
Abstract
Home birth is becoming increasingly popular. Labour in the privacy and comfort of a familiar environment has clear appeal. Home birth is usually as safe for low-risk women with appropriate prenatal care. Yet events during delivery can be unpredictable and may be stressful for unprepared family members. Here we report a case of Tako-tsubo cardiomyopathy, also known as broken-heart syndrome, in a relative attending an impromptu home delivery. Thus, while home delivery is generally safe for the mother we ask: is it safe for everyone involved?
INTRODUCTION
Home birth is becoming increasingly popular. Labour in the privacy and comfort of a familiar environment has clear appeal. Home birth is usually as safe, if not safer than hospital births for low-risk women with appropriate prenatal care. 1 Yet events during delivery can be unpredictable and may be stressful for unprepared family members. Thus while home delivery is generally safe for the mother, we ask: is it safe for everyone involved?
CASE REPORT
With delivery of a second grandchild imminent our patient, a 59-year-old lady, was resident with her son's family expecting to care for the first born when the time came. Her daughter-in-law, gravida 2, para 1, had wanted a home birth. Unfortunately midwifery cover for home delivery was not supported when labour began in the early hours of the morning. Grandma was called into action, allowing the rest of the family to attend hospital for assessment. It was felt safe to return home to await assistance from the home birth team at the start of the working day. The baby had different ideas.
Shortly after returning home, and with dawn a few hours away, labour progressed rapidly and the baby's head arrived in the perineum. An ambulance was summoned and Grandma ran out to flag it down. The ambulance crew drove past the animated old lady, who returned to the house in some distress to be greeted by a new grandson, and a fresh placenta. At this point she experienced severe central crushing chest pain. So while the first ambulance took mother, baby and placenta to hospital, another was called for Grandma.
Emergency assessment by the paramedic crew revealed electrocardiographic changes compatible with antero-apical ST elevation myocardial infarction (Figure 1). With ongoing pain the patient was given anti-platelet therapy and transferred to the closest acute-cardiac centre for treatment.
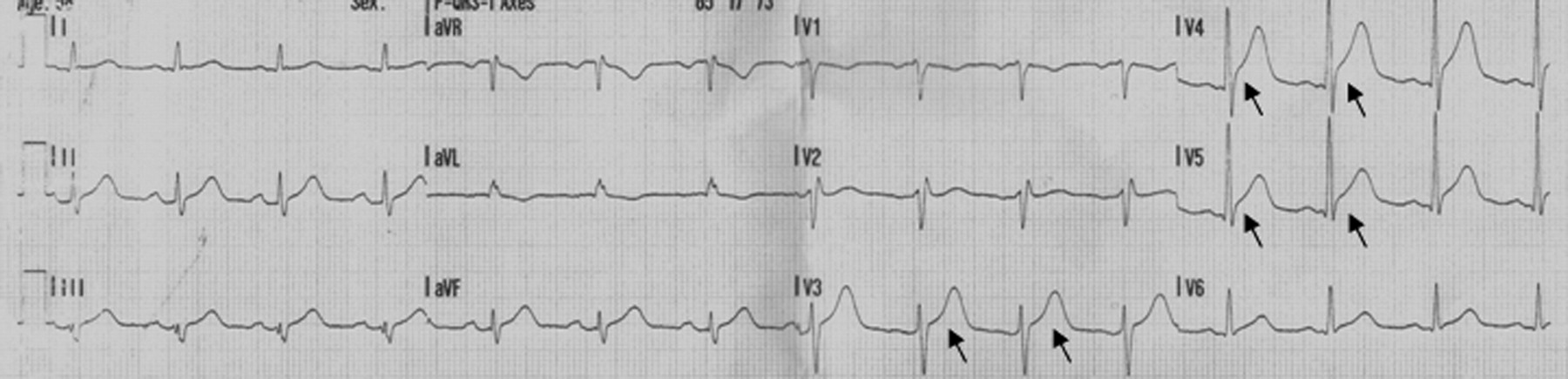
ECG. Presenting 12-lead ECG: Contiguous ST elevation (arrow) in leads V3, V4 and V5 >2 mm with ongoing chest pain satisfies primary percutaneous coronary intervention referral or thrombolysis criteria. ECG, electrocardiogram
Coronary angiography revealed a right dominant circulation without a significant focal stenosis. The left main stem was unobstructed. The left anterior descending artery had mild atheroma only. There was moderate plaque in the mid-circumflex vessel which was not flow limiting. The right coronary artery demonstrated mild atheroma only. Collectively these angiographic findings excluded an acute coronary event as the cause of the clinical presentation. However, left ventriculography showed the anticipated findings of a stress-induced ‘Tako-tsubo’ cardiomyopathy with extensive antero-apical regional wall motion abnormality and depressed systolic function (Figure 2). By contrast, troponin T was only modestly elevated at 1.3 ng/mL (normal range in our laboratory is <0.04 ng/mL). Heart failure therapy was initiated, and the patient observed for several days prior to discharge. Follow-up echocardiography, two weeks postdischarge, showed left ventricular systolic function had normalized with no evidence of regional wall motion abnormality.
