
Abstract
Objective
Compression hosiery is widely used in the prevention and management of symptoms related to varicose veins. However, there are still gaps and questions in relation to its benefit. This review seeks to examine the current evidence regarding the effectiveness of compression hosiery in the treatment of varicose veins.
Method
Prospective, randomized controlled trials (RCTs) evaluating compression hosiery in the treatment of varicose veins were sought. Where RCTs were unavailable other evidence was included. Studies were included if they evaluated the application of compression to patients with a diagnosis of varicose veins. Twelve electronic bibliographic databases and 18 internet-based research resources were searched. Inclusion or exclusion of trials was decided by two reviewers acting independently.
Results
The search strategy identified 25 studies. Eleven were RCTs or systematic reviews, 12 non-randomized studies and two guidelines. No consensus was found regarding the class of compression needed for the effective management of varicose veins. Wearing compression improved symptom management, but could be confounded by the exclusion of high number of non-compliant patients within the trials. Wearing compression to slow the progression, or prevent the reoccurrence of varicose veins could not be supported by the current published evidence.
Conclusion
The evidence for the benefit of compression hosiery for varicose veins was equivocal. The published literature was often contradictory and had methodological flaws.
Introduction
Compression hosiery is widely used in the prevention and management of symptoms for patients with varicose veins 1 and is often the first treatment option offered prior to surgical management. 2 A number of authors have highlighted the fact that compression has been used in one form or another as a treatment for varicose veins for several hundred years.3–6 Compression stockings rely on graduated external pressure, with the highest pressure at the ankle, being applied to the calf or thigh muscle. 7 This raises the interstitial pressure, decreases the blood volume and superficial venous pressure, and improves venous return. 8
Types and classification of compression hosiery
Compression hosiery consists of elasticated socks, stockings and tights. These can come in either thigh or knee length. There is currently no evidence for which length of stocking is more effective 9 and decisions about which of these are used will usually be made on the basis of patient and/or clinician preferences.
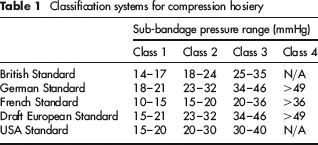
Compression hosiery is classified on the basis of the pressure that is applied beneath the bandage at the ankle. These sub-bandage pressures are determined by three factors. 10 First, the material the stocking is made from in terms of its stiffness and elasticity. Second, the size and shape of the leg to which the stocking is being applied. Third, the activity being undertaken by the person – whether they are lying down, sitting, walking or running. The sub-bandage pressures were measured by the manufacturers based on in vitro measurements, but concern has been expressed regarding whether these measurements bear any relation to the pressures applied within real-life situations. 10
There are currently five different classifications in use for compression hosiery 11 which have between three and four different classes:
British Standard – BS:6612; 1985;
German Standard – RAL-GZ 387; 1987;
French Standard – ASQUAL;
A draft European Standard – ENV 12718; 2001;
USA Standard.
These different classifications systems differ in terms of the thresholds applied for Classes 1–3. The classes and pressure ranges are shown in Table 1. The aim of the draft European Standard was to try and ensure a consistency within the European Union, but was abandoned due to a lack of consensus. 12 Concern has been expressed in the past about the potential for confusion the use of different systems can cause. 13 It was highlighted in the UK that hospitals and community supply stockings based on different standards and different materials. Hospitals use the European Standard while community pharmacists use the British Standard.
Classification systems for compression hosiery
Assessment for suitability for compression hosiery
The application of compression hosiery is not without any hazards. Badly fitting stockings and inadequate assessment can lead to severe problems. 14 Poorly fitting stockings can cause pressure necrosis, and, if stockings are applied to a limb with impaired arterial flow, it can lead to inadequate perfusion, necrosis and possible amputation. 13 Other problems can be caused if the stocking is too long – as it can roll down and create a tourniquet effect – or if the hosiery material results in contact dermatitis. 11
In order to minimize the potential for harm, local and national guidelines have been produced which detail the necessary training for clinicians, and the assessment and care of patients wearing compression.10,15–17 The guidelines specify that only those who have undergone appropriate training should assess patients for compression hosiery, and, prior to its application, a clinical history and ankle brachial pressure index (ABPI) should be performed in order to exclude arterial disease.
