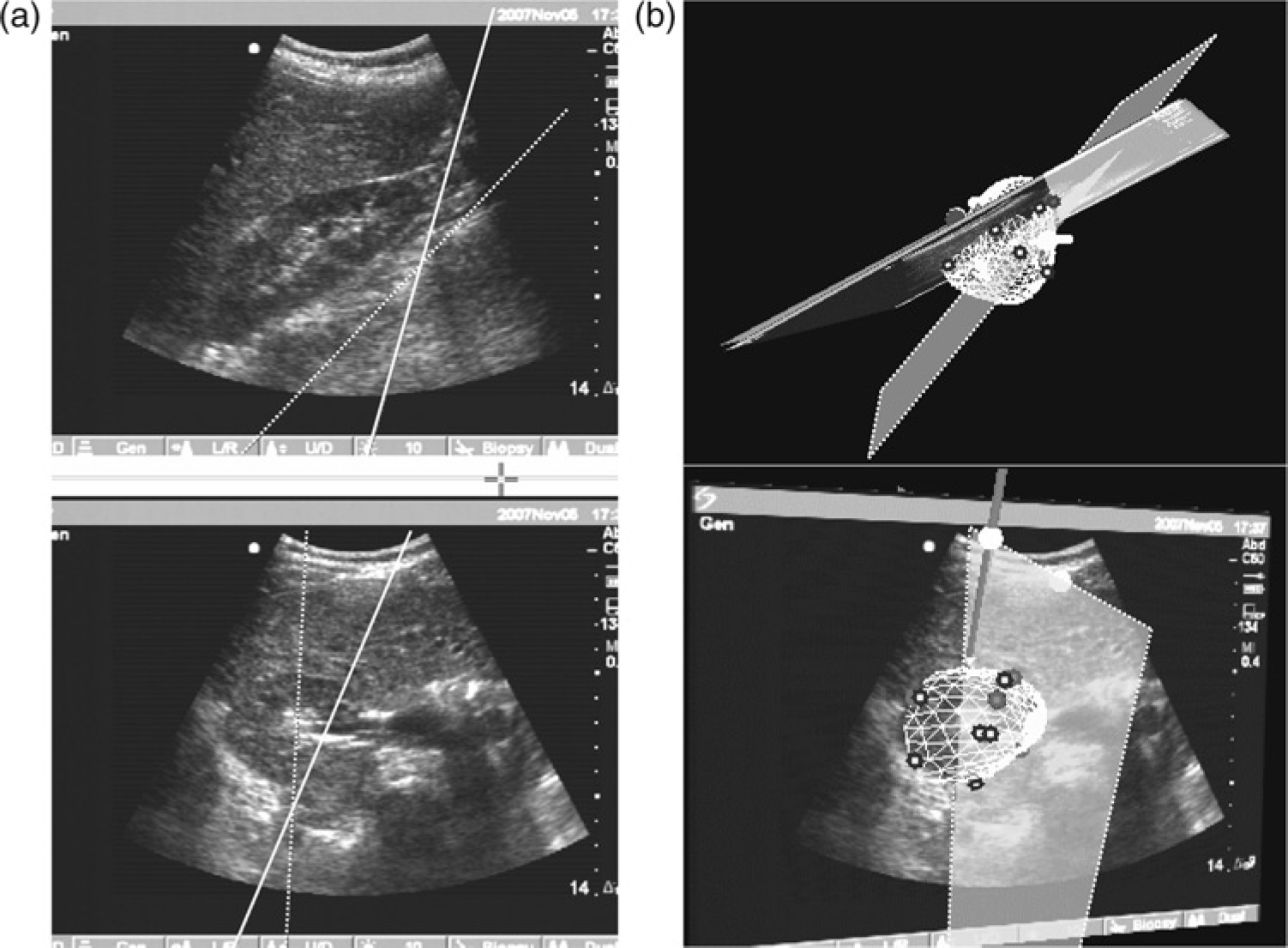
Expert guidance. (a) The expert's guide plane is shown as a line of intersection (dashed line) on the scout images together with the current image (solid line). (b) The expert's guide plane is shown as a plane (outlined with dashed lines) together with the surface
Subjects
Two groups of subjects were recruited for scanning. The first group comprised subjects who underwent 3D ultrasound imaging of their abdominal aorta and/or right kidney in order to populate a database for each test structure. Ten subjects in the first group were patients and 29 were normal volunteers. The aorta database comprised images from eight normal aortas and one aneurysmal aorta. The kidney database comprised images from 30 normal right kidneys.
