
Abstract
We assessed the effects of a care coordination home-telehealth (CCHT) programme on health service utilization. The subjects (n = 387 for each group) were US veterans diagnosed with diabetes and followed for 48 months. The service utilization measures were numbers of all-cause inpatient stays and outpatient visits during the follow-up period. We used generalized linear mixed models to estimate the adjusted effects of the CCHT programme on service use over time. Compared with the controls, the CCHT clients were less likely to be admitted for inpatient care during the first (P < 0.001) and second (P < 0.01) six-month follow-up period, and were consistently more likely to visit outpatient clinics (P < 0.001) during the whole 48-month follow-up period. The likelihood of increase in outpatient utilization tended to decline over time. The findings suggest that the CCHT programme helped to reduce overall inpatient and outpatient use by the clients over the 48-month follow-up period.
Introduction
Diabetes is a common condition which affects nearly 24 million people in the USA. 1 It is a leading cause of blindness, end-state renal disease and amputation. 2 Within the US Veterans Health Administration (VHA) system, over one million veterans have been diagnosed with diabetes, which represents nearly 20% of all VHA patients. 3 On average, veterans with diabetes have six primary care clinic visits and spend approximately eight inpatient days in hospital each year. 4 Every year, the VHA spends about $215 million and $1.5 billion on outpatient and inpatient care for patients with diabetes. 5
The VHA care coordination home-telehealth (CCHT) programme was developed as a part of the transformation from hospital-based care to one that emphasizes ambulatory and patient-centred care. 6 To date, over 40,000 veterans have been enrolled in the CCHT programme. 7,8 Veterans enrolled in the CCHT programme receive a home telehealth device (messaging device) that is connected to a telephone socket in their home. CCHT clients answer questions from the messaging device about their symptoms and health status every day. Care coordinators monitor the daily information from the devices and take follow-up actions such as: (1) making a telephone call to the patient; (2) arranging a referral to the patient's physician or scheduling new appointments with VHA clinicians; (3) placing new orders for patient medications; (4) helping patients manage their medications; (5) reminding patients of their clinic appointments; and (6) assisting with technology difficulties. The CCHT programme has been described in more detail elsewhere. 9,10
A few observational studies have examined the association between the CCHT programme and health service utilization. During the first 12 months after enrolment, CCHT clients with diabetes had a 50% reduction in the number of inpatient stays, an 11% reduction in emergency room use and a three-day reduction in average hospital stay length. 11 During the first 24 months after enrolment, CCHT clients with diabetes were significantly less likely to be admitted for all-cause inpatient care than matched controls. 9 In the present study, we have assessed the effects of the CCHT programme for diabetes on the average number of inpatient stays and outpatient clinic visits over a follow-up period of 48 months.
Methods
The intervention group consisted of 387 veterans who were diagnosed with diabetes and enrolled in a CCHT diabetes programme at one of four VHA medical centres in a single VHA region. To be enrolled in the CCHT diabetes programme, veterans had to (1) be multiple users of inpatient or emergency services from one of the four VHA centres within the 12 months prior to enrolment; (2) be non-institutionalized; and (3) have a landline telephone at home to connect the messaging device.
The control group also consisted of 387 veterans with diabetes. These patients had not been enrolled or approached by the CCHT programme. They were selected from a pool of patients who were matched by the CCHT clients' date of enrolment, VHA medical facility and diabetes diagnosis, as well as age and gender. To ensure the quality of the matching, we applied the propensity score method to enhance the balance between the two groups of patients. The propensity score is a single summary score of patient's characteristics which represents the probability that a patient belongs to a naturally occurring intervention group. 12 This method has been used extensively in research that uses surveys of observational data, and it has the potential to reduce selection bias. 13 More detailed information about the propensity score applied in the CCHT programme study can be found elsewhere. 9,11,14
All study patients were community-dwelling veterans, had a primary diagnosis of diabetes, and were followed for four years post-baseline. The study was approved by the appropriate ethics committees.
Dependent variables
The dependent variables were the number of all-cause inpatient stays and outpatient clinic visits, within the 48 months post-enrolment. Service utilization data were extracted from VHA Medical SAS Patient Treatment File for inpatient care and from the Outpatient File for outpatient clinic visit information during the follow-up period.
Covariates
Race/ethnicity (white vs. all others) information was obtained during the baseline interview for the intervention group only and extracted from the VHA inpatient and outpatient databases for the control group. Patients' sex (male vs. female) was obtained from the VHA inpatient database, and their priority for VHA medical care (high vs. low) was calculated based on their Means Test indicator in the VHA inpatient database. 15 The four VHA centres (study sites A, B, C and D) provided care for patients in both groups.