Issues surrounding compression hosiery for varicose veins
In spite of the widespread use of compression hosiery, there still seem to be gaps and questions in relation to their use in the treatment of varicose veins:9,17
What is the mechanism of action of compression hosiery?
Which is the best method of measuring the effects of compression?
Compression pressures for hosiery are measured in vitro, but in vivo these pressures may not be consistent between patients, positions and activities;
Are calf or thigh length stockings better?
There are variations in the strength of compression stockings applied to patients with varicose veins and it is not clear what level of compression is ideal;
Does compression hosiery have any effect on symptoms related to varicose veins?
Does compression hosiery have any benefit in slowing the progression or in the prevention of varicose veins?
This review seeks to examine the current evidence regarding the effectiveness of compression hosiery in the treatment of varicose veins and to examine these questions.
Methods
Prospective randomized controlled trials (RCTs) evaluating compression hosiery in the treatment of varicose veins were sought. Where RCTs were unavailable, evidence from lower down the hierarchy of evidence was included. Studies were included if they evaluated the application of compression to patients with a diagnosis of varicose veins.
Full-text articles of studies were identified using the search strategy outlined below. Decisions regarding inclusion were based on review of the title or abstract and those citations that may have evaluated compression for varicose veins obtained for more detailed review. Inclusion or exclusion of trials was decided by two reviewers acting independently. Trials were considered for inclusion if they evaluated the use of compression therapy for uncomplicated varicose veins.
Any disagreements on inclusion or exclusion were adjudicated by a third reviewer. Where data were missing authors were contacted to provide additional detail.
The quality of the RCTs were assessed on the basis of factors that have been widely recognized in the minimization of bias and confounding. These were:
Comparability of treatment groups at baseline;
Analysis of outcomes on an intention-to-treat basis;
Completeness of follow-up;
The blinding and objectivity of outcome assessment;
The appropriateness and completeness of statistical analysis of results.
All analysis was on an intention-to-treat basis with withdrawals and losses to follow-up being assumed to be treatment failures.
For other types of studies a narrative review was undertaken.
Search strategy for identification of studies
Searching was undertaken to identify trials that evaluated the use of compression hosiery in the treatment of varicose veins. Computerized searches of the major electronic databases including Medline, Cinahl and Embase. In addition, hand-searching of relevant journals, using the search strategy described by the Cochrane Peripheral Vascular Diseases Group, was performed. The searches were originally conducted during May 2008, although the major database searches were re-run in July 2008.
Twelve electronic bibliographic databases were searched, covering biomedical, science, social science, health economic and grey literature (including current research). In addition, searches of 18 internet-based health services research-related resources were undertaken and the reference lists of relevant articles checked.
Where possible (e.g. in the smaller databases), searches were not restricted by publication type or study design. However, methodological filters aimed at identifying guidelines, systematic reviews and clinical trials were applied in the larger databases, such as MEDLINE. Date and language restrictions were not used. The electronic bibliographic databases searched are listed below:
AMED;
Best evidence;
Biological abstracts;
Cochrane-Controlled Trials Register (CCTR);
Cochrane Database of Systematic Reviews (CDSR);
EMBASE;
Medline;
NHS Database of Assessments of Reviews of Effectiveness (NHS DARE);
NHS Economic Evaluations Database (NHS EED);
NHS Health Technology Assessment (NHS HTA);
PubMed (last 180 days);
Science Citation Index.
Other sources searched:
Agency for Healthcare Research and Quality (AHRQ);
Bandolier;
Canadian Co-ordinating Centre for Health Technology Assessment (CCOHTA);
Current Controlled Trials (CCT);
CenterWatch Trials Register;
ClinicalTrials.gov, NIH Clinical Trials Database;
COIN (Department of Health Circulars);
Current Research in Britain (CRiB);
Department of Health;
Health Services/Technology Assessment Text (HSTAT), USA National Library of Medicine;
Medical Research Council (MRC) Funded Projects Database;
National Guideline Clearinghouse;
National Research Register;
National Co-ordinating Centre for Health Technology Assessment (NCCHTA);
NHS Centre for Reviews and Dissemination (NHS CRD), University of York;
NHS R&D Programmes;
Scottish Intercollegiate Guidelines Network (SIGN);
Turning Research into Practice (TRIP) Database.
