
Abstract
A pilot trial of telemedicine in primary care began in the village of Letham in 1998. The service provided conventional consultations with the district nurse, plus teleconsultations with a general practitioner (GP) at the health centre in Forfar, a few km away. In the first year, the videoconferencing link was used by 14 patients, all aged over 65 years. The telemedicine service was judged to be successful and subsequently expanded to patients of any age. It was used for a wide range of health matters, including postnatal care, mental health problems, physical ailments, receiving test results and discussions with the doctor. During the 11-year study period, a total of 646 teleconsultations were conducted, a median rate of 65 per year. A qualitative evaluation of the service was conducted in 1999. Although the GPs involved expressed some reservations about the limited video quality, all three user groups were positive about the service. Nonetheless, the telemedicine service was not adopted as a routine method of health-care delivery by the NHS. To enable any telemedicine application to move from the pilot trial stage to routine service requires several things to happen at an organisational and contractual level. Ultimately an organizational decision about adoption is required, followed by appropriate mechanisms to enable diffusion.
Introduction
Telemedicine has been used sporadically around the world to support general practitioners. For example, a remote general practitioner (GP) in a mining town in Western Australia used a telemedicine link to obtain support from clinical specialists in Perth, about 1800 km away. 1 Over a two-year period, a total of 90 teleconsultations were carried out. About one-third of the injuries to mining construction workers were eye problems. In more than 75% of teleconsultations a patient transfer to Perth was avoided.
In the UK, a randomised controlled trial was conducted during the year 2000 of joint teleconsultations between GPs and hospital specialists. 2 The trial demonstrated that outreach teleconsultations resulted in significantly higher levels of patient satisfaction than standard outpatient appointments and led to substantially fewer tests and investigations. However, teleconsultations were variably associated with increased rates of offer of follow-up according to speciality and site. The main hypothesis that virtual outreach would be cost neutral was not supported.
In 1994, a nurse-led clinic was established in central London with telemedicine support from a main hospital accident and emergency department. 3 The purpose of the clinic was to manage patients with minor injuries. The introduction of telemedicine support was associated with an increase in the proportion of patients that could be managed by the nurse practitioners without requiring referral to a doctor elsewhere.
Setting
The present work took place in the large rural village of Letham in north-east Scotland. In 2009, the population of Letham and surrounding area was about 3000, having almost doubled in the previous 20 years. The demography of the village has also changed, from being mainly retired people who have lived and worked around Letham all their days, to a mixture of retired people and commuters with young families. The local school was upgraded a few years ago to cope with the growing number of pupils, but is now struggling to cope with the numbers.
There is no GP in the village and public transport is limited. Another village nearby with a smaller population (1800) does have a practice with two GPs. This has caused resentment in Letham, which is served by eight GP practices altogether, the nearest of which is 10 km away and the furthest is 20 km away. GPs from the Forfar practice used to visit twice weekly, but this ceased some years ago and home visits are only made on request.
Public transport has improved over the years, but trying to arrange appointments to coincide with buses is difficult and can mean a wait of up to 2 hours for the next bus. Car ownership in Letham has also increased, but many elderly people are not keen to drive into towns and use their cars mainly for getting around Letham and to visit the local shops.
Primary care in Letham
A primary care service, supported by telemedicine, began in 1998 and is still operating, nearly 12 years later. The service initially comprised a weekly nurse-run clinic, which was available to patients over 65 years of age for first consultations. The service provided conventional consultations with the district nurse, plus teleconsultations where appropriate with a GP at the practice in Forfar. While many problems such as minor ailments could be handled by the district nurse, others were more suitable for video consultation with the GP; the nurse then arranged this for the following day. In this way patients avoided the 10 km journey to their GP surgery in Forfar. The service operated from 1998 to 2002 with a single GP and nurse. After the GP in question retired, there was a hiatus until a new GP took over responsibility for telemedicine. There were also problems with the nursing service because the nurse could not always be available owing to other commitments. A team of four nurses was therefore trained by her to support the service.
The aims of the service were:
To provide consultations for the villagers of Letham; To improve patient care; To help the district nurses with their workload; To improve the nurses' job satisfaction.
Equipment
The telemedicine equipment in Letham comprised a desktop videoconferencing unit, and an additional video camera for close-ups. The GP's surgery in Forfar was equipped with a similar desktop videoconferencing unit.
