
Abstract
Aims
To determine whether the brain–body weight ratio is increased in sudden infant death syndrome (SIDS).
Methods
Review of autopsy files from Forensic Science SA, South Australia was undertaken over an eight-year period from 1999 to 2006, with classification of cases according to the San Diego definition. Sudden and/or unexpected deaths in previously healthy infants due to asphyxia or infection were selected as controls.
Results
There were 42 SIDS cases and 25 controls. The SIDS cases were aged from 1 to 42 weeks (mean: 16.26 ± 1.5 weeks) with a male to female ratio of 26:16. The control infants were aged from 3 to 48 weeks (mean: 19.24 ± 2.9 weeks) (P > 0.05) (M:F = 16:9) and included 13 cases of asphyxia and 12 cases of sepsis. Comparison of the brain–body weight ratios failed to demonstrate a significant difference: SIDS mean = 0.121 ± 0.003; control mean = 0.115 ± 0.003 (P > 0.05).
Conclusion
Although, there was a trend towards higher brain–body weight ratios in SIDS infants, this did not reach significance. The role of brain weight in the aetiology of SIDS remains controversial.
Introduction
Sudden infant death syndrome (SIDS) is defined as ‘the sudden unexpected death of an infant less than one year of age, with onset of the fatal episode apparently occurring during sleep, that remains unexplained after a thorough investigation, including performance of a complete autopsy and review of the circumstances of death and the clinical history’. 1
The pathogenesis of SIDS has remained elusive with many theories being proposed over the years based on a variety of pathological findings. 2,3 One observation that has been made concerns the weight of the brain, with a number of studies showing an apparent increase in the brain weights of SIDS infants. This has been attributed to a variety of possible mechanisms including congenital megalencephaly and oedema, the latter most recently related to possible differences in aquaporin four expression. 4–9 Other studies have, however, failed to substantiate an increase in brain weight in SIDS infants, 10–12 with some authors even suggesting ‘that organ weights obtained from SIDS infants could be used as norms in the first year of life’. 12 Given this significant divergence of results and opinions, a group of South Australian SIDS cases that had been re-classified using the San Diego definition were compared with a carefully selected control group to determine whether a difference in brain–body weight ratios could be identified in this population.
Materials and methods
Autopsy cases of sudden infant deaths taken from coronial files at Forensic Science SA, South Australia were available over an eight-year period from 1999 to 2006. These cases had been previously used in a study of cerebral β-amyloid precursor protein deposition (unpublished). All cases had been subject to full police and coronial investigations and had undergone complete autopsies with formal neuropathological examinations. Cases where death had been attributed to SIDS had been classified according to the criteria specified in the general San Diego definition of SIDS. 1 Cases not meeting the San Diego criteria had been excluded from the study. A group of control infants were selected from cases where sudden or unexpected deaths had occurred in previously healthy infants due to asphyxia or infection. Brain–body weight ratios were selected for comparison purposes rather than brain weight alone, to avoid bias from prematurity, as gestational age at delivery was not available in some cases.
At autopsy, the brains had been cut in a standard manner at the level of the upper cervical cord at the foramen magnum, had the dura removed and had been weighed after fixation in 10% formalin for 10–14 days. The age, gender, body weight and weight of the brain were recorded. Statistical analysis was conducted using the Student's t-test.
Results
A total of 67 cases were included in the study consisting of 42 SIDS cases and 25 controls. The SIDS cases were aged from 1 to 42 weeks (mean 16.26 ± 1.5 weeks) with a male–female ratio of 26:16. The control infants included 13 cases of death due to asphyxia and 12 cases of lethal infection (age range 3–48 weeks, mean 19.24 ± 2.9 weeks). Asphyxial deaths were caused by acute upper airway obstruction from suffocation or positional asphyxia. Lethal infections included septicaemia, pneumonia and two cases of viral myocarditis. There was no significant difference in ages between the SIDS infants and controls. Neuropathological examinations in all the cases did not reveal any significant microscopic abnormalities.
