
Abstract

Chronic obstructive pulmonary disease (COPD) is a slowly progressive, irreversible and life limiting disease affecting approximately three million people in the UK, of whom only 900,000 have been diagnosed. One in eight (130,000 per year) emergency admissions to hospital in the UK is the result of an exacerbation of COPD, making it the second largest cause of acute admission, with enormous cost to the healthcare system. Exacerbations are also the most common cause of contact with health services and of death in people with COPD. The direct cost of COPD to the health care system in the UK is estimated to be £810–930 million (US$1243–1427 million) a year and this is expected to grow.
There has been considerable interest in the role that telemonitoring of COPD might play. It has been used in a number of operational settings, and the results suggest that it may be effective. For example, a trial of telemonitoring in 53 COPD patients in the UK reported a decrease in hospital admission rates of 83%. 1 However, evaluation reports such as this are often based upon small samples, adopt methodologies with substantial limitations, and do not adequately control extraneous variables.
In terms of higher quality research findings, the evidence base for telemonitoring in COPD is less mature than that of chronic heart failure (CHF). Three recent reviews 2–4 have concluded that although there appear to be benefits from telemonitoring patients with COPD, limitations in the published research make definitive conclusions hard to reach. The reviews suggest that telemonitoring can have a positive effect on quality of life and patient satisfaction. In addition, they suggest that home telemonitoring in COPD could reduce emergency department visits and hospital admissions, although there did not appear to be any significant effect on mortality. It is believed that telemonitoring, whilst costly to set up, will reduce costs in the long term. 2 It has been suggested that in-hospital stay can be reduced by up to 50%. In COPD, telemonitoring is claimed to have the potential for national savings of £63 million (US$97 million). 5
Despite these superficially promising results, all reviewers advise caution. There is substantial clinical heterogeneity in the trials, many studies are small scale, and researchers are unable to blind participants to interventions. Crucially, telemonitoring is often introduced as part of a complex care package, so it is difficult to identify the independent benefits brought by remote monitoring. In addition, the telemonitoring intervention itself varies from study to study in terms of, for example, methods of data transfer (e.g. automated or via the telephone), the presence or absence of an educational component added to monitoring, and the vital signs measured as part of the intervention.
The conclusion of all reviews is that further research is required to identify the best delivery mechanism for telemonitoring in COPD and establish the true level of benefits.
One reason why it has been difficult to identify the true effectiveness of telemonitoring in COPD is that the mechanism by which benefits might be gained is unknown. It may be that monitoring of signs, symptoms and physiological indicators such as oxygen saturation might give early warning of exacerbations and allow prompt intervention. Such monitoring may also enhance patients' understanding of their condition, thereby promoting self-care, or it may simply have a reassuring and quasi-placebo effect. The mechanism of action is further complicated by a lack of clarity about what should be monitored. In CHF, there is a strong argument for trend monitoring in relation to bodyweight, blood pressure and pulse rate. Current monitoring of COPD patients routinely includes pulse rate, blood pressure, oximetry and qualitative question trees. Ostensibly, oximetry would seem to be the most attractive indicator of deteriorating COPD, but in practice this is not a reliable sign of exacerbation.
Patients with COPD most frequently complain of breathlessness and cough which is increased during exacerbations. In the UK, the National Institute for Health and Clinical Excellence (NICE) defines an exacerbation of COPD as an increase in breathlessness, cough and sputum production. COPD exacerbation and hospital admission are associated with poor outcomes. The two-year mortality rate among these patients is increased significantly to 49%. A further problem with exacerbations is that patients have a tendency to under-report them. Under-reporting of exacerbations has been seen to have an effect on health status. Patients exacerbating are significantly more breathless and more likely to report cough than healthy patients, but do not differ in baseline spirometry. Cough has the greatest predictive value for subsequent hospital admission due to respiratory disease in general and COPD in particular. 6,7
Although cough can be monitored without subjective bias, passively and continuously, there are problems. 8 Due to the episodic and paroxysmal nature of cough, recording over a prolonged period of time is required. Hence the aural analysis of these recordings requires an equally long time. Excluding background noise and other respiratory noises has always proved difficult as has counting the peal (paroxysm) of cough. Automatic systems suffer from the disadvantage of being less accurate than the human ear in differentiating cough. 8 In addition there is no universally accepted definition of what constitutes a cough for counting purposes. The problems of definition primarily arise in relation to counting a peal of coughs. The acoustic signal of cough varies enormously with differences in gender, age, and whether there is sputum production or not. Studies have shown poor correlation between subjective and objective assessment of cough.