Videoconferencing unit
The videoconferencing units were standard commercial videophones (VC7000, BT). This equipment was introduced in 1993 and was available commercially for about five years. It was manufactured by Tandberg (Vision Classic) and sold by BT as the VC7000 (see Figure 1). The VC7000 was a low-cost digital videophone, with a 25-cm colour cathode-ray tube display screen. It was normally connected to a basic-rate ISDN line and could operate at either 64 or 128 kbit/s bandwidth. The videophone cost £7500 (equivalent to £11,250 at 2010 prices). All the work described in the present study was conducted at a bandwidth of 128 kbit/s

Videoconferencing unit
Close-up camera
The close-up camera was a standard commercial home video camera. Initially a tripod-mounted camera (Panasonic) was used; this was subsequently replaced with a hand-held camcorder camera (Viewcam VL E37, Sharp). The camera was connected to the composite video input on the VC7000.
Technical quality
Videoconferences were conducted at CIF standard, i.e. video pictures of 352 × 288 pixel resolution, at a frame rate of 30 per second.
Patients
The initial criteria agreed for patients to be suitable for video consultation were:
The patient required more than advice from the nurse; The nurse could not provide the necessary prescription; The patient did not require ‘hands on’ assessment from the GP; The patient was registered with the practice in question; The patient was aged over 65 years.
A protocol was drawn up to facilitate the process of helping patients consult with their GP using telemedicine equipment.
As the the service evolved over the first 2–3 years, the telemedicine clinic was opened to all age groups, starting initially with those over 18 years old, then babies and children. In addition, the senior nurse became an independent prescriber, which allowed her to assess and treat certain conditions and to carry out care, such as hypertensive care, with the agreement of the GP using a clinical management plan. The senior nurse was also trained to carry out and prescribe for patients in other areas, such as smoking cessation.
Experience
Nurse-led clinic
The average number of patients seen at the nurse-led clinic was approximately 450 per year once it was fully established in 1999. These patients came from all eight practices covering the area. Approximately 40% were registered with the practice in Forfar, i.e. there were about 180 per year from the practice that employed telemedicine.
Teleconsultations
During the 11-year study period, a total of 646 teleconsultations was conducted (see Figure 2). In 2003, the number of teleconsultations fell sharply. This was due to the GP retiring and there being no suitable replacement. The median rate of teleconsultations during the study period was 65 per year. That is, approximately one-third of patients from the practice that employed telemedicine who presented at the nurse-led clinic were managed by telemedicine.
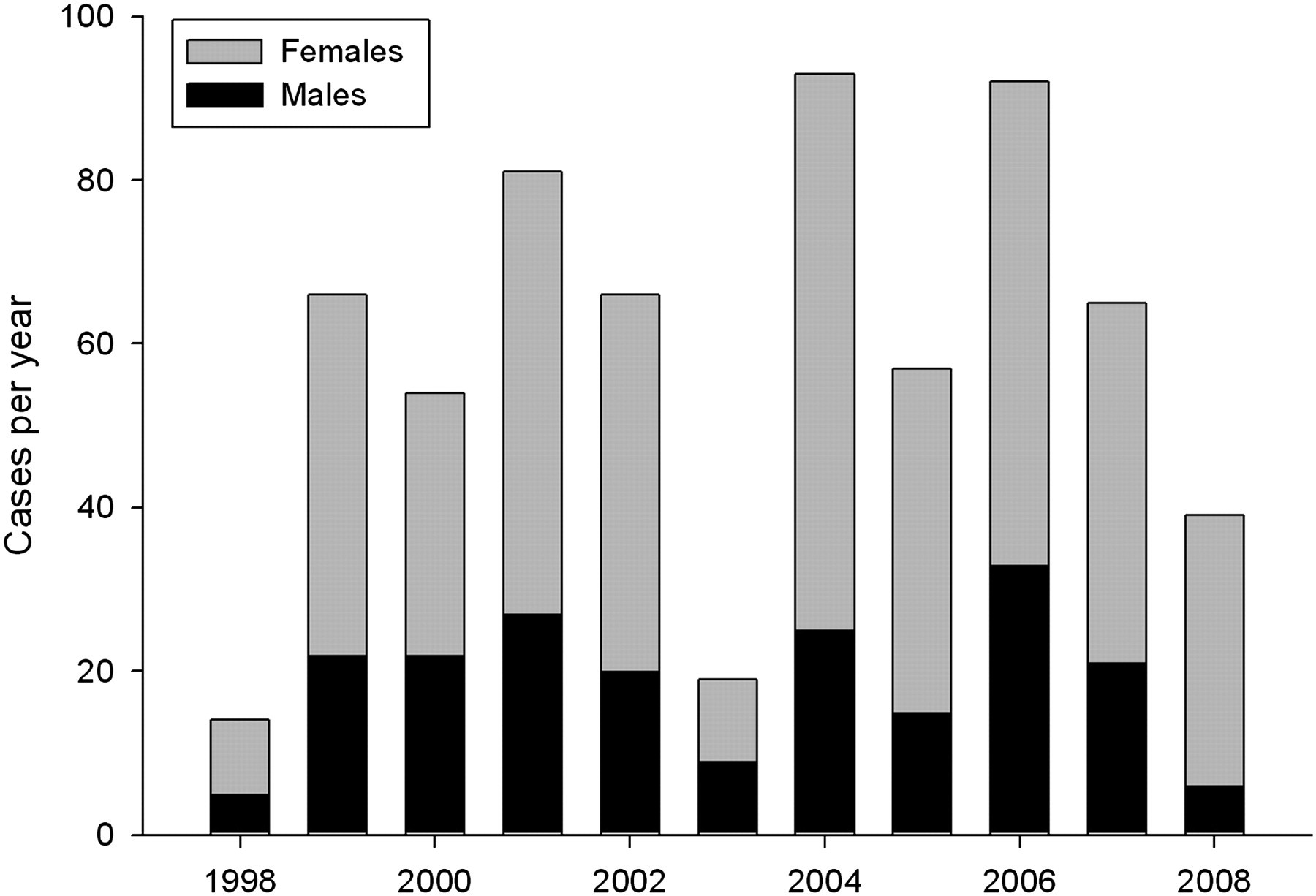
Annual number of teleconsultations (n = 646)
Of the 646 telemedicine patients, 205 were male and 441 were female. In conventional consultations in general practice, females tend to outnumber male patients. Also, older females tend to outnumber older males.