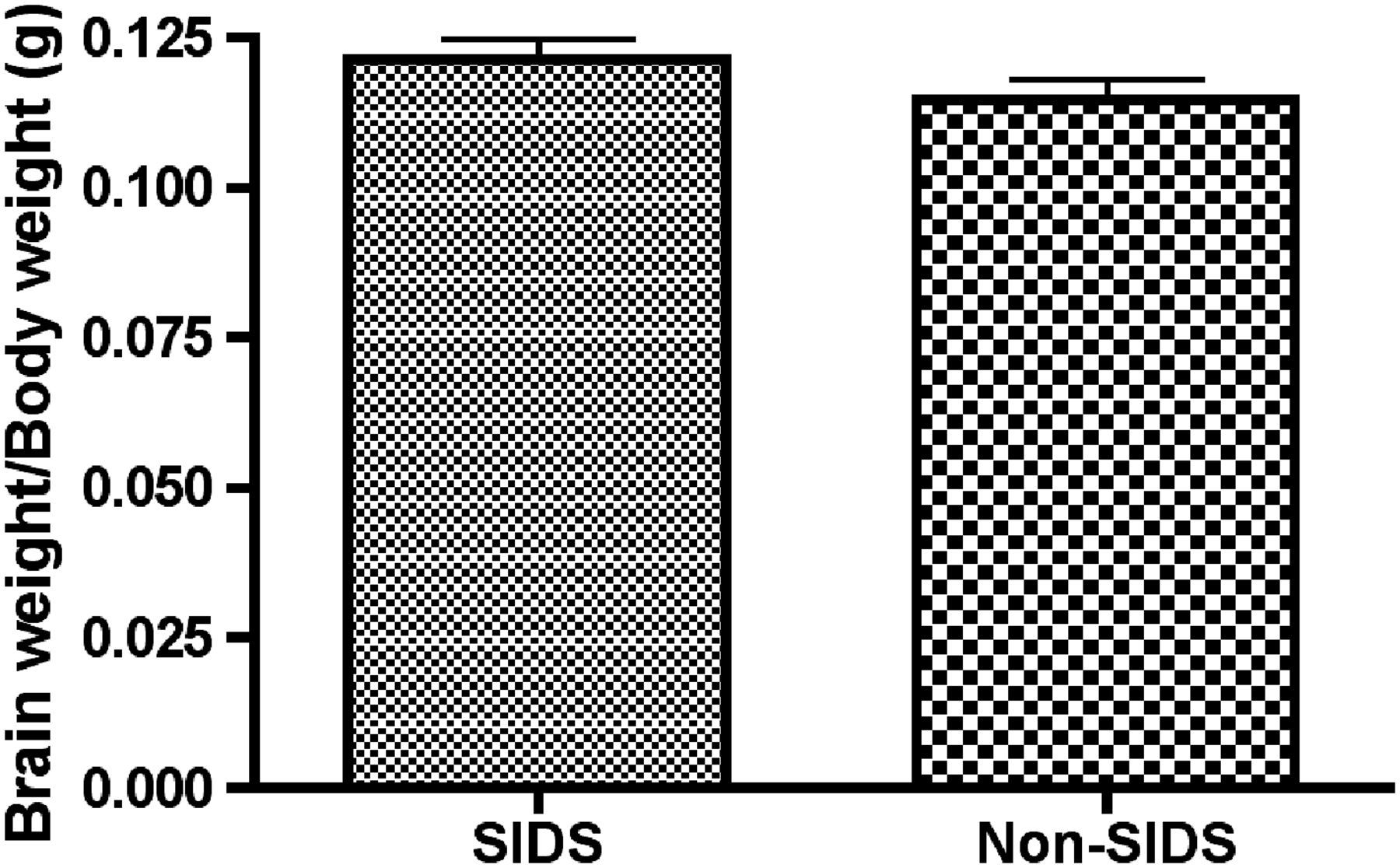
Comparison of the brain–body weight in SIDS infants demonstrated a positive correlation as would be anticipated (r = 0.8315) (Figure 1). Comparison of the brain–body weight ratios in the 42 SIDS infants to the 25 control infants, however, demonstrated no significant differences: SIDS mean 0.121 ± 0.003 and control mean 0.115 ± 0.003 (P > 0.05) (Figure 2). Comparison of seven SIDS infants to seven age- and sex-matched controls in both control groups (asphyxia and infection) also revealed no significant differences: (a) SIDS – mean 0.119 ± 0.001, asphyxia controls – mean 0.108 ± 0.007; (b) SIDS – mean 0.118 ± 0.009, infection controls – mean 0.114 ± 0.006.