Search strategy used in the major databases:
#1 varicose veins/all subheadings;
#2 explode varicose veins/all subheadings;
#3 (varicose ADJ vein$) in ti, ab;
#4 #1 or #2 or #3;
#5 explode compression hosiery/ all subheading;
#6 (compression ADJ stocking$) in ti, ab;
#7 (compression ADJ hosiery) in ti, ab;
#8 (support ADJ stocking$);
#9 (support ADJ hosiery);
#10 #5 or #6 or #7 or #8 or #9;
#11 #4 and #10;
Description of studies
The stages of the process of undertaking the review using the QUOROM statement 18 as a basis are shown below:
Three hundred and seventy-nine citations describing potentially eligible studies were identified from the searches;
Five citations were excluded as they were duplicates;
One hundred and eighty-three were excluded as they evaluated the use of compression for venous ulcers and not varicose veins;
Ninety-six were excluded as they were review articles of either venous ulceration, deep vein thrombosis (DVT) or phlebitis;
Thirty-one were excluded as they evaluated the use of compression after surgery or sclerotherapy;
Five were excluded as they evaluated drugs;
Three were excluded as they evaluated compression after DVT;
One was excluded as it evaluated compression in post-phlebitic limbs;
A total of 55 citations were, therefore, potentially suitable for inclusion and were retrieved for full inspection;
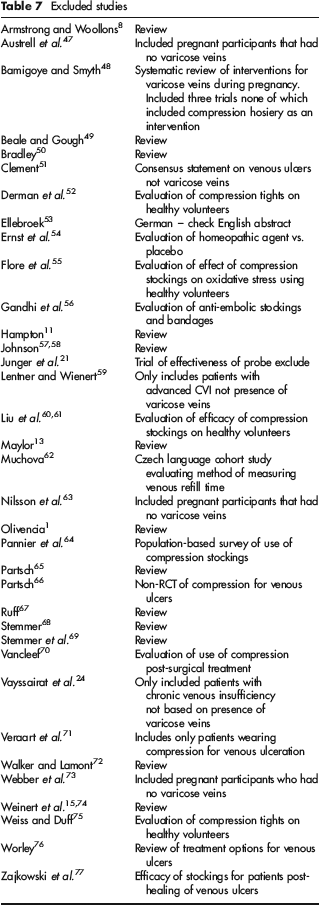
A total of 28 citations were excluded after review (Table 7);
One additional study was found to be a duplicate and one of the guidelines was published in two parts;
The table of excluded studies summarizes the reasons for exclusion;
A total of 23 clinical studies and two guidelines were included in the review.
The clinical studies were conducted in the UK (n = 12), USA (n = 3), Germany (n = 2), Switzerland (n = 2), Australia (n = 1), France (n = 1), Japan (n = 1) and Sweden (n = 1).
The included studies were categorized into five groups:
Studies that evaluated the efficacy of compression therapies (n = 15);
Studies that evaluated the use of compression hosiery compared with other treatments (n = 4);
Studies that evaluated compliance with compression therapy (n = 2);
Studies that evaluated compression for varicose veins in pregnancy (n = 2);
Guidelines and consensus statements (n = 3).
(1) Studies that evaluated the efficacy of compression therapies
A total of 15 studies were found which evaluated the efficacy of compression hosiery in patients with varicose veins. The majority of the trials (11/15) were non-randomized comparative studies. The other studies included one systematic review 19 and three randomized trials.4,20,21
Systematic reviews and RCTs:
Amsler and Butler 19 conducted a systematic review and meta-analysis of RCTs that compared stockings exerting an ankle pressure of 10–20 mmHg with those exerting a pressure of greater than 20 mmHg for mild chronic venous insufficiency. There was no separate reporting of those trials that specifically included the presence of varicose veins. Trials were included if they included a control group that had no compression or placebo stocking. No details are given of the search strategy and time period searched. They reported that they had problems accessing studies as many were not indexed on Medline or other electronic databases.
Eleven trials fulfilled their inclusion criteria. Four of these were in healthy volunteers and two evaluated compression post-varicose vein surgery. One trial was concerned with the prevention of venous thrombosis. This means that four trials may have included patients with varicose veins. However, of these, two were not included in the meta-analysis due to poor reporting22,23 and two were written in French.24,25 Details of Benigni et al. 22 are given below.
