
Abstract
Five types of elder abuse (physical, psychological, sexual, neglect and financial) are recognized. They are not new, occur worldwide and are associated with persistent morbidity and mortality. The forensic clinician has responsibilities to: (i) the patient, with competent history taking and examination, (ii) interpret findings and recognize patterns of harm and (iii) promulgate this issue in wider professional and public forums. Research into elder abuse is relatively recent; standardized terminology remains unsettled, and small-scale, local studies are hard to generalize. Cross-sectional, population-based studies of elder abuse should be possible, and standardized endpoints will require forensic science contributions.
Introduction
Goosey Goosey Gander, whither shall I wander?
Upstairs, downstairs and in my lady's chamber.
There I met an old man who wouldn't say his prayers,
So I took him by the left leg and threw him down the stairs.
– Anonymous, 17th century
The old man may have been victimized for a number of reasons: inability or unwillingness to co-operate with his carers (‘wouldn't say his prayers’), or political or religious bias by the victimizer against his easy victim (colloquially, to ‘gander’ is to inspect, and the Roundheads are said to have ‘goose-stepped’). In the 17th century, the protestant and Roman Catholic prayer books were in competition. 1 A further speculation is that the old man might have been a recusant priest in hiding. Regardless, there was a violent response, and elder abuse is not a new phenomenon.
Elders possess the same human rights as everyone else. Abuse of those rights, especially those aspects to which clinical forensic medicine can contribute, is the theme of this review. Moreover, in spite of their different ages, the intrinsic features of vulnerability leads to numerous parallels between abuse of elders and children, as seen below, and we should not forget that vulnerable people have deserved aspirations that go beyond mere respect for their rights. 2
Terminology and evidence base
Elder abuse is a relatively new research field in comparison with, say, the issue of child abuse. Due to this youth, standardized terminology is yet to emerge; but, aiming for a consensus, the following definitions are used below:
Abuse: an improper action committed by one person and directed to another; there may be tangible or intangible gain for the abuser (e.g. satisfaction of sense of retribution, avoidance of effort, monetary gain, etc.); Elder: due to his/her advanced age, a person who is vulnerable in comparison with younger adults in the same community. No precise age limit is implied; Elder abuse: abuse directed at an elder by a person with a responsibility for care;
3
Neglect: omission of care deserved by an elder; neglect can be by a person or organization and due to medical, legal, professional or moral responsibility for the elder; Negligence: a cause of action at civil law with a standard legal definition and massive literature. Civil negligence (briefly) must comprise that the transgressor: (i) has (or had) a duty of care, and (ii) neglected that duty, that (iii) neglect of that duty caused identifiable harm to some person, and (iv) that monetary compensation for the harm can be assessed. In some jurisdictions, there is also criminal negligence, where the harm is conceived to have been sustained by society as a whole, and monetary compensation is irrelevant for conviction. The same act(s) of negligence can be both civil and criminal;
4
Self-neglect: neglect by a capable person leading to harm to him/herself.
The term ‘forensic clinician’ is used below without any intent to imply that the issues raised should be reserved for the forensic medicine specialist. All medical specialties overlap. Elder abuse may present to many types of clinicians, including general practitioners, emergency and accident officers, district nurses, health visitors, orthopaedic surgeons, psychiatrists and psychologists. If progress in detection, research and prevention of elder abuse is to be made then encouraging all these other specialists to include a forensic aspect to their practices is sine qua non.
The evidence base for elder abuse is sparse. Sidney Stahl, a senior member of the United States National Institute on Aging (NIA) felt able to say in 2002 that:
‘Elder abuse is probably where child abuse was 30 or 40 years ago, which is nowhere.’
5
The PubMed® database confirms this view. The earliest case report is probably a letter to the British Medical Journal that used the term ‘granny-battering’.
