
Abstract
Objectives
In healthy postmenopausal women (PMW) increased platelet activation has been associated with adverse cardiovascular events. There is much debate about the relationship between platelet function and serum estradiol level in PMW. This study assessed the effect of short-term oral estrogen replacement therapy (ERT) on platelet activation markers (CD62P and PAC-1) and its correlation with age and body mass index (BMI) among healthy PMW.
Methods
A prospective intervention study was conducted at Hospital University Sains Malaysia, involving 48 healthy PMW who were evaluated for platelet activation marker levels as determined by flow cytometry, before and after two weeks of oral ERT with 0.625 mg of conjugated equine estrogen once daily. The pre- and post-ERT platelets activation markers difference was analysed by paired t-test.
Results
The pre-ERT, mean ± SD percentage levels of CD62P and PAC-1 were significantly reduced from 7.00 ± 5.91 and 41.75 ± 26.85 to 3.05 ± 2.47 and 20.86 ± 19.02, respectively, after two weeks of ERT (P value < 0.001). The correlation of platelet activation markers was significant with estradiol but not with age and BMI.
Conclusion
Short-term ERT leads to reduction in platelet activity, which might contribute to protection against cardiovascular diseases in healthy PMW.
Introduction
Platelets play a pivotal role in the formation of thrombus and hence in cardiovascular events secondary to this complication. Adverse thrombotic cardiovascular events increase after the menopause, which may be related to metabolic and hormonal changes. 1 Coronary heart disease is the leading cause of morbidity and mortality among postmenopausal women (PMW). 2 A study has suggested that estrogen plays a protective role against atherosclerosis. 3 Others have demonstrated that estrogen is able to prevent thrombogensis; mediating cardiovascular protection 4 and estrogen deficiency has a widespread impact on the cardiovascular system with a direct harmful effect on vessel-wall physiology and platelets. 5 On the other hand, epidemiological studies have reported increased relative risk of venous thrombogenesis and pulmonary embolisms in PMW who have taken hormone replacement therapy (HRT). 6,7
Increased platelet activation has been reported to be associated with unstable angina, stroke, deep vein thrombosis, acute myocardial infarction and trauma. 8 Decrease in estrogen level is related to increased platelet activation. 9 Estrogen has a direct effect on the endothelial production of nitric oxide and prostacyclin, 10 both being potent vasorelaxants, inhibiting platelet aggregation and adhesion.
By using monoclonal antibodies with flow cytometry, it is possible to determine the activation state of platelets. 9 At molecular level there was a need for a study to determine the effects of estrogen replacement therapy (ERT) on platelet activation markers, CD62P and PAC1, among Malaysian women. We were not able to find any study which has investigated this issue in the Malaysian women. This study was therefore conducted (i) to assess the effect of ERT on the platelet activation markers (CD62P and PAC-1) among healthy postmenopausal Malaysian women and (ii) to study the correlation of these markers with estradiol level, age and body mass index (BMI) of the study population.
Materials and methods
Setting
The study was conducted at Hospital Universiti Sains Malaysia (HUSM), situated in Kelantan, a state positioned in the north-east of Peninsular Malaysia and bordered by Thailand to the north. HUSM is a tertiary care centre and is regarded as a referral health facility for the east coast region of Malaysia. A prospective intervention study was carried out from January to December 2008 to determine the percentage differences in the expressions of platelet activation markers in healthy PMW before and after taking ERT for two weeks. Ethical approval was obtained from the Research and Ethics committee of HUSM.
Study population recruitment
PMW attending the postmenopausal, family medicine and staff clinics at the study hospital were invited to participate in the study. Women aged 45 to 70 years with natural menopause (12 consecutive months of amenorrhea and serum estradiol level <150 pmol/L) or surgical menopause (both follicle-stimulating hormone [FSH] and luteinizing hormone [LH] levels ≥40 mIU/mL), normal liver and renal function tests, normal lipid profile [cholesterol ≤6.3 mmol/L], non-smokers, not on HRT for the preceding three months or on non-steroidal anti-inflammatory drugs or aspirin or any other antiplatelet drugs for the preceding two weeks, and not having any acute illness during the recruitment period were eligible to participate. Those with hypertension (>140/90 mmHg), hyperglycaemia (fasting blood glucose >99 mg), previous history of thromboembolic phenomenon or stroke were excluded from the study. Informed written consent was obtained from the participants after giving them written and verbal information about the study. They were screened for eligibility based on the information obtained from their physical examination, medical records and laboratory results. Participants whose relevant laboratory results were not available were given appointment and were advised to fast in the morning of appointment date. Information about their eligibility was conveyed to such participants on telephone, after receiving the laboratory reports. Participants who were on some medication but otherwise eligible were advised on the optimum wash out period before joining the study.