The primary outcome measures included in the review were pain/discomfort, symptoms and leg oedema. The quality of data was highlighted as being poor. Three studies out of the 11 provided sufficient data for pooled analysis and showed significant benefit of compression compared with no compression (standard mean difference −1.01 CI −0.83, −1.2; P < 0.0001). No difference between low and high compression was found in terms of alleviating symptoms (OR 0.99; CI 0.56, 1.74; P = 0.97);
The study by Benigni et al. 22 was a randomized double blind cross-over study conducted in France. No details of randomization procedure were reported. One hundred and twenty-five female patients with symptoms of chronic venous disease (CVD) based on the clinical, aetiological, anatomical and pathological elements classification C1–C3 were recruited to the trial, with 114 analysed. Participants were randomized to either Class 1 compression (10–15 mmHg) (n = 60) or a placebo stocking (n = 65). Patients wore their allocated stocking for 14 days and then had a one week washout period before crossing-over and wearing the other type of stocking. The primary outcome was pain measured by a visual analogue scale (VAS). Other outcomes included subjective symptoms and leg volume. A total of 111 patients completed the study. Pain scores were lower in those wearing the Class 1 stocking compared with placebo (P = 0.024). Improvement in symptoms such as heaviness, cramps and swelling of ankles also occurred in the group wearing the Class 1 stocking. No differences were seen in leg volumes;
In the study by Chant et al. 20 a RCT trial was conducted in the UK. No details of randomization procedures were reported. One hundred and four patients awaiting surgery for treatment of varicose veins were randomized between Class 2 (30–40 mmHg) and Class 3 (40–50 mmHg) compression stockings. Participants wore the stockings for six weeks. The primary outcome was leg symptoms. Both groups reported improvement in their symptoms. The conclusion of the trial was that higher compression can be tolerated;
Jones et al.‘s 21 was a randomized crossover trial conducted in the UK. No details of randomization procedure were reported. Ten patients with superficial varicose veins plus 10 health volunteers and 10 patients with a post-phlebitic limb were randomized between two types of compression stockings – Eesiness (20 mmHg) and Sigvaris (30–40 mmHg). The primary outcome was the competence of the superficial and deep venous system measured by foot volumetry and Na 24 subcutaneous tissue clearance. A secondary outcome was the acceptability of the stocking. The group with varicose veins showed significant improvement in ‘restitution time’ (T1/2 = time in seconds for refilling of half the volume expelled from the foot during exercise) and in Na 24 clearance for the Sigvaris stocking at rest. Preference was expressed for the Sigvaris stocking. The Sigvaris stockings were provided by the manufacturer.
Non-randomized studies:
The study by Christopolous et al., 26 based in the UK, examined 132 limbs in 114 patients with CVI, 32 (40 limbs) of whom had primary varicose veins. A group of 20 healthy volunteers were used as a comparative group. Air plethysmography was used to examine arterial inflow and venous haemodynamics. Baseline results were compared 30 minutes after the application of ‘elastic compression’ – no details of length or type were reported. Uncomplicated primary varicose veins showed no increased arterial flow compared with those who had ulceration or skin changes. Elastic compression reduced skin flow by 45% after application;
The study by Fronek et al., 27 conducted in the USA, examined 45 limbs in 29 people. Eight were healthy volunteers, 10 had telangiectatic veins and 11 had primary varicose veins. Photoplethysmography was used to examine venous haemodynamics in terms of displacement of blood volume in the legs. All of the different groups showed significant increases in veno-muscular efficiency (exercise displacement volume/tilt displacement volume). In the varicose vein group this increased from 28% to 44% (P < 0.01) after application of compression hosiery;
The study by Hirai et al. 28 was a study conducted in Japan that examined 20 limbs in 14 female patients with varicose veins; a group of 14 female healthy volunteers were used as a comparison. Oedema was measured using strain gauge plethysmography pre- and post-application of four types of compression hosiery: 8 mmHg, 14 mmHg, 22 mmHg and 30–40 mmHg. Significantly smaller increases in foot volume were found in varicose vein patients wearing stockings compared with when not wearing stockings. None of the different types of stocking showed any difference in volume increases for the control subjects;