6
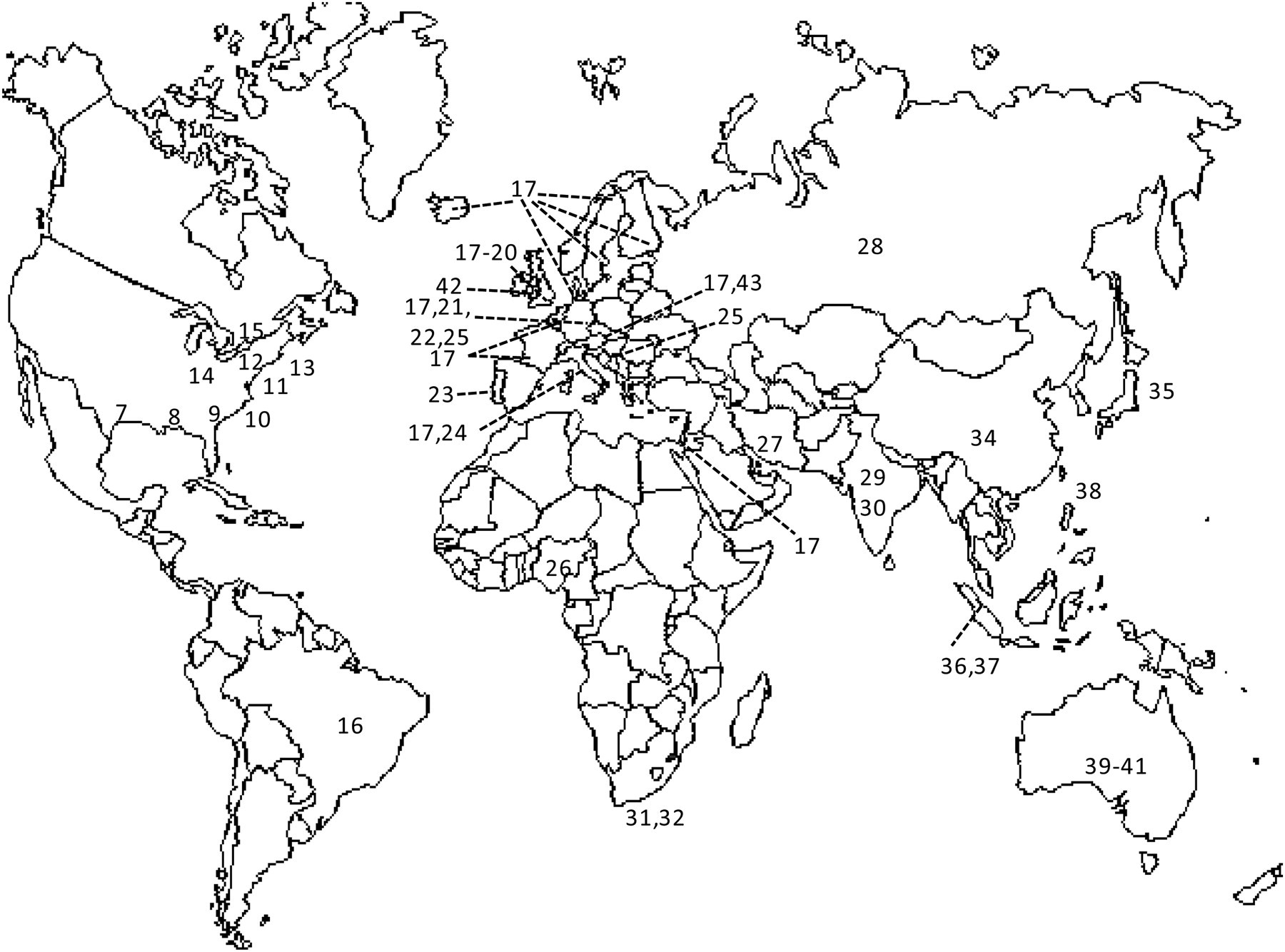
Using the terms ‘elder abuse’ and ‘elderly abuse’, Figure 1 shows that while the number of publications is increasing, it still compares poorly with the literature on child abuse (768 citations January–November 2011), or heart failure (thousands of publications each year). And yet, sparse as this literature may be, it has a worldwide distribution (Figure 2).