We conducted a two-week pilot study on a 78-year old male with severe COPD and a smoking history of at least 60 years. He was receiving optimum medical therapy but did not require long-term oxygen. He lived with his partner in a small house (bedroom not shared). Two recording devices were used; a small hard drive recorder with a free-field microphone and a recording capacity of three days, and a laptop computer, also with a free-field microphone. The hard drive recorder was placed in the living room and the laptop recorder in the bedroom with the microphone approximately 1 metre from the bed. Both rooms were small. The computer was closed and shut with secure tape. Ethics approval was not required.
The system used did not allow real-time or store-and-forward telemonitoring of data. Instead, the recorder and laptop were removed after the deployment period, and the data analysed retrospectively. During the recording period the subject noted more symptoms than usual in his diary record, with increased cough and sputum, but did not suffer exacerbation or require any change in medication.
The pilot study found that the system produced a recording of sufficiently good quality for cough counting purposes (Figure 1). The cough signal had greater amplitude than speech or background noise.
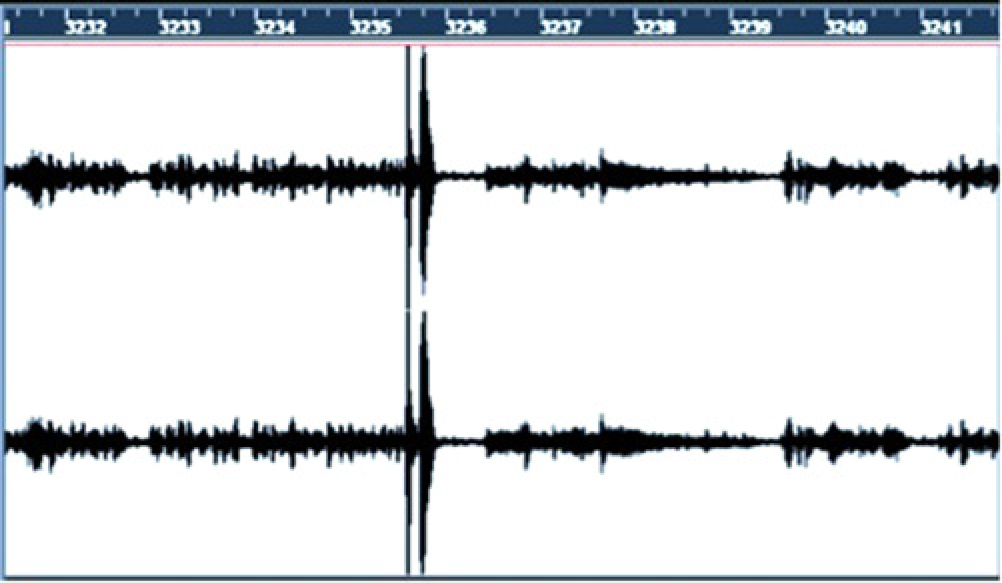
Acoustic signal of cough on background noise
Several problems were encountered. Some sections of the recording, approximately 5% of the total, were unusable due to high levels of environmental noise. Respiratory noises other than cough caused confusion at times and as the subject lived with a partner, her cough was also recorded although this was assumed to be negligible and not to introduce significant bias. Nevertheless, the recording was of sufficient quality to identify, characterise and cough count. The data were analysed using a trained Gaussian Mixture Model of the spectral features, tonality, rhythm and percussiveness and found to be of sufficient quality to identify and quantify cough.
We conclude that the use of free-field microphones in the patient's own home offers a possible method of capturing cough data reliably. We therefore propose that remote cough measurement should be further tested to confirm whether it is technically feasible, acceptable to patients and associated with clinical benefit. Further work is also required on data transmission to identify appropriate real-time communication. To this end we have embarked on a larger study using the techniques described above.