
Abstract
We evaluated a mobile phone application (Nutricam) for recording dietary intake. It allowed users to capture a photograph of food items before consumption and store a voice recording to explain the contents of the photograph. This information was then sent to a website where it was analysed by a dietitian. Ten adults with type 2 diabetes (BMI 24.1–47.9 kg/m2) recorded their intake over a three-day period using both Nutricam and a written food diary. Compared to the food diary, energy intake was under-recorded by 649 kJ (SD 810) using the mobile phone method. However, there was no trend in the difference between dietary assessment methods at levels of low or high energy intake. All subjects reported that the mobile phone system was easy to use. Six subjects found that the time taken to record using Nutricam was shorter than recording using the written diary, while two reported that it was about the same. The level of detail provided in the voice recording and food items obscured in photographs reduced the quality of the mobile phone records. Although some modifications to the mobile phone method will be necessary to improve the accuracy of self-reported intake, the system was considered an acceptable alternative to written records and has the potential to be used by adults with type 2 diabetes for monitoring dietary intake by a dietitian.
Introduction
The accurate assessment of dietary intake is essential for understanding the relationship between diet and disease, and for the management of a number of chronic conditions. Type 2 diabetes is one such condition in which the prescription of, and the subsequent compliance with, medical nutrition therapy is important to successful diabetes management. 1 There is a need for methods that are practical and simple to use to monitor the diets of people with type 2 diabetes.
In an attempt to reduce incomplete and inaccurate self-reported intake data resulting from the need to keep written food records, 2–5 new approaches to dietary assessment have been developed. In particular, the feasibility of photographic dietary records captured via disposable and digital cameras to quantify intake has been investigated with positive results. 6–9 More recently, mobile phones and personal digital assistants (PDAs) with cameras have been used for recording dietary intake. 10–14 These devices are more compact than conventional cameras, and allow the user to transfer the recorded information immediately to a researcher for analysis. After recording an image, the user must input a description of the items by selecting from a food composition database stored on the device. 13 Alternatively, the user can write the name of the item on the display to assist in the analysis of the data. 10 However, this approach may be restricted to people with the necessary dexterity, technical knowledge and/or literacy skills.
Tape recorders have been used in the past as a method of reducing the burden associated with documenting dietary information. 15,16 However their effect on improving reporting accuracy is not known. The majority of mobile phones allow the user to record and save a voice file. Approaches that further simplify the recording process by combining the camera function of the mobile phone with the in-built voice recorder warrant further exploration.
Nutricam
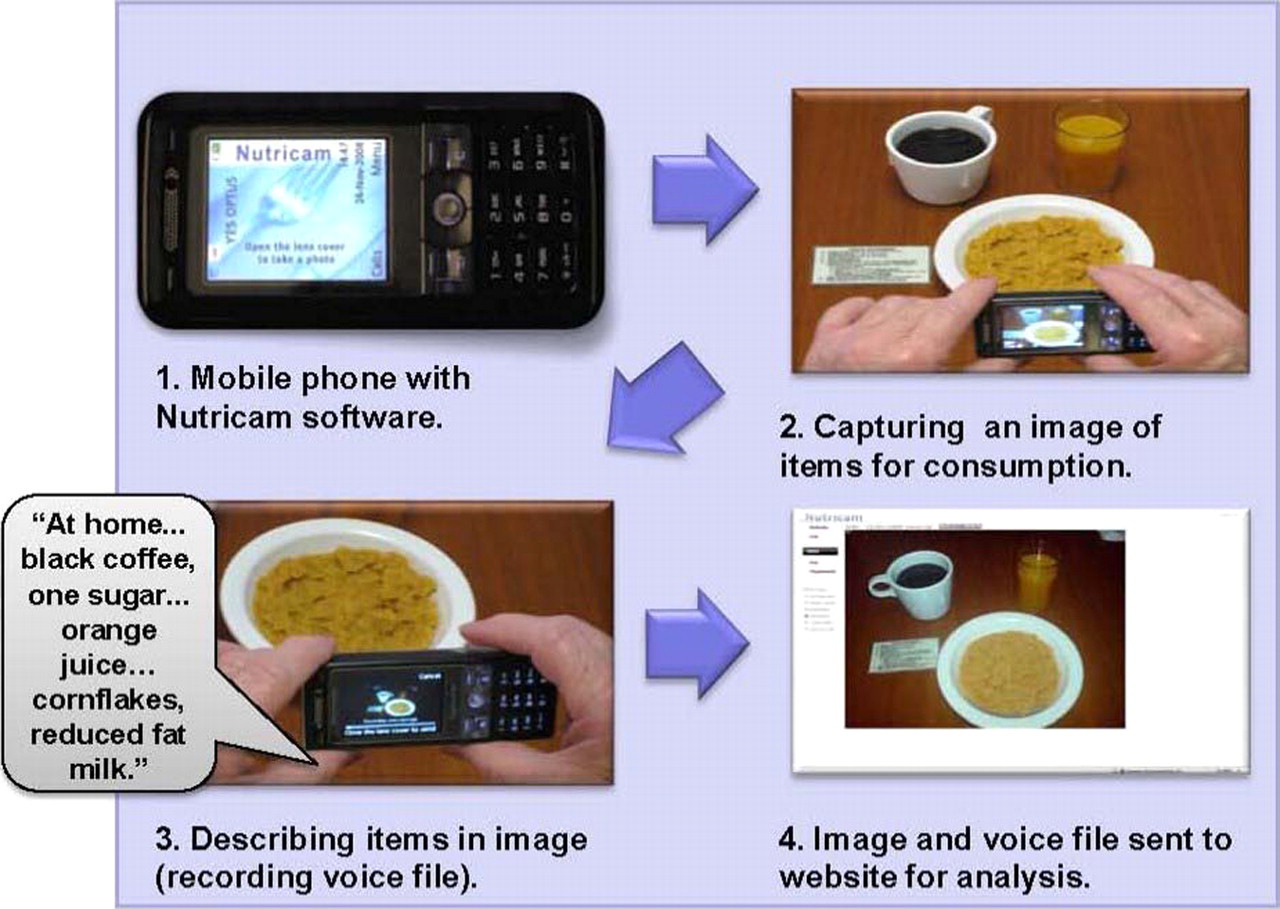
Nutricam is a mobile phone application (Alive Technologies Pty Ltd). It allows users to capture a photograph of food items before consumption and store a voice recording to explain the contents of the photograph. This information is then sent to a website where it is analysed by a dietitian.
