
Abstract
In response to the Victorian bushfire disaster in 2009, various telemental health services were provided by three national agencies: Kids Helpline (BoysTown), MensLine Australia (Crisis Support Services) and Lifeline Australia. All provider agencies used their existing national service structures and staff resources, which were expanded to respond to bushfire-related service demand. We examined service provider reports and conducted key informant interviews. Despite a lack of quantitative data on consumer outcomes and perspectives, it appears that all three telemental health services experienced significant increases in overall service uptake levels in the wake of the bushfires. Uptake of specialized telephone-, web-, email- and crisis counselling services was substantial, although that of callback services was very limited. Potential clients encountered specific barriers in relation to service access and the callback model. The bushfire experience highlighted the impact of transitory living circumstances and the increased complexity of post-disaster calls on service provision. Telemental health services need to be integrated into mainstream services and disaster response structures.
Introduction
In February 2009, a series of bushfires devastated large parts of the state of Victoria. These fires affected 51 townships, destroyed more than 2000 homes and resulted in the loss of 173 lives. 1 Large scale natural disasters such as this can have a major impact on the lives of affected people and communities. 2,3 The impact on mental health can either be mild, moderate or severe, as well as short term, enduring or variable over time. 4 Mental health problems can be expected after disasters of all types (Table 1).
Predicted 12-month prevalence of psychosocial problems following disasters
Adapted from Van Ommeren 4
In response to the Victorian bushfire disaster, the Australian government in collaboration with the Victorian state government provided mental health support for the wider population. The services included telephone-based crisis counselling and callback services, and to a lesser extent, Internet-based and on-the-ground support. Services were provided by three national agencies: Kids Helpline (BoysTown), MensLine Australia (Crisis Support Services) and Lifeline Australia. These national services were intended to complement existing avenues for telephone and face-to-face mental health support at state and local levels. 5
We conducted a pilot evaluation of the telemental health services provided as part of the response to the bushfire disaster. The aim was to answer four questions: (1) What is the precise nature and scope of telephone-based counselling and callback services? (2) What is the level of service uptake? (3) What are the benefits and disadvantages of services for those affected by bushfires and (4) What problems are associated with the provision of services to people affected by bushfires?
Methods
Data were obtained from written service provider reports and interviews with key informants. Four project reports (which included an independent evaluation of one project) and supplementary service use data on another project were analysed systematically. Semi-structured interviews were conducted with six key informants from the three provider agencies and the Victorian Department of Health. Respondents were asked about their experience of delivering bushfire services, including the factors that had aided and hindered delivery and suggestions for further improvement. The interviews were recorded and transcribed. Transcripts were analysed by basic descriptive analysis (frequencies, percentages) and thematic analysis.
Results
All provider agencies used their existing national service structures and staff resources, which were expanded to respond to bushfire-related service demand. The three agencies also provided support services such as: (1) training and supervision for counselling staff; (2) interagency networking and service promotion; (3) upgrades to bushfire referral databases; (4) on-the-ground counselling support for bushfire recovery centres and media organisations; and (5) outreach to affected Victorian households.
Nature and scope of services
The service provided by the Kids Helpline (BoysTown) was available between June 2009 and July 2010. It involved a substantial increase in the counselling hours provided by 120 existing staff operating from the national call centre in Brisbane. The service provided specialised telephone, web and email counselling to young people (aged between 5–25 years), as well as parents and caregivers concerned about the impact of the fires on their children. The staff received additional training in relation to trauma, loss and grief, and the impact of disasters on target groups. As part of the project, a bushfire web portal was set up to support those affected by the fires.
The MensLine Australia Bushfire Emergency Aftermath Rebuild service was available between May 2009 and June 2010. It provided telephone counselling support to men and women (aged 15 years and over) affected by the bushfires, as well as to families and friends of those affected, emergency service workers and volunteers. The project operated through a 24 hour, seven days a week intake line and a telephone counselling callback service which provided up to six 50-min counselling sessions, 7 days a week between the hours of 10:00 and 22:00. The callback service was based on the Skills for Psychological Recovery approach. The intake line was operated by the majority of the 45 counselling staff based at the national call centre in Melbourne, who were briefed about the fires and trained in relation to trauma and grief.