7–41
Date of publication and number of publications in the PubMed database, when searched using the two terms ‘elder abuse’ or ‘elderly abuse’. Word order within these terms does not alter the search yield. The part-year total January–November 2011 was 67 publications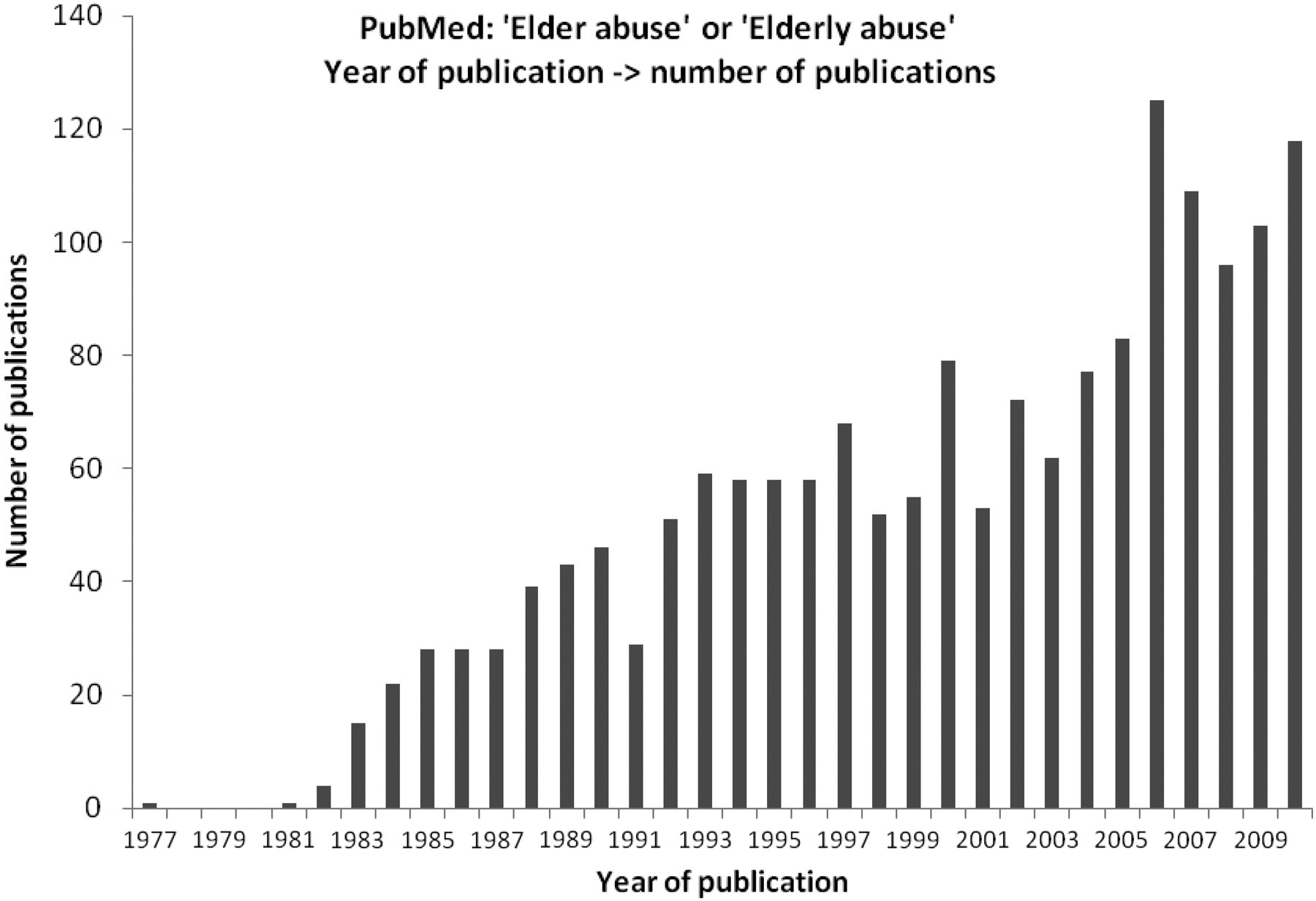
Epidemiology
While elder abuse exists worldwide (Figure 2), quantitating it is more difficult. Population-based studies of elder abuse should be possible, but have been conducted only rarely.
42
The form of abuse can usually be categorized into one or more of the following components:
3,10,43–45
Physical abuse; Sexual abuse; Psychological abuse; Neglect; Financial abuse.