A protocol was developed by an Accredited Practising Dietitian for the recording of dietary intake using Nutricam. Prior to each meal, the individual recorded an entry, consisting of a photograph and voice recording explaining the food and/or drink items for consumption. When capturing the image, individuals were instructed to hold the mobile phone camera at an angle of approximately 45° and ensure that all items were clearly visible on the screen of the device (Figure 1). The flash settings on the mobile phone camera were set to automatic. After capturing a photograph, a preview of the image appeared on the phone screen, allowing subjects to check for clarity and inclusion of all items. If any items were not clearly visible in the image, subjects were instructed to re-record the image. The subjects were then prompted to make a voice recording listing the name, type (e.g. low-fat milk), brand/product name and preparation/cooking method of each item. To assist in the consistency of entries, a prompt card with a brief summary of the instructions for recording intake was attached to the back of the mobile phone. This card was placed next to the items to be photographed and acted as reference object during the analysis of the dietary record.
Recording dietary intake using Nutricam
The present study aimed to evaluate the feasibility of the Nutricam system for assessing nutrient intake in adults with type 2 diabetes.
Methods
The study was approved by the appropriate ethics committee. People with type 2 diabetes who were not eligible to participate in a large-scale trial of an automated telephone system for diabetes self-management 17 were invited to participate in the present study. After subjects provided written informed consent, their height and weight was measured. The subjects then completed a questionnaire to collect information relating to demographics, history of recording dietary intake and mobile phone use.
The Nutricam program was installed on three mobile phones (K800i, Sony Ericsson Mobile Communications AB, Sweden) and the camera resolution set to 1 megapixel (1280x960 pixels). At each eating occasion, subjects were instructed to use Nutricam to record all food and drink items to be consumed. Any food and/or drink which was served but not consumed was also recorded. In addition, subjects were required to document all items prior to consumption using a written food diary, with quantities measured using household utensils such as measuring cups and spoons. 18 Recording of intake occurred over three consecutive days (two weekdays and one weekend day). In addition to receiving verbal and written instruction, a demonstration of both dietary recording methods was provided to all subjects.
Following completion of the recording period, subjects were required to complete a written questionnaire on the usability and acceptability of the Nutricam method. Included were nine closed questions regarding the ease of use of Nutricam; the recording of consumed and leftover items; length of time to record using Nutricam compared to written food diary; confidence to use Nutricam again; maximum number of days willing to use Nutricam again to record intake; and preferred recording method. The subjects were asked to elaborate if all consumed and/or leftover items were not recorded using Nutricam and to provide a reason for the preferred method. They were also asked to suggest any improvements to the Nutricam method.
