
Abstract
Purpose
To detect the influence of pelvic vein incompetence (PVI) on pain levels in patients with varicosity of the lower limb.
Materials and methods
Women of child-bearing age with symptomatic primary or recurrent varicosity of the greater saphenous vein (GSV) were prospectively included in two groups depending on the presence or absence of phlebographic signs of PVI. Pain assessment was carried out with the help of a visual analogue scale (VAS).
Results
Forty women were included in the study. Nineteen of them had phlebographic evidence of PVI (group A), whereas 21 were included in the control group (group B). Patients of group A reported a higher median total pain level than patients of group B (group A median 62, range 25–100; group B median 32, range 0–100; P = 0.001). In group A, patients experienced a median level of pain of 67.2 at the lower limb in the standing position (range 40–100) versus a median of 50.3 (range 36–81) in patients of group B (P = NS). The median level of leg pain in the sitting position was 41.2 (range 0–67) in patients of group A and 38.1 (range 0–46) in women of group B (P = NS). Pelvic pain level in the standing position was higher (P = NS) in patients of group A (median 72.2, range 50–91), than in women of group B (median 20.1, range 0–41). In patients of group A, statistically significant (P = 0.0001) higher VAS scores for pelvic pain level in sitting (group = A median 67.2, range 59–71; group B median 18.1 range 0–35) were reported.
Conclusions
In a small population of patients with GSV varicosity, overall pain levels were significantly higher in a subgroup of patients with phlebographic signs of PVI. This finding suggests that the presence of PVI might influence the intensity of varicosity symptoms.
Introduction
Besides aesthetic problems, leg swelling is the most frequent reason why patients with varicosities consult physicians. Symptoms are known to worsen in the standing and sitting position, due to the augmented blood flow to the distal parts of the leg. Besides swelling, leg pain and heaviness are typical. In late stages, venous claudication can appear.
In women of child-bearing age with varicosity at the lower limb, the presence of a pathological reflux in pelvic veins, better known as pelvic vein incompetence (PVI), can complicate this common clinical entity. 1 Furthermore, dyspareunia and dysuria have often been documented in this subgroup of patients. 2–4
In the last decade, the researchers have focused their attention on the clinical influence of minimal invasive treatment of PVI. 2–4
As the magnitude of blood reflux to the distal part of the lower limb is known to be one of the determining factors of varicosity symptoms, the presence of reflux pathways originating in the pelvis and connecting to the incompetent saphenofemoral junction (SFJ) in patients with PVI might have an influence on the severity of symptoms.
Based on this hypothesis, we conducted a prospective study in order to evaluate if there are differences in the pain levels of female patients with primary or recurrent varicosity of the greater saphenous vein (GSV) and phlebographic evidence of PVI as compared with a control group of patients with isolated GSV varicosity.
Materials and methods
Female patients of child-bearing age with symptomatic GSV varicosity of the lower limb were recruited between January and December 2006 at our vascular centre. The study protocol was approved by our local ethics commission.
Inclusion criteria were: symptomatic primary or recurrent varicosity of the lower limb, with ultrasonographic evidence of pathological reflux at the SFJ. All patients gave written informed consent to take part in the study.
Exclusion criteria were: age under 18 years, known vascular malformation in the abdomen or at the lower limb, actual pregnancy, thrombophlebitis of the GSV, and a history of deep vein thrombosis at the lower limb.
Patients who met the inclusion criteria underwent a meticulous clinical examination. At the time of patients' hospital admission, co-morbidities, as well as standardized physical examination findings, were recorded. Clinical data and stage of PVI were collected in all patients. The clinical evaluation included a history of congestion symptoms and a physical examination focusing on the inspection of the pelvic region and the lower limbs in order to detect signs of venous incompetence. As clinical signs of PVI, prominent varices at the thigh and varicose veins with proximal distribution (medial and dorsal veins) were considered.
A duplex examination of the groin as well as of the lower leg was performed. All venous segments were tested in order to detect pathological reflux as well as obstruction/occlusion.
Previous surgery due to lower limb varicosity, pregnancies as well as clinical extension and anatomical localization of varicosity based on the clinical, aetiological, anatomical and pathological (CEAP) classification 5 were recorded.
In particular, we defined C0 as no visible or palpable signs of venous disease, C1 as telangiectasies or reticular veins, C2 as varicose veins, C3 as oedema, C4a as pigmentation or eczema, C4b as lipodermatosclerosis or atrophie blanche, C5 as healed venous ulcer and C6 as active venous ulcer.