Lifeline Australia enhanced the capacity of its national network of 42 telephone centres and 3500 trained volunteer counsellors to provide crisis counselling to individuals who were emotionally distressed by the bushfires, suicidal, or in need of support during times of crisis. This service was available 24 hours a day. In addition, two web-based bushfire forums/chat site facilities were operated immediately after the bushfires and at the time of the first anniversary. These professionally-facilitated forums enabled people to share their experiences and discuss strategies for dealing with bushfire events. Additional online resources such as toolkits for people experiencing trauma, loss and grief were made available on the Lifeline web site.
Service uptake and caller characteristics
Kids Helpline. An analysis of Kids Helpline contacts for the period July 2009 to March 2010 demonstrated a doubling in call volume for bushfire affected areas in Victoria. There were 519 recorded calls from affected regions (as determined by postcode). On the basis of the proportion of contacts with known postcodes (10–15% during the quarterly reporting cycle) the overall call volume (n = 3951) was estimated. Similarly, recorded counselling contacts (n = 314) and relative proportions of known postcodes (32–48%) were used to estimate the overall number of counselling contacts (n = 978). The data did not permit differentiation of bushfire-related and ordinary service calls.
The majority of service contacts were made via the telephone (60–67%) with the remainder taking place through web-based counselling (16–20%) and email (13–22%). ‘Difficulties in managing challenging emotions and behaviours’ were the most common contact reason (27% of counselling contacts) at the start and ‘Mental health issues’ (23% of counselling contacts) at the end of the reporting period. Further contact reasons included ‘family relationships’, ‘sexual assault’ and ‘relationship with peers’. Of the young callers from affected regions, 24–35% were reportedly engaged in self-injuring behaviours and 9–17% had current thoughts of suicide at various intervals during the reporting cycle. The majority of callers were female (>74%), aged between 15–25 years, and from Caucasian backgrounds. Of the counselling type contacts, 6–18% involved a referral to a specialised service and 11–13% a non-specific referral to a GP or school counsellor.
During the quarter around the time of the first anniversary (January to March 2010) there were: 775 hits to the Kids Helpline Victorian Bushfire teen web site, 86 hits to the kids web site, 55 hits to the adult web site, and 28 hits to a site containing bushfire tip sheets.
MensLine Australia. During the reporting period of July 2009 to May 2010, the MensLine's bushfire service recorded 106 incoming calls, 59 outgoing calls and nine callback clients. Thirteen additional calls were received between May and June 2009.
The consumer profile was evenly balanced in terms of gender (49% male, 44% female, rest unknown) with the majority aged 35-64 years. While the origin of calls was known in less than half of the cases, 35% (n = 37) of incoming calls were received from Victoria and 9% (n = 9) from other states. A significant proportion of callers were single or separated and most lived in temporary accommodation. The majority of calls related to physical and mental health 46% (n = 35) and inter-personal problems 37% (n = 28) with other problems including parenting 9% (n = 7), legal, material, financial 5% (n = 4) and safety 3% (n = 2). Over half of the clients (54%) were reported to have medium to high levels of distress. While 57% (n = 94) of calls were classified as ‘engaged’ (i.e. involving provision of counselling, information and/or referral), a large proportion of calls (43%, n = 71) was classified as ‘non-engaged’ (i.e. involving inappropriate calls, phone messages, or callers refusing the support offered). Of the total number of calls, 39% (n = 64) related to counselling, 6% (n = 10) to counselling and referral and 4% (n = 7) to requests for information. A total of eighteen referrals were made to Counselling services (n = 8), Health services (n = 3), Housing and Accommodation (n = 2), Other services (n = 3), Drug and Alcohol services (n = 1) and Legal assistance (n = 1).