The feasibility analysis consisted of an evaluation of the quality of the dietary data contained in the Nutricam record. The photographic and voice recording components of each Nutricam entry were assessed independently by an Accredited Practising Dietitian. A photograph was deemed acceptable to be used for the quantification of energy intake if all food items could be seen clearly and the reference card was visible. The voice component of each Nutricam entry was determined to be adequate for the identification of dietary items and coding of these items into a food composition database if the four key descriptors of name, type, brand/product name and preparation/cooking method were listed (where appropriate) for each item.
To determine energy intake, the established method of the food diary was considered as the reference. For all subjects, energy intake was estimated for each day of the three-day food diary using a food analysis program (FoodWorks version 5.1, Xyris Software, Brisbane, Australia) and then averaged to obtain mean daily energy intake. To quantify energy intake for the Nutricam method the calculation was based on the quantities recorded for the same items in the food diary. Food items which were missing in either method, when compared to the other, were noted. The missing items from both records were categorized as either a meal, snack, 19 beverage or other (i.e. additional items added to foods, such as sugar or dressing).
The statistical analysis was performed using a standard package (SPSS for Windows, SPSS Inc, Chicago, Illinois). A paired t-test was used to compare the difference in estimated energy intake between methods. A Bland-Altman plot was used to assess the level of agreement between self-reported energy intake as recorded by the Nutricam and food diary methods. 20
Results
Ten adults with type 2 diabetes aged 59–70 years were enrolled. Their BMI was 24.1–47.9 kg/m2, with five subjects reporting a restriction in intake to assist with weight loss. Six subjects had kept a written food record in the past. Nine subjects had used a mobile phone previously, with three using a mobile phone to take photographs.
Evaluation of the Nutricam method
Using the food diary as the reference method, individual differences in energy intake between the two records varied from –6.7 to 29.7%, see Table 1. On average, energy intake was significantly under-recorded using Nutricam by 649 kJ (SD 810) (t = 2.5, P = 0.03). The differences between the two measures of energy intake for each subject are shown in Figure 2.
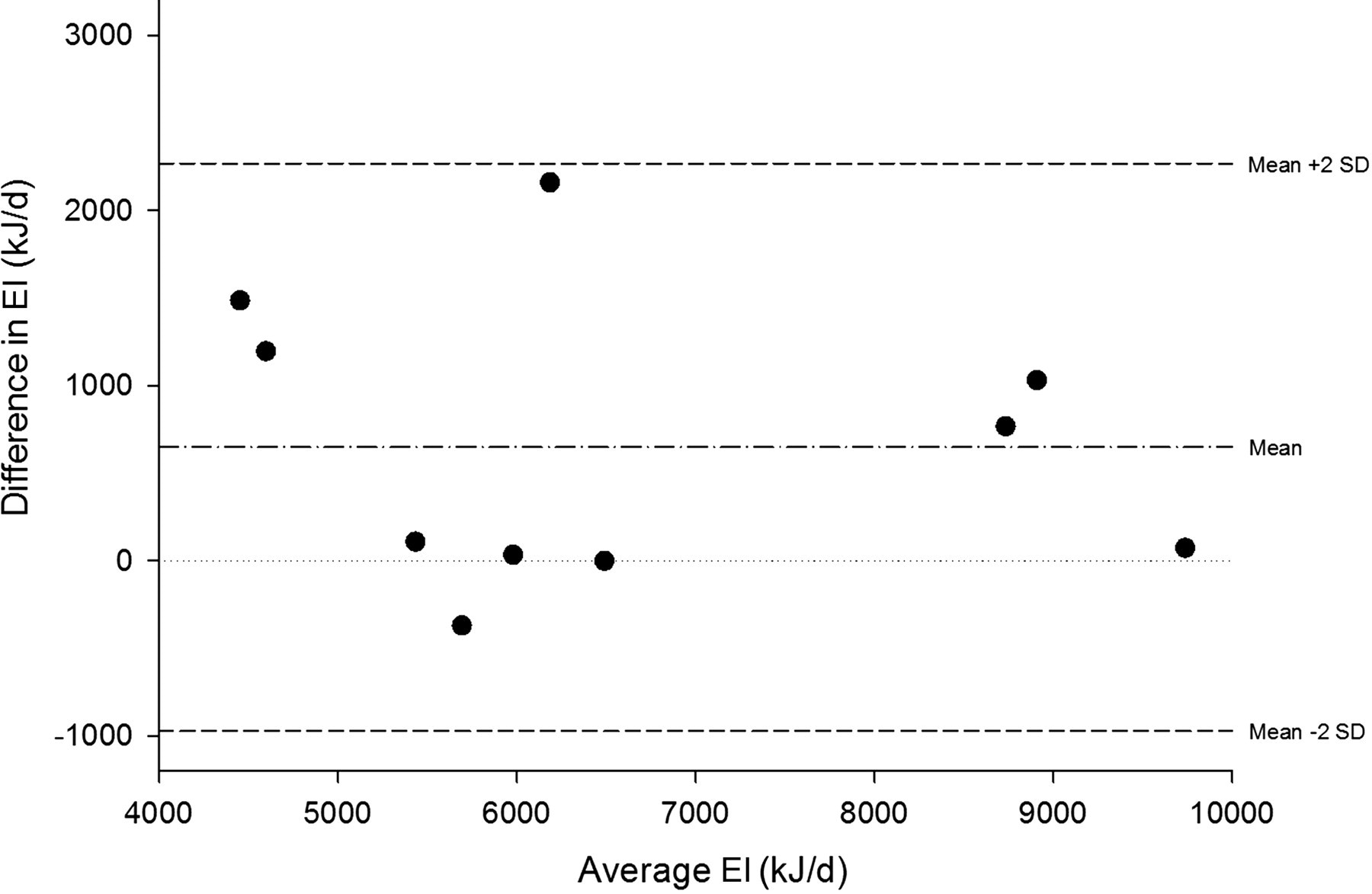
Bland-Altman plot of energy intake (EI) measurements (average and difference between food diary and Nutricam EI estimates)
Estimated energy intake (EI) for each subject
†Mean of 3 days of intake recorded using food diary
‡Mean of 3 days of intake recorded using Nutricam
^Difference=(Mean EI Food Diary – Mean EI Nutricam)/Mean EI Food Diary * 100
*P < 0.05, paired t-test