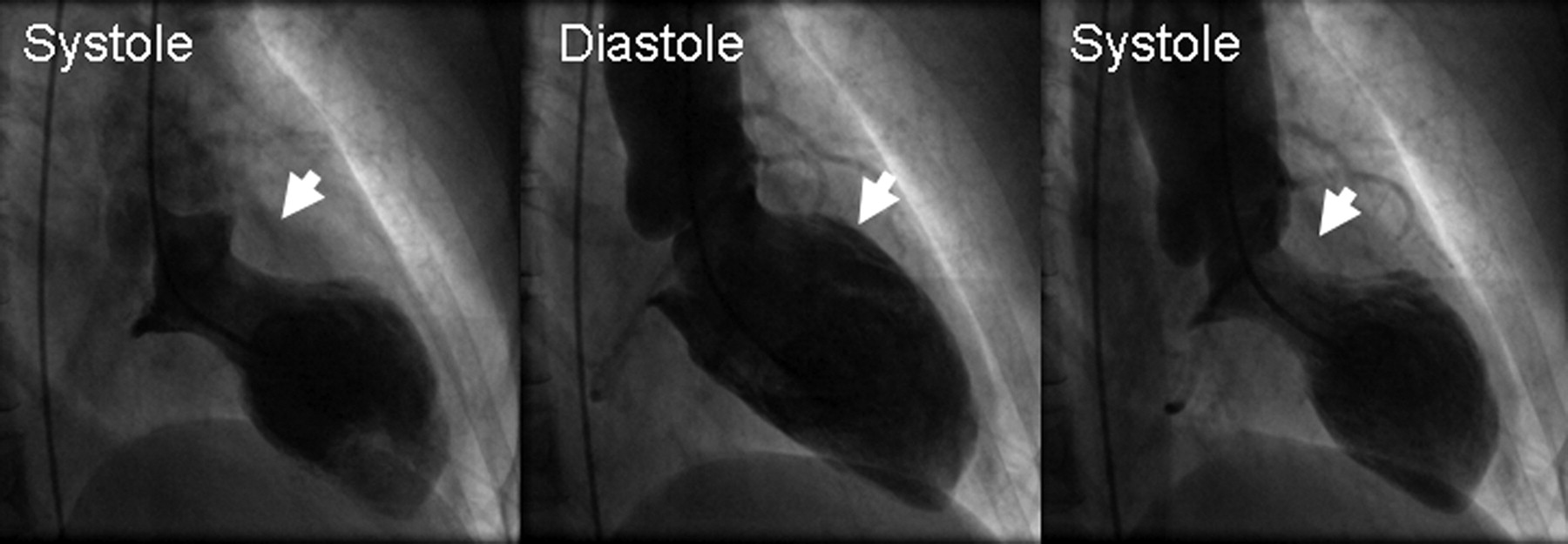
Left ventriculography. A pigtail catheter inserted from the femoral artery into the left ventricular cavity is used to deliver contrast throughout the cardiac cycle. In Tako-tsubo cardiomyopathy, clear wall motion abnormalities are present which are not restricted to a single coronary artery territory. Arrows indicate the base of the heart which retains normal contractile activity in contrast to the apex which shows little contractile activity. This appearance is commonly known as ‘Tako-tsubo’ cardiomyopathy after the Japanese octopus-pot that it morphologically resembles
COMMENT
Tako-tsubo cardiomyopathy was first described in 1991 by a group based in Hiroshima, a Japanese coastal city. 2 Tako-tsubo means ‘octopus pot’, and was the traditional method to catch inquisitive cephalopods. This earthenware pot resembles an amphora but with a rounded bottom and an opening after a long neck. It has similar appearances to the left ventriculogram in systole associated with the condition. The condition is variously known as ‘apical ballooning syndrome’, ‘broken-heart syndrome’ and ‘stress-induced cardiomyopathy’; the later two romantically referring to the stressful or emotional precipitants approximately two-thirds of patients presenting with Tako-tsubo usually describe before symptom onset. 3
Importantly, Tako-tsubo cardiomyopathy is transient, and normally reversible. It mimics myocardial infarction, accounting for about 2–5% of the STEMI (ST elevation myocardial infraction) population,
4,5
and is characterized by the following:
6
Typical regional wall abnormalities of apical ballooning, where only the basal segments retain contractile activity, the remaining segments are akinetic; New ST segment elevation or T-wave inversion on electrocardiogram; Normal coronary arteries on angiography.
Ninety percent of patients are postmenopausal women.
7
Investigations typically reveal elevated cardiac troponins, with hypokinesis of the apical segments of the left ventricle and reduced ejection fraction on echocardiogram. As in our case, the magnitude of troponin rise is often more modest than that expected for a large wall motion abnormality due to ischaemia. The gold standard for diagnosis, however, relies on cardiac catheterization, to document normal coronary arteries.
8
The initial clinical course is variable,