Lifeline Australia. Lifeline calls recorded between October 2008 and September 2009 were categorised by counsellors (via call sheets) as arising directly in the context of ‘Community Crisis or Disaster’. During this period, 205 calls were recorded for Victoria and 414 calls nationally, with a marked increase for both during the months of February and March 2009, see Figure 1. The timing of this peak and level of increase (accounting for nearly half of annual Victorian calls in February and another quarter of annual calls in March) suggests that this reflected the impact of the February bushfires in Victoria. However, the increase in national call volume may also have been partly due to Lifeline support provided to victims of the 2009 Queensland floods which took place at about the same time.
During February 2009 there was a slight increase for calls in relation to abuse and trauma (i.e. 6.2% vs. annual average of 3.7%) and for calls relating to adjustment and loss (5.5% vs. annual average of 4.5%). All other categories showed little temporal variation relative to the bushfires.
Interview data suggested that the first online forum provided by Lifeline immediately after the bushfires was well received by the public, whereas demand for the second forum held at the time of the anniversary was not particularly high.
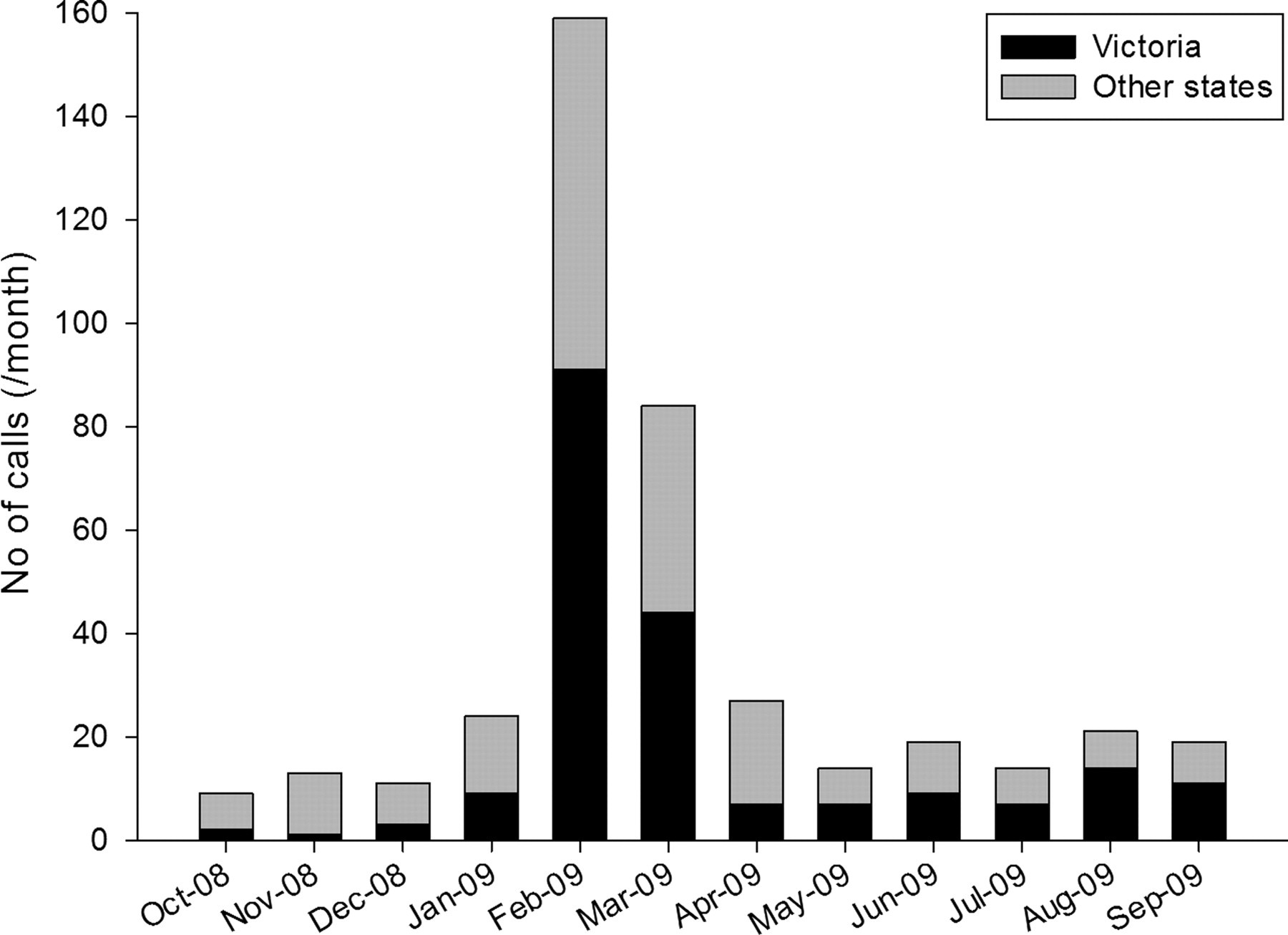
Number of Lifeline calls in relation to community crisis or disaster
Benefits and disadvantages
The benefits of telemental health services for users were identified by the key informants as: (1) availability of a free service; (2) quick response; (3) a less confrontational medium which allowed greater privacy and confidentiality; (4) widely accessible services; (5) after hours access; and (6) additional online information.