Of 72 subjects who responded to the invitation and were initially registered, three did not turn up for the screening appointment and 19 were excluded; nine had hypercholesterolemia, seven had hyperglycemia, and three had premenopausal levels of FSH, LH and estradiol defined for surgical menopause. The 50 eligible women were informed that there would be two visits two weeks apart and were advised not to do strenuous exercise in the morning of the appointment date, as strenuous exercise may activate the platelets. 11 Two of them were lost to follow-up at second visit, thus 48 participants completed the study (Figure 1).
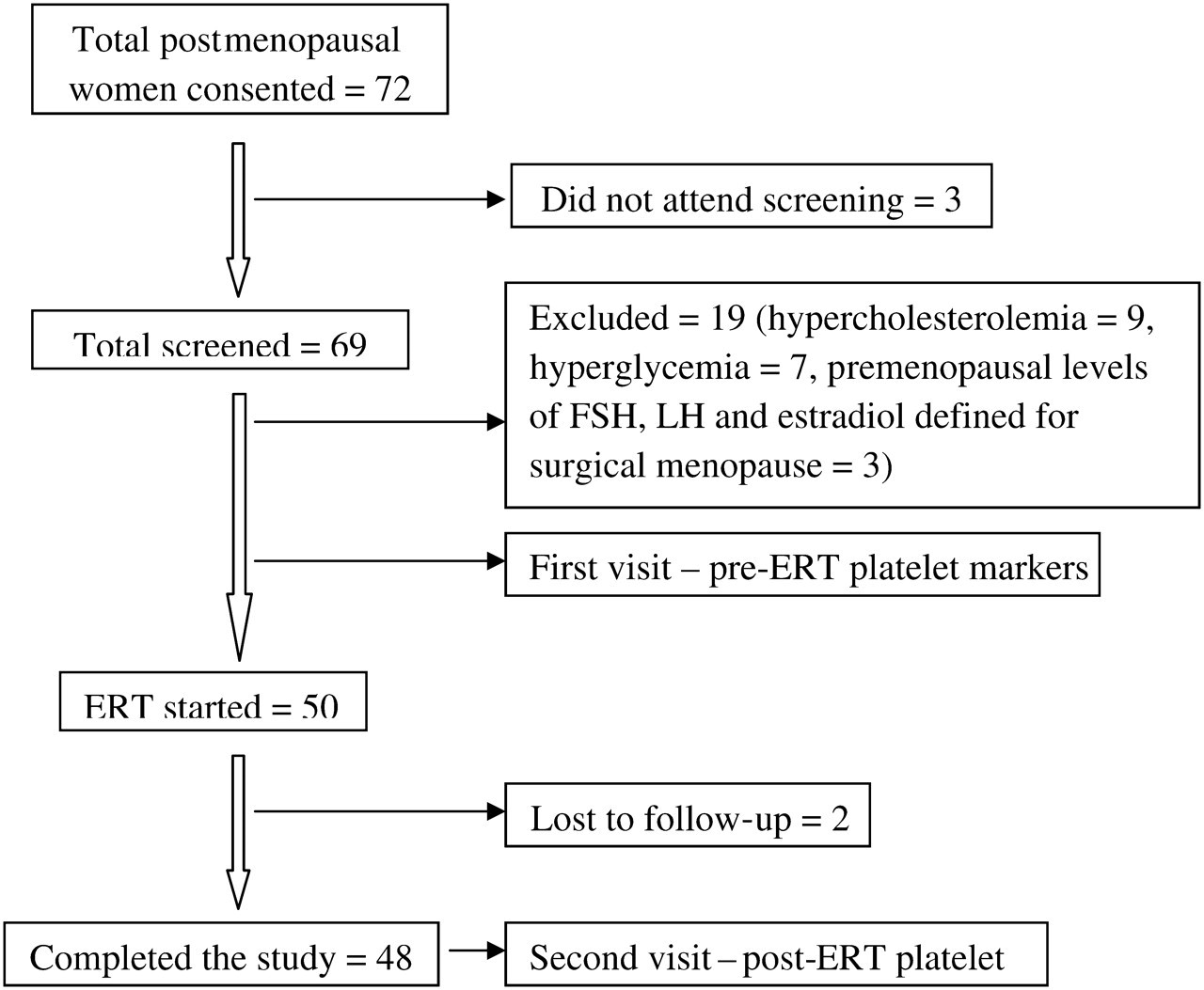
Flow chart for the short term estrogen replacement therapy study in Malaysian postmenopausal women FSH = follicle-stimulating hormone; LH = luteinizing hormone; ERT = estrogen replacement therapy
Blood collection
On each visit, the participants were asked to rest for 10 minutes so as to attain basal body conditions before taking blood. In order to prevent artificial activation of platelets, no tourniquet was used. 12 A butterfly cannula was inserted into the ante-cubital vein to collect 2 mL of blood for the analysis of platelet activation markers (CD62P and PAC-1) and 3.8% sodium citrate was used as an anticoagulant.