Only patients who were suspected of having PVI, on the basis of clinical signs and symptoms as described before, 6 underwent additional phlebography as well as eventual endovascular treatment of incompetent pelvic veins when deemed necessary.
The vulval varices during pregnancy, increase of venous insufficiency symptoms during intercourse, dyspareunia, dull pelvic ache of unclear origin and a positive history of recurrent surgery of the SFJ were considered clinical signs and symptoms of PVI.
The patients of the control group did not receive further invasive diagnostic examinations. Patients were included in two subgroups depending on the presence or absence of phlebographic signs of PVI.
Pain assessment was carried out at the time of the first presentation with the help of a visual analogue scale (VAS) graduated from 0 (no pain) to 100 (intolerable pain). In particular, besides an overall pain level, the intensity of the following symptoms was chosen to be evaluated during consultation:
Leg pain in the sitting and standing position; Pelvic pain in the sitting and standing position.
The presence of dyspareunia, dysuria and leg swelling in the sitting as well as in the standing position was also documented in a standardized way.
The Mann-Whitney U test was used for continuous variables and the Fisher's exact test was used for discrete variables. Metric data such as age or pain levels are reported as median. A P value of >0.05 was considered statistically not significant and reported as P = NS.
Results
From January to December 2006, 40 women of child-bearing age with primary or recurrent GSV varicosity fulfilled the previously mentioned criteria and were included in this prospective study. After clinical and phlebographic examination, 19 (47.5%) patients were found to have PVI and were included in the study group (group A), while 21 (52.5%) patients represented the control group (group B).
An incompetent ovarian vein was recognized in 14 (73.6%) patients of group A, dilated plexi in 12 (63.1%) and an incompetent IIV in six cases (31.5%). Six patients were found to have multiple incompetence.
An endovascular treatment with coiling of the incompetent veins was performed in 10 cases. The median age was 41 years in group A (range 29–55) and thereby significantly higher (P = 0.043) than in group B (median 35 years; range 18–52). Overall, in 13 cases a varicose vein recurrence after previous stripping of the GSV and in 27 cases a primary varicosity were recorded (see Table 1: demographic data).
Demographic data
*Age is expressed in years
NS = not significant; CEAP = clinical, aetiological, anatomical and pathological
The overall mean number of pregnancies was 2.5 per patient (range 0–7). Thirty (75%) patients presented with clinical class C2 according to the CEAP classification (group A 78.9%; group B 71.4%) and 10 (25%) with class C1 (group A 21.1%; group B 28.6%). There were no cases of oedema of the legs or venous ulcerations. Varicose veins at the thigh and/or at the calf were the predominant finding.
In group A, dyspareunia was reported by five patients (23.8%), while dysuria was reported only by four (21%) and pain at intercourse by nine (47.3%). In group B, no patient referred of dyspareunia or dysuria, while pain at intercourse was reported in four cases (19%).
Localized pain at the lower limb in the standing position was the symptom most frequently reported (group A 78.9%; group B 85.7% – P = NS), followed by leg swelling in the standing position (group A 78.9%; group B 80.9% – P = NS), leg pain in the sitting position (group A 78.9%; group B 66.6% – P = NS), leg swelling in the sitting position (group A 57.8%; group B 66.6% – P = NS) and pelvic pain in the standing and sitting position (group A 73.6%; group B 19% – P = 0.000).
Twenty-four patients experienced worsening of their symptoms during intercourse (group A 71.4%; group B 47.4% – P = NS). Dyspareunia and dysuria were present in 10 (group A 47.3%; group B 4.7% – P = 0.032) and eight (group A 36.8%; group B 4.7% – P = 0.042) cases, respectively.
Patients of group A reported a higher median total pain level than the patients of group B (group A median 62, range 25–100; group B median 32, range 0–100; P = 0.001) on VAS (Figure 1).