The first four of these are most likely to come to the attention of the forensic clinician. Financial abuse is probably more likely to present to a lawyer than a medical practitioner, although there is at least one report of it from a psychiatrist
45
and such cases often include psychological complications. ‘Pharmacological abuse’ can be defined as drug-induced restraint, with both physical and psychological components.
Many studies recite the reasons why the scale of the problem is unknown. These include reticence of reporting, absence of suspicion on the part of clinicians, difficulties in obtaining a history from patients with dementia, ambiguous clinical signs, denial by carers, disagreements about where the border of abuse lies (e.g. restraint may be for a patient's benefit as well as a form of abuse), and the absence of standardized terminology and measurements among the research community. 3,46,47 Thus, prevalence estimates of elder abuse range from 4% to 25%. 10,19,20,48 Remarkably, one study in a respite care environment in Putney and Barnes (near London, UK) elicited few complaints of abuse from the patients, but anonymous admissions of abuse from 45% of their carers. 18
Mortality
Beyond physical and psychological morbidity associated with abuse (see below), there is clear evidence that elder abuse is associated with mortality. For example, in New Haven, Connecticut, a prospective comparison was made between 176 patients with verified allegations of physical abuse and a control cohort (n = 2812) of persons. 49 All-cause mortality was the endpoint. After 8–13 years of follow-up, the odds ratio for survival was 3:1 (95% confidence interval [CI] 1.4–6.7) favouring the controls; the single largest subgroup with abuse-associated mortality hazard was those with supposed ‘natural causes’ of death due to circulatory disease. More recently, this was confirmed in Chicago, IL, USA. 50 A study similar, in design, to that in Connecticut found a one-year mortality hazard ratio of 5.85 (95% CI 5.20–6.51) associated with elder abuse or self-neglect. Lastly, the relationship between elder abuse and suicide is unexplored, in spite of calls for research dating back to 1995. 51
Recognition of elder abuse
The task of the forensic clinician (regardless of his/her ostensible specialty) is to take a history and examine the patient, with a view to determine whether there is a need for:
Carers to change their behaviour, or formal evidence that abuse is taking place for legal proceedings.
Elders may not provide good histories, dependent upon the degree of dementia. But it is also precisely that complication of old age that might bring an elder into the ambit of an abusive carer. If a history from a potential victim can be taken, then it should be taken separately from that of other possible victims. Interviewing the carer who is under suspicion is also important, and this should be objective; presumptions of ‘guilt or innocence’ should not be developed before conducting such interviews.
Physical stigmata of elder abuse
The Istanbul Protocol [sect. V, para 186 (a)–(e)]
Compared with younger age groups, the skin and subcutaneous tissues of the elderly are usually more fragile. Bruises and lacerations are made with less force than in younger patients and take longer to heal.
55
While ageing a bruise is notoriously difficult under any circumstances,
56
it may be easier to judge whether multiple lesions were acquired at different times.
55
A pattern of repetitive injury is always suspicious (as in children; see Figure 3).
Right posterior forearm of an 81-year-old white female patient in an assisted-care home with (a) irregular, non-linear lacerations associated with bleeding fresh enough not to have formed a scab, (b) scattered ellipsoid bruises of apparently differing ages and (c) two bruises which are straight and tram-lined (arrows), suggesting forcible contact by a cylindrical object, again appearing to be of different ages. The lacerations nearest the wrist (arrowheads) may be an extension of the newer tram-lined lesion, indicating a bulbous end to a weapon, thus being consistent with a defensive wound. Source: 
Soft tissue injuries in the elderly can, of course, also be purely accidental. However, for example, while falls may be accidental, they can also be the result of neglect, if not of physical abuse. Figure 4 shows an example.