Over the three-day period discrepancies between both records were identified for 58 of 355 items. Fifty items consumed and recorded by subjects using the written food diary were not subsequently captured via the Nutricam device. Beverages (n = 25) were the items most frequently not recorded using Nutricam, followed by snacks (n = 17) and meals (n = 8). In comparison, eight dietary items present in the Nutricam records were not recorded in the food diary, i.e. beverages (n = 3), meals (n = 2), snacks (n = 2) and other (n = 1). Collectively of the items not recorded by either method, meals contributed the greatest proportion (67%) to the difference in estimated energy intake followed by beverages (16%), snacks (16%) and other (0.2%).
Of the 144 Nutricam entries received, 66% contained a voice recording suitable for estimating intake, 71% included a photograph of adequate quality, and 60% contained both a voice recording and photograph of suitable quality.
Usability and acceptability
All subjects reported that the Nutricam system was easy to use. Six subjects found that the time taken to record using Nutricam was shorter than recording using the written diary, while two reported that the duration was about the same. All subjects felt confident that they could use Nutricam again to record dietary intake, with five subjects willing to use Nutricam again to record their diet for a maximum period of 30 days. Seven subjects preferred the Nutricam method for recording intake, whilst three favoured the written diary.
Discussion
The present study showed that energy intake was significantly under-reported by 649 kJ (SD 810) with the Nutricam method (Table 1). Discrepancies existed in the dietary records of both methods for nine subjects. However, the level of inconsistency in the use of Nutricam was significantly greater compared to the food diary. Although intake was under-recorded using Nutricam, there was no trend in the difference between dietary assessment methods at levels of low or high energy intake (Figure 2).
In addition to a larger number of dietary items not recorded using Nutricam (50 items) compared to the food diary (8 items), missing items were present in the Nutricam records for nine subjects as opposed to four subjects who had incomplete food diaries. The omission of these food items, especially meals, contributed to the difference in recorded energy intake between methods and may have the potential to bias the measurement of intake at the individual level. However a number of factors may offer an explanation for this variability. First, the extent to which the under-recording occurred with this novel method is likely to have been exacerbated by the use of the written food diary at the same time. When using Nutricam some subjects indicated that it was not important to make additional entries for items which had been captured earlier in the day and were then consumed again throughout the same day, such as beverages. For example, one participant commented in regards to not recording repeat mugs of tea ‘…if you have seen it once that is enough’. However, these individuals recorded such items on multiple occasions throughout the day using the written food diary. This observation indicates that a misunderstanding as to the independence of the two dietary assessment methods tested in this study may have been present among the group. Such a belief may assist in explaining the level of missing information contained in the Nutricam record in comparison to the written food diary.