The second group comprised four subjects who underwent ultrasound imaging during the testing of visual guidance. Two subjects in the second group were patients and two were normal volunteers. One subject had an abdominal aortic aneurysm and a normal right kidney, one subject had a normal aorta and a right kidney with a right upper pole cyst, and two subjects had both a normal aorta and a normal right kidney.
In addition to the test subjects, 20 medical students were recruited to act as inexperienced ultrasound examiners. All were second-year students who had already studied anatomy and pathology. None had previous training or experience in medical ultrasonography.
Image acquisition
Transthoracic 2D echocardiograms were performed on each subject using a portable ultrasound machine (Titan, SonoSite, Inc, Bothell, WA, USA) and freehand scanning. A magnetic field system (Flock of Birds, Ascension Technology Corp, Burlington, VT, USA) was used to track the position and orientation of the transducer. Each subject was placed on a bed constructed of non-ferromagnetic material, and asked to lie completely still during image acquisition. Images were acquired in 2–6 short periods of held end-inspiration lasting about 6 s each. The images and tracking data were acquired on a PC for later analysis.
3D reconstruction for the database
The borders of the target organ and associated anatomical features were traced manually and used to reconstruct the organ as a triangulated mesh using the piecewise smooth subdivision surface method. 7 This method has been shown to accurately measure the volume of diverse shapes such as the left ventricle, right ventricle, papillary muscles, liver and skeletal muscle. 7–10
Examiner training
The 20 examiners were randomly assigned to one of two groups. A sonographer experienced in clinical imaging, telemedicine, and education (the expert) gave both groups instruction for 10 min, aided by posters, on the anatomy of the test structures, the technique for acquiring the specified views and communication with the expert via intercom to mimic the telemedicine scenario. Examiners in Group 2 also received instruction on EVG.
Examiner test protocol
Each of the four test subjects was first imaged by the expert and then by all of the examiners during several imaging sessions. The expert acquired a set of images to establish the presence and visibility of the test landmarks, as well as benchmarks for quantitative analysis. That is, this 3D image set was acquired in order to quantify the competence of the examiners, i.e. the 3D images were not part of EVG. The expert's images were acquired and stored prior to the entry of the examiners into the room.
With the subject supine, each examiner was allowed 20 min to acquire a longitudinal view of the aorta that visualized the superior mesenteric artery branch, a cross- sectional view of the iliac bifurcation and a cross-sectional view that was orthogonal to the longitudinal view. The subject was placed in the prone position and the examiner was allowed another 20 min to acquire a longitudinal view of the right kidney at its maximum length and a cross-sectional view that visualized the renal pelvis. Subjects were permitted to stretch and move about between examinations.
During this process, the expert communicated verbally with the examiners and answered their questions and monitored their activity by video. Group 1 examiners could only see the images on the ultrasound machine. They received verbal assistance from the expert, who was behind a curtain. Group 2 examiners could see the images from the ultrasound machine and also those from the EVG system on an adjacent PC. Group 2 examiners received both verbal instruction and visual guidance from the expert, who accessed the ultrasound images and guidance graphics from another room. The first two modes of guidance, line of intersection and plane of intersection, were available to all Group 2 examiners. The third and fourth modes, 3D reconstruction and expert guidance, were used when the expert felt that the examiner needed additional help.
Examiner image evaluation
Each set of aorta images was graded by the expert for adequacy. Aorta studies were deemed adequate if a longitudinal view was acquired that visualized the superior mesenteric artery and a cross-sectional view that visualized the iliac bifurcation. Kidney studies were deemed adequate if a longitudinal view was acquired showing the kidney at full length and a cross-sectional view that showed the renal pelvis. A study that missed any criterion was deemed inadequate.
Quantitative analysis was also performed. The angle between the best longitudinal and cross-sectional views of the aorta was measured from the spatial coordinates of the respective image plane to measure whether the cross-section was truly orthogonal to the aorta. The contour of the kidney was traced in the best longitudinal view and its longest length was computed. The true length of the right kidney was defined as the maximum length recorded by all observers (i.e. the expert and the examiners). The examiners' results were expressed as a percent of the maximum.
Statistical analysis
The frequency of an adequate grade on imaging the test structures was compared between groups using chi-square analysis with continuity correction. Quantitative data were compared between groups using analysis of variance.