The median return rate was 55%. This was calculated as the number of patients returning for a teleconsultation with the same problem. Non-telemedicine patients attended the nurse clinic for similar problems to those attending for a teleconsultation. In the nurse clinic, patients sometimes returned several times for follow-up visits, which could be weekly or monthly. Some follow-up visits were 6-monthly, e.g. for blood pressure monitoring. The case mix is shown in Table 1. The largest single category was dermatology (19%).
Annual case-mix
Discussion
There are few reports of telemedicine being used routinely in general practice and we are unaware of any other services which have been in operation for periods of ten years or more. The present report reviews a long-running telemedicine service that was clearly popular with the users (both patients and health-care staff) and provided access to a general practitioner more quickly and with less travelling than by conventional means.
In 2004, a systematic review of the literature on nurse-led telemedicine clinics was conducted by Mennie.
4
A total of 40 papers was reviewed, of which 22 met the inclusion criteria (e.g. telemedicine in a nurse-led clinic). There were 29 different themes mentioned in the 22 papers. The five most common themes were:
Costs (in relation to provider and patient); Reductions in waiting time; Reduction in readmission rates; Patient/nurse satisfaction and benefits; Legal issues. Cost reductions (provider savings through telemedicine and patient savings on travel costs); Reduced waiting times; Reduced readmissions; High levels of patient satisfaction. Deal with more complex cases; Complete all of the patient's care; Establish and maintain a very positive role with the patient; Experience high morale and job satisfaction; Have opportunities for professional development. Patients accepted telemedicine as being a good way to consult their GP. The survey showed that 92% were satisfied or fairly satisfied. The main reason for dissatisfaction was technical, e.g. the screen was too small or they were unable to hear the doctor properly. However, all the patients who answered the questionnaire were happy to have the support of the nurse, commenting that the nurse gave reassurance, could discuss their problem after the teleconsultation and arrange their follow-up care. Other comments about the nurse clinic were its convenience, the absence of parking difficulties, the ease of making appointments and the reduced need to travel; Doctors were happy with the consultations via the video link and the support that the nurse gave. They felt that the ideal was to see patients in person, but that telemedicine provided a good alternative. They found fewer communication errors with their instructions for test requests to the nurse, because requests were relayed directly to the nurse via the video link rather than having to leave a message on an answering machine. It saved them travelling time; Nurses were very enthusiastic about teleconsultations as it provided them with more job satisfaction, since they were involved in the patients' care from their initial assessment. Use of telemedicine helped to identify training needs and allowed them to employ their various skills and knowledge. The nurses also had time with the GP to discuss other patients they were seeing in the community.