This 79-year-old white woman was found on the floor between a couch and a radiator, and brought to the Boston Medical Center (Massachusetts) Emergency Room. As per a relative, there was no history of anticoagulant use, but no history of the type or timing of the trauma could be obtained. Burns, bruises and lacerations were documented. Initially suspected as an example of physical abuse, the blood alcohol concentration then was reported as 138 mg/dL. Neglect could not be excluded, and the patient was referred to protective services. Source: 
Fractures are more common in the elderly than in younger patients due to osteoporosis. As in children, multiple fractures of differing ages should raise the suspicion of abuse. 55 However, unlike younger patients, the elderly also sustain spontaneous vertebral and hip fractures, and prior bisphosphonate therapy is associated with spontaneous fractures of the infra-trochanteric femur. 57,58
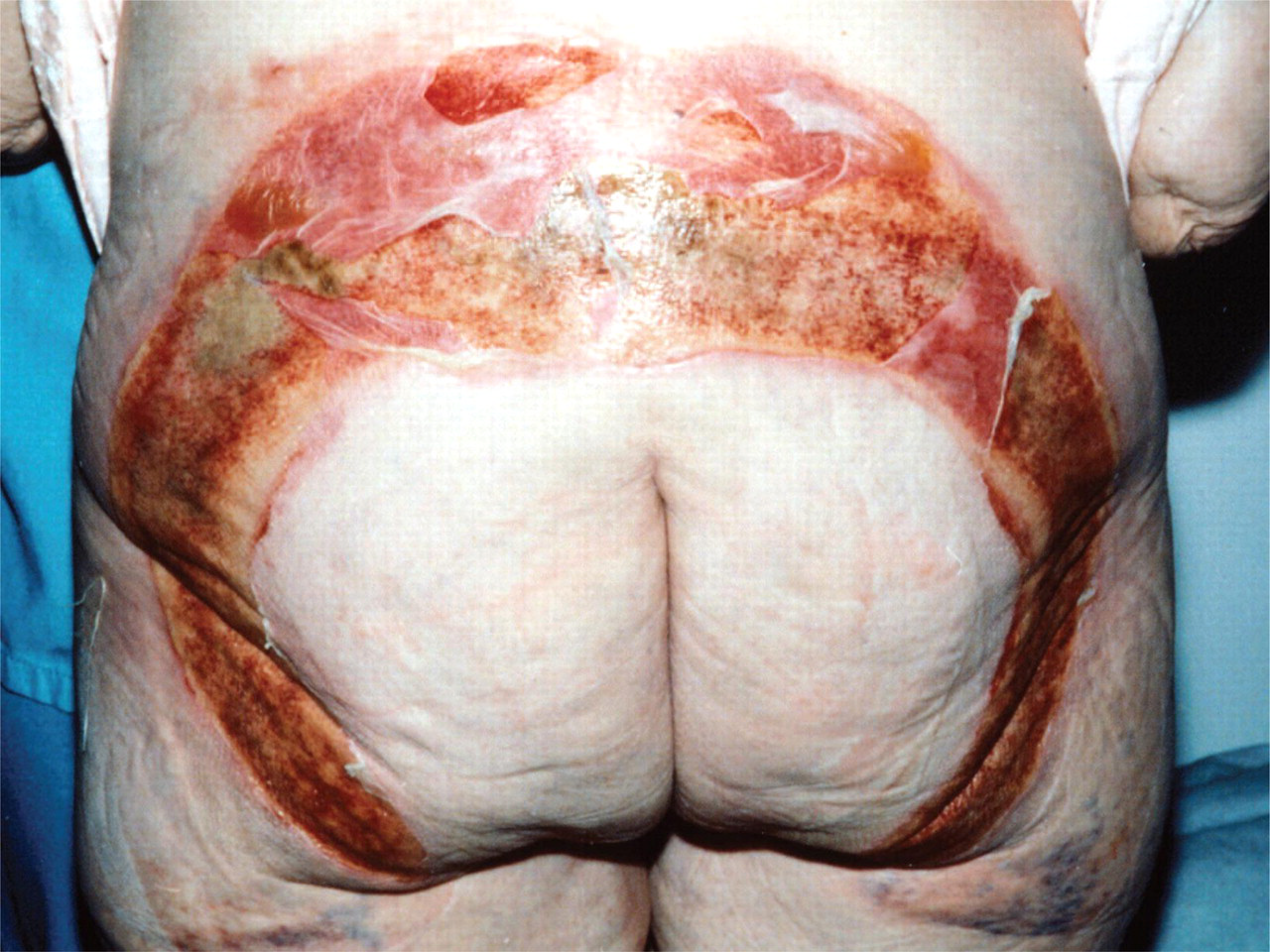
Burns are inflicted on elders either by acts of commission or omission, just as they are in children (see Figure 5).