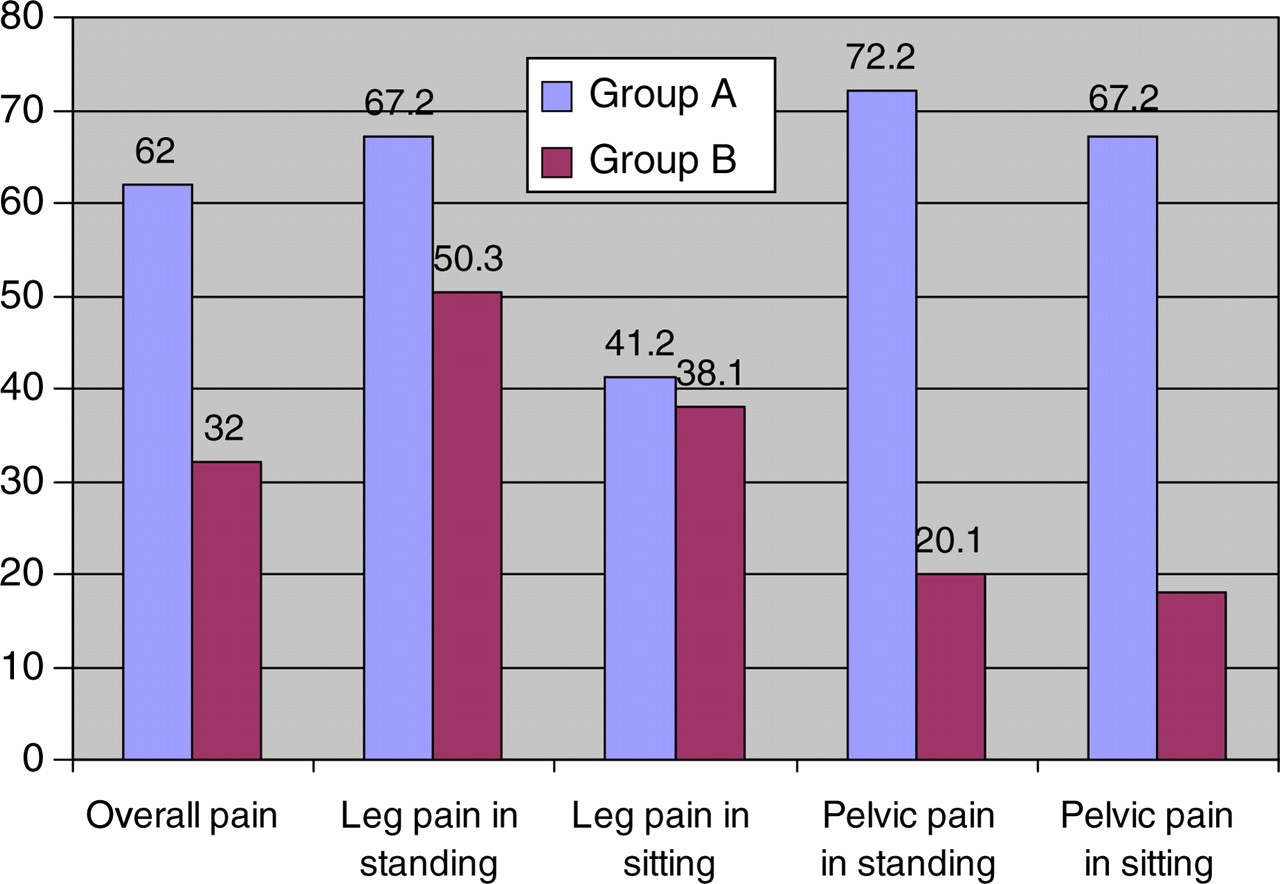
Leg and pelvic pains basing on VAS (0–100). Pain level medians are reported at the top of each column
Furthermore, patients of group A experienced a median level of localized pain of 67.2 at the lower limb in the standing position on VAS (range 40–100), versus a median of 50.3 (range 36–81) in patients of group B (P = NS). The medial level of leg pain in the sitting position was 41.2 (range 0–67) in patients with phlebographic evidence of PVI and 38.1 (range 0–46) in women with isolated varicosity of the lower limb (P = NS). Pelvic pain levels in the standing position were higher (P = NS) in patients of group A (median 72.2, range 50–91), as compared with group B (median 20.1, range 0–41). A similar difference was noted for pelvic pain levels in the sitting position (group A median 67.2, range 59–71; group B median 18.1, range 0–35; P = 0.0001).
Discussion
Taylor 7 used the term ‘venous congestion syndrome of the pelvis’ in 1947 to describe a combination of symptoms consisting of pelvic varicosities, dysmenorrhoea, pain during cohabitation and pelvic pain. This classical tetrad of symptoms is associated with a typical pattern of varicosities. Scultetus et al., 3 in an overview of the female pelvic venous syndrome, described three different clinical presentations: vulvar varicosities without signs of pelvic congestion, varicose veins at the medial and posterior aspect of the thigh, usually caused by incompetent ovarian veins and gluteal as well as vulvar varicosities that are often caused by reflux in the internal iliac veins.