The disadvantages of services identified by key informants were specific barriers to service access, such as: (1) destroyed infrastructure, disconnected telephone lines, out of range mobile phones in rural areas; (2) high mobile phone call costs; (3) little information on wider sources of support; (4) grief, loss and helplessness; and (5) the limited suitability of the callback model for a large number of clients living in transitory circumstances.
The limited consumer data on the callback service suggested that four of the seven clients who eventually engaged in the service benefited positively from it. Data about other callback clients was inconclusive.
Data on consumer demographics and contact reasons indicated that services were accessible to broad segments of the population who were provided with support in relation to a wide range of matters. Additional information on the perspective of staff of bushfire recovery and community health centres and other agencies referring to one of the bushfire telephone services indicated that the service was perceived as helpful and conducive to recovery, and that knowledge of its existence was reassuring for agency staff and community.
Service provision
Interviews and project reports identified various matters that affected the provision of bushfire telemental health services. These were the nature of bushfire calls, the suitability of the callback model, and service coordination and data collection problems.
The nature of bushfire calls varied considerably from regular crisis calls. Bushfire calls did not appear to follow obvious patterns and were more diverse and complex than usual calls. The high levels of client distress and the complexity of the problems often made the intake calls difficult to manage and screening measures difficult to administer for counselling staff. Similarly, crisis calls were reported to be more intense, demanding and slightly longer in duration than ordinary calls to such services.
The evidence suggested that the callback service model was not ideally aligned with post-disaster community needs. Counsellors had difficulty in contacting consumers and converting intake calls into callback services. The low number and greater complexity of bushfire-service calls (amidst generic service calls) made the adoption of a new bushfire specific service model more difficult for service providers. Bushfire affected consumers, on the other hand, who were often living through rather chaotic and transitory circumstances were found to be unable to make the most of the structured callback model. Thus, resulting usage patterns indicated that the service was more readily utilised as a regular crisis service. A representative of the provider agency suggested that the concept and value of callback services was not fully understood in the wider community.
An initial lack of awareness on the part of national provider agencies of the broader bushfire response structures and locally relevant service and referral contexts had to be overcome through provider networking and active acquisition of related information. Key informants suggested that coordination and communication between Federal and State governments and provider agencies could have been stronger. A need for stronger departmental briefing and feedback mechanisms was raised by providers, as was a more systematic approach to the collection and sharing of data on service demand and uptake. This would facilitate overall response planning.
Key informants also highlighted factors which had facilitated the delivery of services in the wake of the bushfires, including: (1) using the existing platforms of reputable service providers and telephone numbers; (2) ready access to highly trained staff who were used to dealing with trauma and difficult matters, such as suicide and violence; (3) a dedicated project officer to assist agencies in liaising with services and supporting counselling staff; (4) information from external experts; (5) cross-promotion of telephone services among agencies; (6) free advertising space provided by cinemas and the media; (7) bushfire case managers facilitating referrals; and (8) high level cooperation and goodwill between all agencies involved.