Second, not remembering to record at the time of eating was commonly reported as the reason for a failure to document intake using Nutricam. This has also been reported in similar studies using photographic dietary records. 13,21 In the present study one individual remarked, ‘If not an actual meal is consumed, e.g. a few nuts or grapes, it is easy to forget to record.’ Subjects who forgot to record meals also did not capture snacks and/or beverages, contributing to a greater difference in estimated energy intake between recording methods for these individuals. The two methods used in this study required the individual to record dietary information prospectively; however an opportunity exists with the written food diary method for individuals to document items after consumption. A similar opportunity does not exist with Nutricam and may offer an explanation for the difference in estimated energy intake calculated between the recording methods. Therefore, an additional procedure is necessary to ensure that dietary data not recorded with Nutricam is captured and a more accurate picture of nutrient intake is established (see below).
Some of the data recorded by subjects using Nutricam was unacceptable. On these occasions, the poor-quality photographs consisted mainly of food items which were concealed by other items in the same dish. These food items often contained multiple ingredients that needed to be quantified separately. For example, photographs of breakfast cereal and milk served in the same bowl were consistently rated as unacceptable due to the difficulty of estimating the quantities of the components.
The inability to account for items not clearly visible in the photograph has been previously identified as contributing to the underestimation of the nutrient content in these types of dietary records. 10 These findings suggest that to improve the quality of the Nutricam photographs, modifications to the protocol are necessary. Individuals are now required to make two entries when recording breakfast cereal and milk; the first entry consisting of the dry cereal only, followed by the second entry depicting the cereal with the milk added.
In general, the voice component of the Nutricam record contained descriptions of items which provided insufficient detail for coding and analysis, with the preparation and/or cooking methods often not provided. Mixed dishes without an adequate description of the key component ingredients were also common, even though training was provided prior to recording intake and a prompt card included to promote consistency in the use of Nutricam. Such a finding is not unusual when individuals are asked to record dietary intake, with clarification of the items recorded often necessary. 5 We conclude that an additional mechanism is necessary to clarify the dietary information contained in the Nutricam record to ensure data collection is complete.
The findings from the present pilot study highlighted the need to clarify the content of the Nutricam record and to probe for items not recorded. This supplemental data collection needs to occur so as to increase the chance of the individual recalling accurately the omitted intake information. For this reason, unlike previous methods, 14 we propose that the collection of this information occurs in the morning of the day following recording with Nutricam during a brief (5–10 min) call to the participant. A protocol and standardized tool have been developed for this component of the method.
One factor that may explain, at least in part, the lack of adherence to the recording protocol was the length of time allocated for the voice record. In the present study, the time available to record a description of the items contained in the photograph was set at 20 seconds. Subjects reported that this was not long enough, particularly when recording multiple items and/or complex mixed dishes. We have subsequently extended the voice recording time to 99 seconds.
The Nutricam method was well-received by the group studied, with the mobile phone photo/voice device preferred over the pen and paper approach of the food diary. Those who favoured the Nutricam method collectively reported that it was easier and less time consuming to record. In comparison, preference for the written diary was based on the belief that the method provided more detailed intake information such as brands (n = 2) or required less preparation to record (n = 1). This suggests that there may have been some confusion over the Nutricam recording protocol, as subjects were required to include specific descriptions of the items consumed in the voice recording. However this information was often missing. Similarly, subjects were instructed not to change their eating behaviour to simplify the recording process or by assembling all items prior to consumption. Instead, subjects were asked to use Nutricam each time any food and/or drink was eaten with no restriction placed on the number of entries which could be recorded.
Other studies evaluating the use of similar devices for the recording of dietary intake have also reported a preference for these novel technologies among college students 11 and adolescents. 13 Acceptance of the Nutricam method among this group of older adults with type 2 diabetes is encouraging and prompts further exploration of the use of such devices in this population.
To our knowledge, the present study is one of the first to use a mobile phone application to collect photo/voice dietary records for analysis by a dietitian. Although the small sample size limits the generalizability of the findings, the Nutricam system was considered an acceptable alternative to written records and has the potential to be used by adults with type 2 diabetes for monitoring dietary intake by a dietitian.
Footnotes
Acknowledgements
MR received a Queensland University of Technology Postgraduate Research Award scholarship (February 2008 to July 2009) and an Australian Postgraduate Award scholarship (from July 2009).