PVI affects young multiparous patients. The typical lower abdominal pain is variable in intensity and duration, sometimes extending to the posteromedial thigh and buttock areas, and often accompanied by dyspareunia, bladder irritability and urgency. 8,9 The abdominal pain is exacerbated by movement which causes a sudden increase in intra-abdominal pressure, such as walking, bending, standing, lifting or sexual intercourse. 7,8,10,11 The causes of pelvic venous congestion are probably multifactorial, involving both mechanical and hormonal factors. During pregnancy, the vascular capacity of the ovarian veins may increase 60 times and remain this way for months after delivery. 12 Dilation of ovarian veins causes vascular incompetence and retrograde venous flow. Furthermore, dilated veins are more frequently observed with increasing parity. 11–13
The often associated worsening of congestion symptoms during intercourse, the higher prevalence in multiparous women 6 as well as the positive therapeutic effects of hormonal substitution on symptoms 14 suggest that sexual hormones could play a crucial role in determining this peculiar clinical entity.
A direct influence of female sexual hormones levels on the aetiology of lower leg varicosity has been already documented, 15 and could be one of the explanations of the higher prevalence of this disease in females.
Congested pelvic venous flow can be directed into the lower extremities through the collateral channels of obturator, inferior gluteal, external or internal pudendal veins or other pelvic venous collaterals. Moreover, the congested pelvic venous blood may flow into the internal iliac vein or the superficial and deep venous systems of the lower extremities. 16 Therefore, patients with unexplained labial and thigh venous dilation should have phlebographic examination of pelvic veins as well as ultrasound of the lower extremity venous system.
In some cases, pelvic reflux to the venous system of the lower limb can result in visible varicosities at the lower limbs and/or in recurrence after surgical treatment of them. 17
We prospectively measured pain levels in a small cohort of patients affected by varicosity of the lower limbs. In particular, in order to prove the hypothesis that pain levels are higher in patients with associated PVI, we used a control group of women suffering of isolated lower limb varicosity.
Using a standardized examination protocol, we selected patients who had to undergo phlebography of the pelvic veins because of suspected PVI.
In this patient cohort, control and study groups were homogenous regarding demographic characteristics, even if the median age of patients with PVI was higher than in the control group (see Table 1).
Recurrence was the reason for medical consultation more often in patients without PVI, even if this did not reach statistical significance and did not seem to correlate with the different symptom patterns.
The augmented pathological reflux through the incompetence of both pelvic and lower limb veins might explain the significantly higher total pain levels in the group of patients affected by PVI, who also reported the specific pelvic symptoms more often and in addition presented with more advanced clinical signs of chronic venous insufficiency (CVI) based on CEAP classification.
Furthermore, pelvic pain in the sitting and standing position were more often reported by patients with PVI (P 0.001).
The fact that patients with PVI presented with more advanced clinical stages of CVI could be one reason for their higher median pain levels.
Chronic pelvic pain is an often 1 overviewed symptom. Identification of pelvic reflux sources generally follows a complicated diagnostic history. Patients undergo repeated laparoscopic as well as transvaginal duplex examinations after consulting general practitioners as well as gynaecologists. In most of the cases, vascular specialists recognize the venous origin of the disease only in late stages.
This prospective study also has some limitations. Not performing phlebographic examinations in patients without signs and symptoms of PVI should be seen as a weakness. However, the effects of radiation exposure can have serious effects on women with child-bearing potential. All patients of our study cohort were asked about recent changes in menstrual rhythm, which could raise the suspicion of pregnancy. In cases where a pregnancy could not be excluded, patients were not offered phlebography. The same was true for patients who were still breast-feeding after a recent delivery.
In these cases, the already reported high sensitivity and specificity of duplex examination 6 in suspecting PVI was in our opinion also a valid argument against the liberal use of phlebography.
An objective evaluation of the entity of clinical symptoms is difficult, as multiple variables might strongly influence individual evaluation. Furthermore, it could be difficult to identify patients with incidental PVI, in which the pelvic pains are caused by other factors.
VAS has been widely used in the determination of symptom severity in many studies dealing with varicosity, 18,19 and should be considered as the most valid way to express sufferance grades.
Conclusions
Based on the results of this prospective investigation we can affirm that in a small cohort of patients with varicosity of the GSV, PVI seemed to cause a worsening of overall pain levels.
The predictivity of these data and their use in the daily practice needs to be confirmed by larger studies on higher number of patients.