ERT intervention regimen
The eligible women were prescribed oral ERT for two weeks duration (conjugated equine estrogen [CEE] 0.625 mg once daily) after taking blood from them on their first visit, and were asked to return back after two weeks for second collection of blood.
Flow cytometry and monoclonal antibodies used
Becton Dickinson flow cytometer (San Jose, CA, USA) was used for flow cytometry. Staining of the blood samples were done within 10 minutes of sample collection. Two activation-dependent monoclonal antibodies, anti-CD62P and anti-GP-IIb/IIIa (anti-PAC-1), were used to detect platelet activation. Flow cytometry was performed and positive events were acquired for platelets. Ten thousand activation independent events were acquired for each sample. Dot plots and quadrant statistics were used to calculate the percentage of positive activation markers. Reference values used for the percentage expression of CD62P were 0.0–3.8% and of PAC1 were 0.25–9.75% at the resting state. 13 Thus the values of >3.8% and >9.75% were considered as raised CD62P and PAC1 levels, respectively.
Sample size calculation
In order to detect a true difference of 1%, with a standard deviation of 1.9 reported previously, 9 in the mean levels of platelet activation markers between pre- and post-ERT PMW, at significance level of 5% and with power of 90%, we needed to study 40 pairs of subjects. We were able to recruit 48 pairs.
Statistical analysis
SPSS (statistical package for social sciences version 12.0.1) was used for data entry and analysis. Descriptive statistics such as means and their standard deviations (SDs) were calculated for continuous variables – serum estradiol, age, BMI, CD62P and PAC-1 – while frequencies (%) were calculated when the variables were used as categorical. The pre- and post-ERT mean of platelet activation markers (CD62P and PAC-1) was compared by paired t-test. The correlation of platelet activation markers with serum estradiol, BMI and age at the pre-ERT condition was determined by Pearson correlation analysis. P value of less than 0.05 was considered to be significant.
Results
The mean (SD) age, BMI and serum estradiol level of the participants in the current study at baseline (pre-ERT) was 53.9 (5.57) years, 27.19 (4.12) kg/m2 and 57.40 (37.57) pmol/L, respectively. There was 41.7% and 20.9% reduction in the number of women with raised platelet activation for CD62P marker and PAC1 marker, respectively, after taking ERT for two weeks (Table 1).
Percentage expression of platelet activation markers (CD62P and PAC-1) among postmenopausal women pre- and post-ERT in Malaysia in 2008 as assessed in an intervention study (n = 48)
ERT = estrogen replacement therapy
*Platelet activation state (normal range: CD62P: 0.0–3.8%, PAC-1: 0.25%–9.75%)
The paired t-test analysis revealed that both the mean CD62P and mean PAC-1 marker levels were significantly different before and after two weeks of ERT (P value <0.001) (Table 2). Pearson's correlation analysis showed that with increase in serum estradiol there was decrease in CD62P marker (r = −0.34, P value = 0.02), as well as in PAC-1 marker (r = −0.30, P value = 0.04). However, there was no relationship of these markers with BMI and age of the PMW (Table 3).
Comparison between pre- and post-ERT platelet activation markers (CD62P and PAC-1) in postmenopausal women in Malaysia as assessed in an intervention study, 2008 (n=48)
ERT = estrogen replacement therapy; CI = confidence interval
Correlation of age, BMI, and serum estradiol with platelet activation markers (CD62P and PAC-1) in postmenopausal women in Malaysia as assessed in an ERT intervention study, 2008 (n=48)
BMI = body mass index; ERT = estrogen replacement therapy
Discussion
The assessment of inappropriate platelet activity in vivo is one of the ways to risk-stratify those who are at risk of arterial thrombosis. Until recently, platelet aggregometry was regarded as the gold standard for platelet function but with the availability of sensitive techniques like flow cytometry, reliable results can be obtained.