A modified Charlson co-morbidity index was used to assess the co-morbid conditions: the higher the weighted score the more severe the burden of co-morbidity. 16 The information was collected during the six months prior to the patients' enrolment from the VHA inpatient and outpatient databases. We also obtained the number of inpatient stays and outpatient clinic visits during the 12 months prior to the patients' enrolment.
Statistical analysis
Generalized linear mixed models were fitted to estimate the effects of the CCHT programme on each of the utilization variables (inpatient stays and outpatient clinic visits) over a period of 48 months, with adjustment for age, sex, marital status, race/ethnicity, priority for VHA medical care, co-morbidity, pre-enrolment inpatient and outpatient utilization, and study sites. The generalized estimating equation method was used for parameter estimation since the dependent variable consisted of repeated measurements. All analyses were conducted using a standard package (SAS version 9.13, SAS Institute, Inc, Cary, NC, USA).
Results
At baseline there were no differences in characteristics between the intervention and control groups, including pre-enrolment inpatient use (see Table 1). Compared with the control group, the intervention group had a significantly higher co-morbidity score during the six months pre-enrolment (P < 0.02) and had a higher number of outpatient clinic visits (P < 0.0001) during the 12 months pre-enrolment. In addition, the intervention group had a smaller proportion of deaths than the control group during the 48-month follow-up time period (P < 0.002).
Patient characteristics at baseline
*Chi-square tests on discrete variables, t-tests on age and Wilcoxon tests on co-morbidity summary score
The average number of inpatient stays and outpatient visits in the two study groups are shown in Figures 1 and 2, respectively. There was a significant increase in inpatient stays for the intervention group between months 12–24 (P = 0.02), but no significant change after that. For the control group, the inpatient utilization pattern was almost exactly reversed. The intervention group consistently had more outpatient visits than the control group during the entire follow-up period (Figure 2). There was a general pattern of reduced inpatient and outpatient use by the intervention group compared to the control group over the 48-month follow-up period.
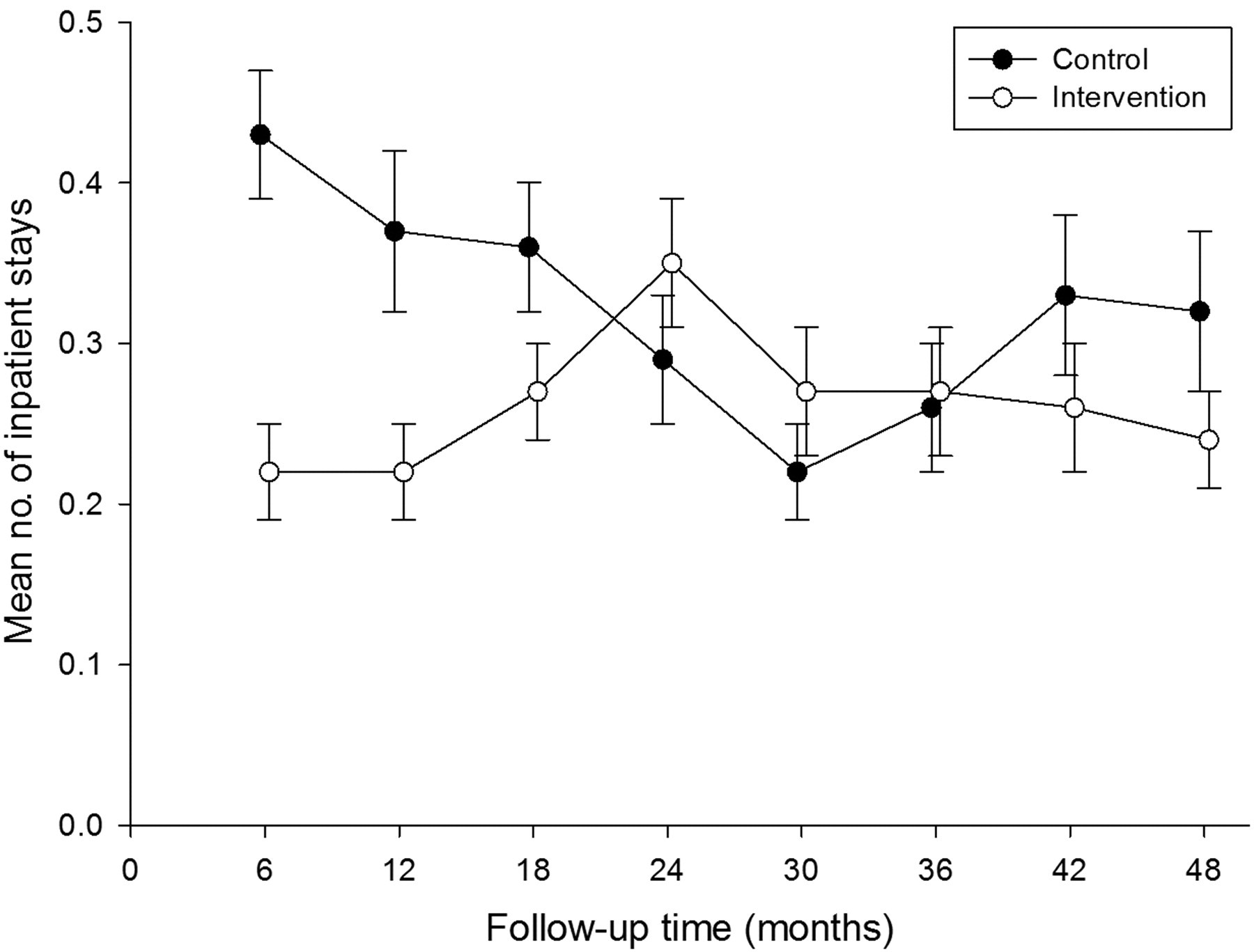
Average number of inpatient stays
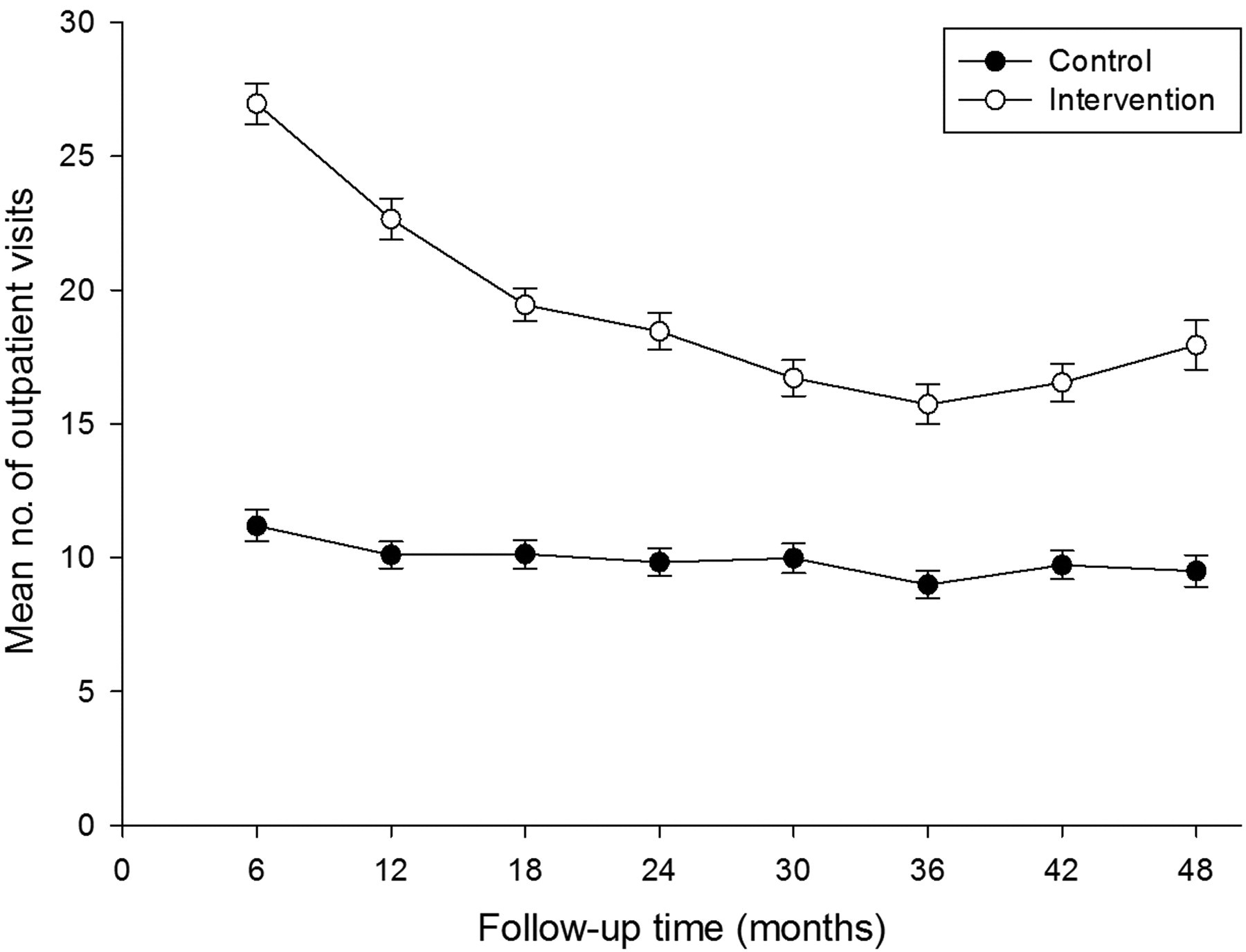
Average number of outpatient visits
There was a significant reduction in number of outpatient visits in the intervention group after 48 months (P < 0.001). There was no significant change in inpatient stays (Table 2).