Comparison of brain weights to body weights in 42 infants whose deaths had been attributed to SIDS demonstrating a positive correlation Comparison of brain–body weight ratios in 42 SIDS infants and 25 controls demonstrating no significant differences (P > 0.05)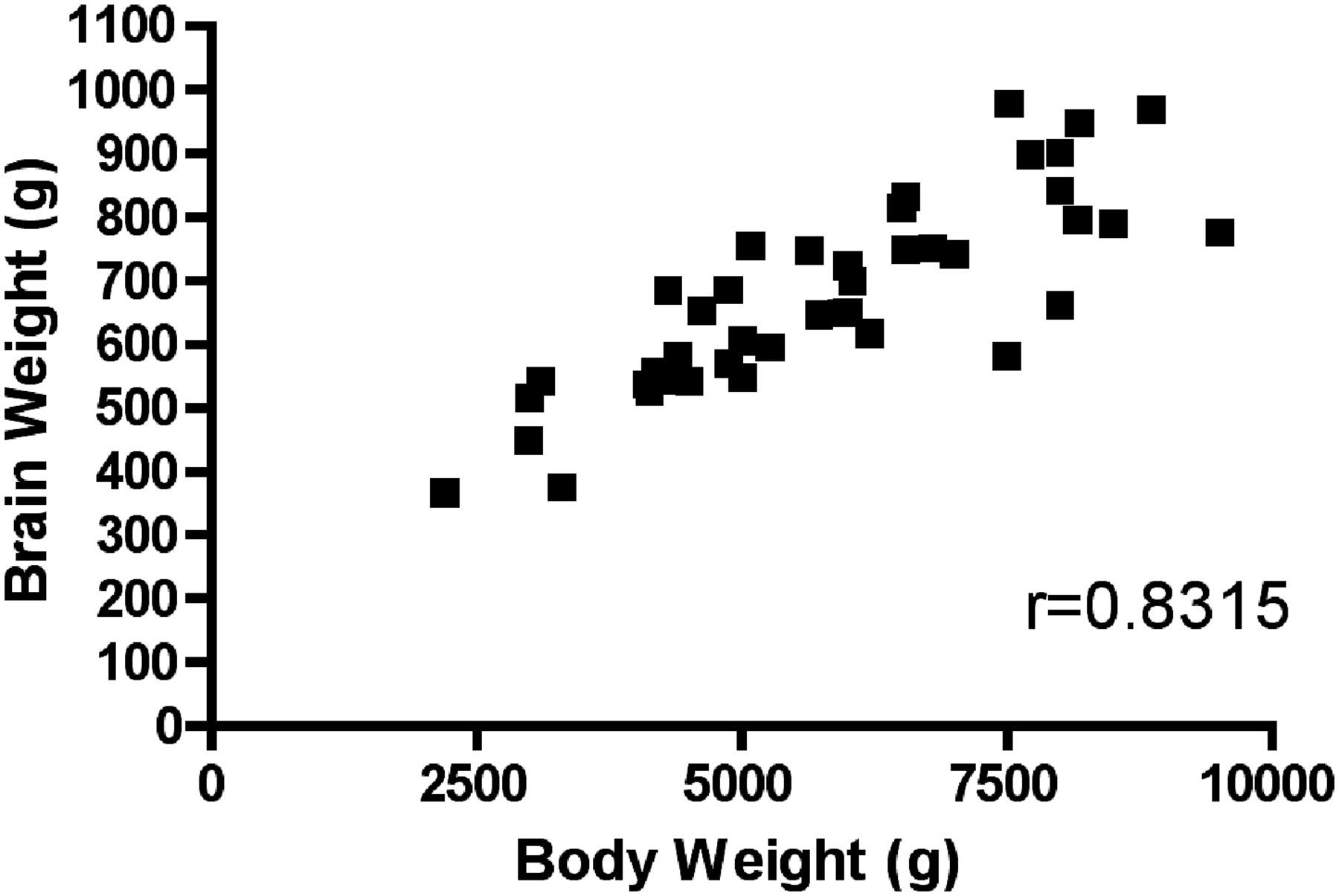
Discussion
The issue as to whether infants who die of SIDS have increased brain weights may be of considerable significance as it may shed light on possible mechanisms of death and pathogenesis. For example, if an increase in brain weight was due to congenital megalencephaly, this might suggest that there are other subtle congenital abnormalities of cerebral 13,14 or other major organ functions that could contribute to death; i.e. megalencephaly has a number of quite diverse causes that include chromosomal abnormalities, metabolic disturbances and neurocutaneous syndromes. It may also manifest with seizure activity. 15,16 Alternatively, it has been suggested that the increase in brain weight may be due to abnormal cerebral development associated with cytokine upregulation that could adversely affect central neural control. 4 Equally, if SIDS infants are predisposed to the development of cerebral oedema, this may imply that there are abnormalities of regulation of the blood brain barrier with disturbances in water homeostasis related to aquaporin-four mutations that are not present in other infants. 9
The present study has not, however, shown a significant difference in brain–body weight ratios in SIDS infants compared with controls. A value of the current study is that it has used recent cases where the diagnosis of SIDS had been made following careful autopsy and medicolegal evaluation, and that have been classified according to established contemporary international criteria. 1 Although brain weight may alter with formalin fixation, the brains in both SIDS and control groups were subject to identical brain handling protocols and time schedules. Although the numbers in this study are small, there was a trend for greater brain–body weight ratios in SIDS infants compared with controls which did not reach significance. Thus, these data do not reveal a demonstrable increase in the brain–body weight ratio in SIDS cases from South Australia that could contribute to the underlying occult pathological processes, congenital abnormalities or oedema. A weakness of the study is that we were not able to get sufficient numbers to enable a meaningful analysis of brain–body weight ratios in relation to particular risk factors.