Results
Adequacy of anatomical visualization
The abdominal aorta was successfully imaged in 30 of 40 (75%) examinations by Group 1 and in 37 of 39 (95%; one study was not recorded for technical reasons) in Group 2. The difference between the groups was significant (P = 0.032). Group 2 examiners were also able to visualize the right kidney (39 of 40, 98%) better than Group 1 examiners (35 of 40, 88%) but the benefit of visual guidance was not significant (P = 0.09).
Accuracy of anatomical visualization
There was no significant difference between groups in the angle between longitudinal and cross-sectional views of the aorta. Examiners receiving verbal instruction achieved an angle similar to that of examiners who had EVG (88° [SD 10] vs. 86° [SD 8]), respectively, P = 0.249). Their results were similar to the angle recorded by the expert: 89° (SD 8).
Kidney length (percent maximum) was also similar when measured by Groups 1 and 2 (87% vs. 89%, respectively, P = 0.156).
Ease of instruction with visual guidance
The expert found that the visual feedback afforded by the line of intersection and plane of intersection modes was the most helpful, both for immediately detecting when the transducer was held backwards and for guiding the examiners. The 3D reconstruction was also found to be very helpful in teaching. Only 5% of examinations (2 of 39 aorta examinations and 2 of 40 kidney examinations) were successful in locating the anatomical targets without this aid within the 20 min allotted to each examiner to image the aorta and the 20 min for the kidney. Expert guidance was only utilized for four of the examiners who were having difficulty in locating the anatomy or running out of time.
Discussion
The results of the present study demonstrate a significant benefit of expert visual guidance in assisting inexperienced observers to acquire images of the abdominal aorta and visualize specified anatomy. The benefit was smaller for imaging the right kidney. However the test criteria were probably too lenient, judging from the high score of those who received only verbal instruction.
These results build on the experience of others, who have also reported that visual guidance is more efficient in conveying expert directions to the examiner than verbal instructions alone. For example, Suenaga et al. projected a bull's eye pattern onto the patient's skin to show the examiner where to place the transducer. 11 The study showed that inexperienced examiners achieved specified views in half the time using this visual aid than when directed by the expert using only verbal instructions. In addition experts found it easier to direct the transducer manipulations when provided with video cameras showing the patient and examiner. 11
Limitations of the method
The present study simulated a tele-ultrasound scenario in which a remote expert attempted to guide an inexperienced observer in acquiring medical ultrasound images. The efficacy of EVG was tested in terms of the adequacy of the diagnostic examination, but not its efficiency. Further testing in a clinical setting is required to confirm the benefit of visual guidance and to measure the time savings for the expert.
Subjects were required to lie on a table free of metal components, which would have interfered with the sensor and image acquisition by the EVG system. This was not a major limitation in practice.
In the present study, the expert scanned the patient initially to acquire 3D images used to measure examiner performance. In a telemedicine scenario, the expert would not have had the opportunity to become familiar with the patient acoustic windows and anatomy. Also, the EVG system would need to be populated with databases for all anatomical structures that might need to be imaged. Nevertheless we believe that the comparison of two approaches to coaching an examiner is valid, because the same expert coached both the video and voice alone group as well as the expert visual guidance group.
Clinical implications
Patients generally appreciate the advantages of telemedicine, including the speed of obtaining specialized health services not available in their community and avoiding the need to travel long distances to a tertiary care centre. 12 Most are sufficiently satisfied to use it again or recommend it to others. 13–16 Referring physicians also feel that telemedicine improves their ability to manage patients and would recommend the modality to colleagues. 17 However as many studies have shown, diagnostic success in tele-ultrasound appears to depend heavily on expert availability to assist rural examiners acquire the images, particularly in complex or unusual cases. 2,3,12,17 Indeed the availability of expert assistance lessens the need for prolonged sonographer training. 18,19 This need for real-time rather than asynchronous transmission adds to the cost and complexity of the consultation. EVG is a method to improve the efficacy with which the expert directs the examiner. By adding a visual and anatomical component to this interaction, the expert's directions can be more effectively conveyed to the rural examiner.
Our experience has demonstrated that an inexperienced ultrasonographer can be significantly assisted by EVG compared to verbal instruction alone. This could be useful for tele-mentoring in rural hospitals as well as for teaching, both in person and at a remote site.
Footnotes
Acknowledgements
This work was supported by a grant from NIH/NIBIB. Dr Sheehan is a founder and equity holder in VentriPoint, Inc. The other authors have no conflicts of interest.