In the present study, we report the effect of short-term oral ERT on platelet activation markers in healthy PMW. We found an increased platelet activation in PMW which decreased after HRT administration, supporting previous findings. 14 Estrogen improves the lipid profiles, reduces atherosclerotic plaque formation, 15 increases nitric oxide production in many tissues 16 leading to reduction in platelet adhesion, aggregation and activity of platelet-activating factor acetyl-hydrolase in PMW. 17
Our study showed a significant reduction in expressions of platelet activation markers (CD62P and PAC1) in PMW after taking short-term ERT. The increased platelet activation markers in the women prior to ERT may correlate with the frequent thromboembolic events and may suggest a role of platelets activation in an increased incidence of cardiovascular disease in this population. This favourable effect of short-term ERT on platelet activation markers is an interesting finding and it can be hypothesized that longer ERT may further reduce the platelet activation markers level.
We used CEE because it has been reported that some of the beneficial effects of estrogen may be attenuated by the concurrent administration of progesterone. 18 The maximum platelet half-life is reported to be 9–11 days using in vitro labelling with chromium-51. To avoid any experimental bias, we administered the HRT for a period of two weeks which cover the life span of platelets reported previously by different authors, the maximum being 9–11 days. 19
For the analysis of platelet activation, two principal assays can be used, enzyme-linked immunosorbent assay (ELISA) and flow-cytometry. We chose the later because it needs lesser volume of blood sample as well as it is a more sensitive technique that allows seeing changes in individual platelets, thus yielding more accurate and reliable results. In contrast, ELISA is mostly used to measure the metabolites of activated platelets in the plasma or urine. 20 There are many platelet activation markers but we chose only CD62P and PAC-1 because their expression on platelet surface is characteristic of platelet activation. Similarly, in the literature many different monoclonal antibodies are mentioned and we choose only anti-CD62P and anti-GP-IIb/IIIa (anti-PAC-1) which bind specifically to these platelet activation markers. It has been suggested that CD62P might reflect platelet activation in response to acute stimuli, while PAC-1 is a better marker in detecting circulating activated platelets in clinical settings where more ‘chronic’ stimuli are present. 21
In the present study, a significant negative correlation was detected between serum estradiol and platelet activation markers (CD62P and PAC1) in PMW showing the beneficial effects of estradiol on platelet activation reduction. However, no significant correlation was observed between age and these platelet activation markers and this finding is consistent with a study 22 which reported that advanced age is associated with elevated interleukin-6 and C-reactive protein levels, indicating an inflammatory state that may be another possibility for thromboembolic disease in the elderly.
There was also no significant correlation between BMI and platelet activation markers and these results are contrasting to those of Basili et al., 23 who concluded in their study that insulin resistance contributes to increased platelet activation in obesity. These contrasting results might be explained on the basis of different range of BMI because they included only patients with BMI >30 kg/m2. 23 A study by Samocha-Bonet and colleagues, 24 the results of which are quite similar to our study, reported that flow cytometric analysis of platelets showed no significant differences in activation marker expression between non-obese and obese individuals. 24
Until now, the results of observational and randomized clinical trial studies, which examined the effects of HRT on platelet function and risk of cardiovascular events, are conflicting. Discrepancies found in estrogen action may be attributed to the variable methodologies adopted by different investigators including type of platelet preparation analysed (washed platelets or platelet-rich plasma), concentration of estrogens used and length of platelets exposure to estrogens, and other sociodemographic and clinical characteristics of study population. 25 Moreover, differences in route of administration, dose, type, duration of use, starting time of HRT (early or late menopause) and measurement of in vitro incubation of hormones versus in vivo effects of oral hormonal therapy on platelet function also account for conflicting results. In our study, we examined in vivo effects of oral ERT on platelet function by measuring platelet activation markers.
Limitations
The present study design did not permit us to draw strong conclusion about the short-term (2 weeks) ERT effect on platelet activation markers in the absence of placebo arm. Furthermore, long-term ERT and follow-up was out of the scope of this study due to logistical constraints.
Conclusion and recommendations
Platelet activation level was found to be raised in healthy PMW. In majority of women, it was converted into resting state level when they were given two weeks estrogen-alone HRT. Such decrease in platelet activation level might contribute to protection against cardiovascular diseases in healthy PMW. Considering our results as ‘pre-event’ data, we recommend a follow-up study based on PMW's exposure to ERT, to demonstrate the long-term favourable and adverse outcomes of this type of hormonal replacement therapy. However, using estrogen when not hysterectomized is appropriate for short-term use only. Moreover, there is need for research to look at effect of adding in progestrogen onto the current findings.