A difficulty that has been noted in this area lies in finding reliable normal data for brain weights in infants, as cerebral oedema may develop rapidly in a number of conditions 6,17 and formalin fixation may result in an artefactual increase in brain weight. 18 For this reason, brain weights in the current study were compared with the controls that had been processed in an identical manner, rather than to published normal values. A further difficulty involves the assessment of cerebral oedema after death. Although we have been able to demonstrate oedema in an animal model by immunohistochemically staining for albumin, 17 we have not been able to replicate this in the human tissues due to non-specific staining associated with prolonged postmortem intervals. Thus, brain weight remains one of the most reliable indicators of oedema at autopsy.
It has been proposed that central and peripheral nervous system dysfunction may be responsible for a variety of cardiorespiratory abnormalities found in infants who have subsequently died of SIDS. Whether this results in acute or chronic cerebral hypoxia is unclear. Neuropathological findings have included brainstem gliosis, increased numbers of neuronal dendritic spines, white matter changes, neurotransmitter receptor changes and axonal and chemoreceptor abnormalities. 13,14,19 Only cases where temporary resuscitation has occurred will manifest changes of hypoxic ischaemic encephalopathy. 20 Findings in the literature on brain weights have, however, been contradictory. Shaw et al. in a study of 79 SIDS infants proved that all of the brain weights (prior to fixation) were above the 50th percentile when compared with the published data, with 81% above the 95th percentile and 19% above the 99.9th percentile. 7 Although other authors have also demonstrated increases in the brain weight of SIDS infants, 4–6 a problem exists in determining how stringently the ‘diagnosis’ of SIDS had been made in the groups studied, what controls are used and what investigative parameters had been undertaken, 21,22 as variations in these areas may markedly affect diagnostic groupings. A similar problem also exists in series where no differences were found between the weight of the brain in SIDS cases and controls as specific information on death scene examination and other investigations may not have been detailed. 10–12
Whether contradictions in the literature reflect difficulties with case accession or genuine differences in geographically separate subsets of SIDS cases remains to be clarified. It appears, however, that an increase in brain weight is not a constant finding in all groups of SIDS infants. Future studies could examine brain–body weight ratios in relation to risk factors such as shared sleeping, cigarette smoke exposure and prematurity.