Mennie concluded that there were substantial patient care benefits from nurse-led telemedicine, in terms of:
Also, the nurse was able to:
A qualitative evaluation of the service in Letham was conducted in 1999.
5–7
Although the doctors involved expressed some reservations about the limited video quality, all three user groups were positive about the service:
Despite these positive views, the telemedicine service in Letham failed to become adopted into routine practice across Scotland.
Telemedicine adoption
Studies of the adoption of telemedicine in the USA have suggested that a number of factors are important, including reimbursement. 8 This is not directly relevant in a publicly-funded health service, such as the NHS. However, other factors such as persuading physicians to practice telemedicine or to refer patients, or to recruit physicians who will be involved actively in one or the other role are clearly relevant to the situation in the UK. Grigsby et al. also observed that most efforts to encourage physicians to adopt telemedicine have focused on the supply of specialists, rather than attempting to stimulate demand among GPs who have patients to refer. Habit was identified as an important, albeit overlooked, factor explaining physician adoption of telemedicine. In a separate study, Whitten et al., found that non-adoption of a telemedicine application was partly because managers did not endorse its use, or offer incentives for using the new technology. 9
Masella and Zanaboni have reviewed the stages in the adoption of telemedicine innovations into routine service delivery. 10 After the introduction of a pilot service, an initial assessment of its feasibility allows a decision to be made about proceeding to clinical trials. Following trials, an evaluation of clinical and cost-effectiveness can then be made. At this point it should be recognised that there are two separate aspects of subsequent implementation: adoption and diffusion. Adoption is the decision to make full use of an innovation as the best course of action available, and diffusion is the process by which the adopted innovation is communicated through appropriate channels to the members of the organisation. It is clear that the telemedicine service in Letham moved successfully beyond the pilot stage, but that the process stalled during the evaluation stage.
To enable a telemedicine application to move from the pilot trial stage to routine service requires several things to happen at an organisational and contractual level. For example, video consultations need to be identified in organisational databases, so that a cost and payment can be attached to them. Training needs to be specific and recognised, and should start early on at undergraduate level for both nurses and doctors. Although telemedicine provides the opportunity for integrated team working, contractual mechanisms are required to enable teams or individuals to be paid for the use of the technique. In addition, without fiscal evaluation there is no drive to change health-care delivery systems. The absence of these mechanisms for diffusion in Letham, and the lack of an organizational decision about adoption, explain why after 11 years of successful telemedicine work in nurse-led primary care, the technique has still not entered the mainstream.
Lessons learned
The attempts to expand the project to provide a more general service locally and in other areas of Scotland proved both negative and educational. Patients were generally supportive, but organisations and professionals require more information, incentives and infrastructure before they become fully committed. Our data show the fluctuations in usage which result from changes in the interest and availability of clinicians who need to be persuaded of the value of working in this way, given adequate training and payment for their efforts. Organisations need good economic data to show effectiveness and efficiency, and appropriate governance and safety measures are also required. In addition, it is necessary to provide robust technical infrastructure, to code consultations so that they can be measured and to persuade the managers to adopt new ways of working in traditionally rigid and bureaucratic structures. All this has to be seen in the social context of aggressive tabloid journalism, where changes that can be portrayed as reducing face-to-face contact are often labelled as cuts. Future developments depend on the improved interactions between organisations, professionals and patients.
Footnotes
Acknowledgements
We thank QNI for Scotland who provided funding and the Academy Medical Centre in Forfar for their continuing support and assistance with the pilot. We also thank Margaret Allan, Linda Gray and Laura Terrell for secretarial support.