Discussion
Telemedicine can provide accessible, confidential and cost-effective mental health services, 6–10 but there is very little evidence about its application in disaster contexts. Types of remotely delivered health and mental health services in disaster contexts have included information hotlines, triage and referral services, clinical consultation, crisis counselling and e-therapy. These services have been provided by telephone, email, Internet, videoconferencing and mobile satellite technology. 11–14 International initiatives have included LifeNet, a mental health information and referral hotline, 15,16 crisis counselling on the basis of Psychological First Aid, 17 both in response to the 11 September 2001 terrorist attacks in the US, and psychological assistance for victims of Hurricane Katrina. 18
The present study had certain limitations. These included the small interview sample size, variable baseline and quality of service uptake data, and a lack of data on consumer outcomes and perspectives. In addition, the economic and clinical value of the services was not measured. Despite these limitations, it appears that all three telemental health services experienced significant increases in overall service uptake levels in the wake of the bushfires. Call volume in relation to the callback service, however, remained very limited which may have partly been due to a lack of alignment of the structured callback model with transitory living circumstances in the aftermath of the disaster. Caller profiles and call characteristics further indicated that national telemental health services reached consumers from broad segments of the population (including from bushfire affected areas and to some extent other states).
Due to the existence of state-level telephone counselling and other mental health services, it is difficult to assess the relative contribution of national telemental health services as part of the overall response to the fires.
Service models
The present study suggests that callback services may not be the ideal method of telemental health service provision following a bushfire. Further education about the concept of callback services may be required in the community and among referring agencies in order to enhance service uptake.
Psychological support models underpinning mental health service provision in disaster contexts may benefit from refinement in relation to the telephone modality and complex nature of client calls. Earlier international telemental health initiatives adopted the Psychological First Aid approach 17,18 which is considered the standard of care in the immediate disaster aftermath. More recently, comprehensive stepped care models of disaster mental health service provision have specifically stipulated the benefits of offering three distinct levels of services, including Psychological First Aid (Level 1), Skills for Psychological Recovery (Level 2) and more intensive mental health treatments (Level 3) closely aligned with the varying nature of client needs presenting in the short- medium- and long-term. 19 We believe that telemental health agencies should plan to adopt such differential service models in the event of future disasters, ideally exclusive of the callback services component. Counselling staff clearly benefit from training and support relating to the adoption of new service models, as from briefings in disaster mental health which can highlight the impacts of disaster-level trauma on individuals and communities.
Public access to telemental health services in disaster circumstances can be further improved through: (a) enhancing telecommunication infrastructure (i.e., mobile phone coverage and broadband access) in rural and disaster-prone areas; (b) a stronger focus on web-based service delivery which proved useful in work with younger generations; and (c) a review of existing costing models governing mobile phone calls to disaster telemental health services.
Service coordination
Strategies to enhance service coordination and integration of national telemental health services within broader disaster response structures may include: (a) establishing a disaster response information clearing house; (b) ready provider access to response coordinators who should be familiar with relevant mental health services and disaster resources at local, state and national levels; (c) ongoing departmental briefing mechanisms and updates for provider agencies; and (d) forums in which federally-funded telemental health and relevant state-funded services can liaise and collaborate. The sharing of data between state and federal governments and the will to harness learning about emerging patterns of service demand represent important considerations in the planning of future disaster responses. The integration of disaster specific telehealth services within existing mainstream service structures can maximise their sustainability and utility for the broader population, as well as preparedness and capacity for future disaster circumstances. 11,13
Conclusion
The present study suggests that national telemental health services offered as part of the response to the Victorian bushfires provided a useful addition to existing counselling and crisis support. Structured callback models may be of limited value in the aftermath of disasters. There is a need to support counselling staff and refine existing models of service delivery. Telemental health services need to be integrated into mainstream services and disaster response structures.
Footnotes
Acknowledgements
The study was supported by funding from the Australian Government Department of Health and Ageing. We thank the Australian Government Department of Health and Ageing, the Victorian Department of Health, Kids Helpline (BoysTown), MensLine Australia (Crisis Support Services) and Lifeline Australia.