59
,60
Cigarette burns in the elderly have an appearance that is similar to those in other age groups, although full-thickness burns may be inflicted in less than one second in patients with dermal atrophy, unlike in younger patients. Again as in children, cigarette burns in locations that are anatomically improbable for self-inflicted injury are strong indications for forensic investigation of elder abuse.
61
An elderly woman who, ‘due to negligent supervision’, was unable to get out of a bath that was too hot. This ‘halo pattern’ has outer margins corresponding to water depth in the sitting position and a spared central area that was in close apposition to the bottom of the bath, thus excluding the scalding water.
60
Similar lesions are seen in abused children. Figure courtesy of Greenbaum et al., 2006
60
Decubitus ulcers are usually a sign of neglect or self-neglect. The common sites are elbows, sacrum and buttocks due to prolonged immobility in the recumbent position. When the ulcer is well-developed, necrotic or foul-smelling, and has not been brought to the attention of outside medical professionals, then suspicion of neglect should be extreme. 55
Poor hygiene, malnutrition and dehydration are common in the elderly, and are due not only to declining mobility, but also obtunded senses of taste, smell, hunger and thirst. 55 Mere failure to visit at appropriate intervals is a form of neglect that leads to these forms of harm. Rarely, entomological evidence can be used to prove that fatalities have not been visited according to schedule. 21 Good carers are aware of this, do not rely on spontaneous eating reports, and regularly weigh their patients.
Unnecessary restraints can be associated with morbidity and mortality. This has to be balanced against the need to prevent serious harm and the unsuitability of other means (e.g. drugs) to achieve the same goal. 62,63
Unusual injuries should always trigger investigation into whether elder abuse has taken place. Case studies include manubrio-clavicular dislocation in an 83-year-old man, and takotsubo syndrome following abuse in a 76-year-old woman. 23,64 But unusual injuries can also mimic abuse. One example was a 94-year-old man with a history of dementia and an accidental fall. At postmortem, there were external signs of neck trauma (bruising and a haematoma). However, careful dissection revealed a vertebral artery laceration, secondary to a fractured fifth cervical vertebral body, and no skin, strap muscle or cartilaginous injury. 65
Accident logs
Good carers maintain detailed incident logs. These should be reviewed in conjunction with history and examination of those involved. As in any other health and safety investigation, if patterns and causes can be identified, then measures for prevention can be designed. Good forensic clinicians as well as carers themselves document stress, anxiety and delusional behaviours in the elderly, together with their accident logs.
Dejection, depression, vulnerability and risk of abuse doubtlessly co-exist in many elderly patients. In the clinical situation, assigning one or other as the primary aetiology can be foolhardy. Psychological elder abuse is also often inseparable from physical abuse because the latter can cause the former in the elderly, as in other age groups (for example, this is one intent of the torturer). Psychological abuse of the elderly has the complexity that its detection requires analysis of the behaviour of two parties: the abuser and the abused. Validated scales have been used in one of the few cross-sectional studies of care-givers (n = 114 in Taiwan); care-givers who were young, less educated, and with less specific training in elderly care had a tendency towards more abusive behaviour. 38
A more precise Australian study, again using validated scales, has shown that out of the three domains, coercion, vulnerability and dejection, it was only the last that independently predicted decline in mental health, and risk for abuse. 39 A more nuanced, international study, using well-validated questionnaires, found that greater degrees of cognitive impairment, depression and delusions predicted screening positive for elder abuse among 3881 European patients. 17 From a behavioural perspective, it has also been shown that socially inappropriate, or active resistance of care behaviours by elders are predictive of abuse in the residential setting, although mere unauthorized wandering is not. 24
Sexual abuse of the elderly
If the elderly have the same human rights as everyone else, then expression of sexuality, even in the presence of dementia, may be viewed as one of those rights. Finding the balance between protecting such rights and preventing sexual abuse is a complicated question in the elderly population because hypersexuality can be a feature of disinhibition associated with dementia. 66–68
The manner of sexual abuse does not fundamentally differ between the elderly and other age groups. For example, rape, exhibitionism and ‘fisting’ by sexual predators have all been described as forms of elder abuse. 12,69,70 In the environment of long-term care facilities, sexual abuse or aggression is most commonly perpetrated by one elder resident upon another, and is termed as resident-to-resident sexual aggression (RRSA), with a high potential for physical or psychological injury. 12 Detection of sexual abuse or RRSA by forensic clinicians will often include history taking from witnesses, perpetrators and victims. Physical signs are analogous to those associated with other age groups, although the signs of sexual assault can be both more subtle or more obvious among elders. For example, an elder may sit more awkwardly than usual or may suddenly develop urinary or faecal incontinence following a sexual assault, while unable to provide any history at all. 69 On the other hand, the physical stigmata may be more obvious due to dermal and vaginal atrophy, etc., as for other injuries (see above).