Utilization after 48 months
*Chi-square test on cumulative death, and Wilcoxon tests on mean number of inpatient stays and outpatient visits
The relative risks (RR) and 95% confidence intervals (CI) from the generalized linear mixed models are shown in Table 3. Compared with the matched controls, the CCHT clients were less likely to be admitted for inpatient care during the first (P < 0.001) and second (P < 0.01) six-month period. After 12 months, however, the likelihood of inpatient admission was not significantly different between the two groups of patients. Throughout the 48-month follow-up period, the CCHT clients were more likely to visit outpatient clinics (P < 0.001) than the control patients. However, the likelihood of more outpatient visits tended to decline over time.
Relative risk and corresponding confidence interval of inpatient stays and outpatient visits
*P ≤ 0.05,† P ≤ 0.01,‡ P ≤ 0.001
Several covariates were associated with the utilization variables. Not being married, greater co-morbidity and using more inpatient and outpatient services prior to enrolment were found to be significant predictors for inpatient stays. Older age, being married, using more outpatient services, being in study centres A and D (vs. B) were all significant predictors for outpatient clinic visits.
Discussion
A recent systematic review and meta-analysis of studies on home telehealth and diabetes management called for more studies of higher methodological quality. 17 Our study used a quasi-experimental design to enhance the balance between the two groups of patients. The systematic review 17 reported that home-telehealth helps to reduce the number of hospitalizations and bed-days of care, but these variables were not studied for longer than 12 months. The present study extends existing knowledge by assessing utilization over a 48-month period. Our findings demonstrated that compared with matched controls, patients enrolled in the CCHT programme were 45% and 37% less likely to be admitted for inpatient care during the first and second six-month periods, respectively, even after adjusting for the different sociodemographic, co-morbid and pre-enrolment utilization factors. Our findings are consistent with previous reports of reduced inpatient stays by CCHT clients within the first 12 months 11 and 24 months post-enrolment. 9
During subsequent six-month intervals, however, the adjusted inpatient utilization appeared to fluctuate with the clients being more likely to be hospitalized between months 18 and 36 compared with controls. The increase in the likelihood of inpatient use by the intervention group may have been due to the increased number of deaths in the group during the same periods. The 48-month cumulative mortality in the intervention group was significantly lower than the control group (Table 1). However, the intervention group had significantly higher mortality (P < 0.002) than the control group during the second (33% vs. 27%) and third (31% vs. 18%) follow-up years, respectively (data not shown). The high mortality during the first and second year increased the groups' inpatient care.
We also found that the CCHT clients had more outpatient clinic visits than the controls throughout the follow-up period, both with and without adjusting for the risk factors. During the first and second six-month intervals, the clients were more than twice as likely to visit an outpatient clinic as the controls. This may have been due to the fact that the intervention group had a significantly higher co-morbidity score before enrolment and more outpatient clinic visits before enrolment than the control group. This may also have been due to the fact that the programme's coordinators helped arrange new clinical appointments for the clients. Increasing the number of outpatient visits could help to reduce the overall number of hospitalizations, particularly hospitalizations for ambulatory care-sensitive conditions as previously reported. 15
The present study had several limitations. First, our study patients were all veterans who were enrolled in the VHA health-care system. Since VHA patients are mainly male, older, and have more co-morbid conditions than the general US population, our findings may not be generalizable. Second, the patients all came from a single region of the VHA health-care system, which may also limit generalizability. Third, patients in the intervention group were selected from the CCHT programme of four VHA centres. The inclusion criteria for these CCHT programmes included the multiple use of inpatient and/or emergency services prior to enrolment. As a result, patients in the intervention group had significantly more co-morbid conditions and outpatient visits than the control group.
Notwithstanding these limitations, our findings suggest that patients in the CCHT programme were significantly less likely to be hospitalized than those in the control group during the initial 12 months post-enrolment, after adjusting for the risk factors. Our results also indicate that the intervention group had lower inpatient and outpatient use over the 48-month follow-up period. Randomized clinical trials of the CCHT programme will be necessary to confirm the findings of the present study and to examine the long-term effect of the CCHT programme on health service utilization.
Footnotes
Acknowledgements
The study was supported by the Community Care Coordination Service at VHA Integrated Service Network 8 and the VHA Health Services Research and Development/Rehabilitation Research and Development, Rehabilitation Outcomes Research Center Research Enhancement Award Program at the North Florida/South Georgia Veterans Health System. The views and opinions expressed in this article reflect those of the authors and do not necessarily reflect those of the Department of Veterans Affairs.