8
but importantly unpredictable in the early stages.
There is no randomized controlled data to guide the treatment of patients with Tako-tsubo cardiomyopathy. The general consensus is that they be treated with diuretics, angiotensin-coverting enzyme inhibition and beta-blockade which are the mainstay of conventional heart failure treatment. However, dynamic obstruction of the left ventricular outflow tract (LVOT) is reported in up to 18% of Tako-tsubo cases. 9 Beta blockade can reduce LVOT obstruction, and oppose the adrenergic hormones implicated in the disease mechanism (below). Therefore, in contrast to conventional heart failure management (where beta-blockade is generally withheld in acute congestive cardiac failure), beta-blockers may still be used with caution. Not all patients will respond to these measures. In this situation mechanical circulatory support, initially with an intraaortic balloon pump, is perhaps preferable to the institution of inotropic therapy given that inotropes may (1) theoretically contribute to the sympathetic over-stimulation (below) and (2) worsen or induce LVOT obstruction, in-hospital mortality is about 2%. 4 Recovery of the regional wall motion abnormality within six weeks is typical, and recurrence rates are low, in the order of 5%.
What causes Tako-tsubo cardiomyopathy?
Several possible mechanisms 4,10 that could lead to Tako-tsubo have been hypothesized. The most accepted theory remains stress-induced cathecholamine release, with subsequent stunning of the myocardium. 3 The plausible causative implication of the ‘fight-or-flight’ hormones in this process therefore has led to caution with the use of sympathomimetic inotropes in patients with diuretic refractory heart failure or overt cardiogenic shock. The regional wall motion abnormality is attributed to the differential expression of adrenoreceptor subtypes that has a marked transition in the human heart.
SUMMARY
Home birth can be a stressful event for the unprepared or unsupported. Here we report a case of Tako-tsubo cardiomyopathy in a relative attending an impromptu home delivery. Stress-induced cardiomyopathy is becoming increasingly recognized in the acute myocardial infarction population, and while the outcome is favourable in most patients, a small number will have prolonged hospital stays and may not survive the event.
DECLARATIONS