Recognition and education
In spite of international declarations at Adelaide (South Australia) 71 and Toronto (Ontario, Canada), 72 the primary problem in elder abuse is its recognition; this must necessarily precede efforts to research, intervene, reduce and prevent elder abuse. While forensic clinicians are centrally placed to detect, diagnose and prevent elder abuse, it is remarkable that five major textbooks of forensic medicine contain only one brief chapter on elder abuse.
Factors that lower the threshold for suspicion in individual cases have been suggested above. Environments with poorly trained carers, elder patients with behavioural disorders, unexplained and repetitive injuries (especially without efforts to bring to clinical attention), and negative histories being taken at face value are all warning signs. Promulgation of these basic concepts in primary care have been made for about a decade and a half, 15 and getting this part of forensic science into the nursing curriculum would be immensely valuable. 73
Regulatory responses to elder abuse
Mandatory reporting
In the USA, emergency room physicians have the burden of mandatory reporting of many types of patient, and in 43 states this includes suspected elder abuse. 74 Immunity from breach of patient confidentiality is provided, and sanctions are applied if this task is not fulfilled. 75
In the United Kingdom (UK), the Health Protection (Notification) Regulations 2010 includes only a list of infectious diseases. British doctors do have a responsibility to report victims of gun and knife attacks to the police, but only when it is probable that either a crime has been committed or that danger to third parties persists. 76 These are nuanced, legal definitions which few doctors are trained in, and, in any case, make no reference to any particular age group.
Many local government authorities promulgate reporting of child abuse, both by clinicians and the general public; 77 such measures reinforce the principles of recognition, lead to interventions and are doubtless responses to legislation that specifically protects children. But in the UK there are no such protections for elders, although there are activist groups 78 that have begun where local authorities are yet to tread.
At the parliamentary level, the recent Greengross Report has explored some of these iniquities, especially in the environment of residential care homes in the UK.
79
Drawing upon evidence from elders themselves, the friends and relatives of elders, various service providers, and the public authorities, this report takes off from the UN Declaration of Human Rights 1948 and its successor documents, including the UK Human Rights Act, 1998. Among many major gaps in the current legal and regulatory framework, the report found:
Private and voluntary sector home care are not as rigourously regulated as that provided by public authorities; An independent regulatory body inspecting adult social care commissioning is needed; The Equality Act 2010 is not equitably enforced for the benefit of elders, and that age discrimination does not simply apply to the early part of the lifespan; The Care Quality Commission needs enhancement to include the ‘unconstrained voices of service users’, i.e. complaints from elders themselves; An absence of regulation and training of personnel delivering care to elders; The need for a single statutory scheme for adult social care is supported, underpinned by human rights law, placed on the same footing as the National Health Service.
Presumably the findings of this report will inform the current Private Member's Bill, which is due to be printed January 2012 (see below).
Death certification
In the UK, under the present regulations, a Registrar of Births and Deaths has the statutory duty to report certain deaths to the Coroner. An unnatural death, which includes deaths due to self-neglect or neglect by others, is one such reason for referral. Medical practitioners, while having no such statutory duty, are nonetheless encouraged to pre-empt the Registrar and either report such deaths to the Coroner themselves, or at least to discuss such cases with the Coroner's Officer. A Medical Certificate of Cause of Death (MCCD) can still be issued, even when endorsed that the case has been referred to the Coroner.
Deaths due to physical abuse of the elderly are unnatural or violent, and will reach the Coroner in a straightforward manner. However, death due to neglect will not automatically do so. The current MCCD form contains no specific prompt for whether neglect is suspected. Moreover, most training in MCCD completion involves teaching doctors: (a) the difference between a pathological ‘cause’ and a clinical ‘mode’ of death, and (b) sorting the priorities of multiple pathology. If the medical practitioner does not think about the possibility of neglect as a form of elder abuse, then the Registrar sees only an MCCD carrying the names of diseases. Neither of them will report it to the Coroner. Re-design of the MCCD with prompts for neglect or self-neglect as a cause of death would be an improvement. Moreover, how many times does the forensic pathologist encounter a clothed body, removed from a dwelling in a partly putrefied or mummified state, without considering the potential for neglect due to lack of regular visiting?
Parliamentary activity
The private Support and Protection for Elderly People and Adults at Risk of Abuse Bill 2010–2011 is now due for its second reading in the House of Commons on 20 January 2012, following a report from the Select Committee on Health. 80 This second reading was originally scheduled for June 2011, but the half-year delay will enable the Bill to be informed by the Greengross Report 79 (see above). The details of the Bill will not be printed until just before the second hearing, but its stated aims include enhancing awareness of elder abuse, and encourage training in recognition for those who are likely to encounter it.
There are parliamentary commissioners for children in all four provinces of the UK. In contrast, commissioners for the elderly exist only in Wales and Northern Ireland. This issue has been raised by Baroness Bakewell in a House of Lords debate, and Earl Howe (for the Government) seems to agree. 81 Meanwhile, in the Commons, while the Government has no specific minister, there is nonetheless a shadow minister for the elderly (Liz Kendall, MP).
Prospectus
Clinical interventions
Presuming that an elder at risk of abuse is identified, what then are the interventions that might be deployed? Currently, Adult Protective Services interventions are a narrow range, 11 including institutional placement, guardianships, urgent medications and acute hospitalization. The forensic assessment of the type of abuse to be mitigated presumably guides this sort of case work. Completely separate agencies, such as the police and social workers, have to become interested for other sorts of responses, such as legal injunctions or prosecution of those who abuse elders. Bringing the whole medicolegal apparatus into one single, co-ordinated agency could be a useful reform.
Opportunities for research
Easy-to-use screening tools for elder abuse are clearly needed as a priority. While a wide range has been published, they all have their own strengths and weaknesses. 82 While formal theories of elder abuse are beyond the scope of this paper, 55 and not necessarily relevant, one measure of their usefulness would be to guide the design of instruments that forensic clinicians can use as markers for the risk or actual presence of elder abuse. This could be seen as a corollary of the work that has been done with alcohol and drug abuse: complex history taking algorithms are available, but a three-question brief assessment gets far wider use and identifies many more patients. Cross-sectional, population-based studies of abuse and neglect would seem to be feasible provided agreement could be reached on terminology and semantics. Even if study endpoints for community- and institutional-based studies differed, this would still permit useful standardization. 55 With all that in place, comparative studies of interventions, using endpoints identified by forensic clinicians, could become feasible, and potentially generalizable.
Conclusions
The five types of elder abuse (physical, psychological, sexual, neglect and financial) occur worldwide and are not new. All (except possibly for financial abuse) come to the attention of the forensic clinician commonly. The forensic clinician then has two immediate responsibilities: (i) to the patient, where competent history and examination is sine qua non, and (ii) to investigate, interpret and recognize patterns of any type of harm. Many of these forms of harm are not difficult to grasp, and are similar to those seen in children (see above). In the elderly, they certainly lead to both mortality and morbidity. Meanwhile, a patchwork of interventions is being deployed, partly because research into elder abuse is in its infancy. Standardized terminology and diagnostic criteria remain unsettled.
The forensic clinician's additional responsibility is to elevate the issue of elder abuse in the wider professional realm. Gerontologists, emergency and accident clinicians, general practitioners, community nurses, etc., and others, must all integrate some forensic skills into their practices if the problem of elder abuse is to be properly identified, quantified and prevented.
DECLARATIONS