In the study by Ibeguna et al., 29 conducted in the UK, 20 limbs in 19 female patients who had moderate varicose veins showing some skin changes was examined. Air-plethysmography was used to examine venous haemodynamics pre- and post-application of three types of compression stocking: 7, 10 and 14 mmHg. Statistically significant reduction were seen in venous reflux (P < 0.0002) and calf muscle pump (P < 0.03) after application of all grades of stocking. Venous volume was reduced only for 10 mmHg and 14 mmHg (P < 0.05) stockings. Significant changes in ejection fractions were found only in the 14 mmHg stocking group;
Labropoulos et al.'s 3 was a non-randomized comparative study conducted in the UK that examined 20 patients with grade 2 CVI. Air plethysmography was used to examine venous haemodynamics in two groups. Group 1 (n = 9) wore compression stockings for four weeks and measurements were performed before, during and one day after removal of the stocking. Group 2 (n = 11) wore the stockings for the same amount of time, but measurements were taken before, during and immediately after removal of the stocking. Application of compression stockings improved reflux and residual volume fraction for both groups. Immediately after removal of stockings, all measurements regressed to baseline values. The study concluded that the benefits of stockings are only provided while they are worn;
The study by Leon et al. 30 was a nonrandomized study conducted in the UK that aimed to examine the effect of compression stockings on the elasticity of varicose veins. Twenty-nine patients with ‘venous problems’ referred to a venous clinic were examined using duplex scanning, photoplethysmography and by calculating the elastic modulus – using strain gauge plethysmography with venous pressure measurements. Nineteen of the patients had superficial venous incompetence and 10 had deep venous incompetence. Measurements were taken before and after four weeks of wearing thigh length compression stockings. No correlation between changes in elasticity and superficial or deep venous incompetence were found. An increase in elasticity was found after four weeks of wearing compression stockings. A subgroup of patients who did not respond to compression treatment was found for those whose venous disease had been present for more than 10 years, illustrating a negative linear relationship (r = 0.88) between increase in elasticity and duration of the disease;
Lord and Hamilton's 31 was a nonrandomized comparative study conducted in Australia. The study compared normal legs (n = 17) with legs where varicose veins were present (n = 13). Venous duplex was used to measure the internal diameters of the superficial and deep veins of the calf pre- and post-application of Class 2 compression stockings in the lying and standing positions. Compression stockings were found to compress both superficial and deep veins when supine, but not when standing. In the varicose vein group, the LSV was constricted by the upper band of the stocking. It was postulated that this might explain an increased incidence of superficial thrombosis when compression stockings are worn;
The study by Müller-Buhl et al., 32 conducted in Germany, examined a group of patients (n = 46) who had unilateral LSV varicose veins. The main outcome measured was change in venous blood volume between upright and supine positions using photoplethysmography pre-wearing and one week post-wearing thigh length stockings for seven days. The study found that blood volume increased (P < 0.01) in both normal and varicose legs changing from supine to upright. Varicose legs had greater blood volume than normal legs (P < 0.01). Application of compression hosiery reduced blood volume in both positions (P < 0.001). The wearing of compression hosiery for eight hours or seven days resulted in no significant difference in blood volume;
The study by Norgren's 33 was a nonrandomized study conducted in Sweden that examined three different types of Class 2 (25–32 mmHg) compression stockings for a group (n = 15) of patients with varicosities. Venous haemodynamics were measured using foot volumetry and photoplethysmography Foot volumetry showed increase in venous emptying for only two types of stockings, while photoplethysmography showed it for all three of types of stockings. None of the methods showed any significant increase in refilling time or reduction in reflux;
The study by Pierson et al.‘s 5 was a nonrandomized comparative study conducted in the USA. A group of healthy volunteers (n = 30) were compared with patients who had symptoms related to swelling of the lower leg (n = 73) after wearing Class 2 (24 mmHg) thigh length compression stockings for one week. The patient group consisted of those with uncomplicated varicose veins (n = 20), leg pain with no visible cause (n = 65) and other conditions (n = 35) such as lymphoedema, CVI and phlebitis. The primary outcome measure was a change in leg volume measured by water displacement and leg circumference. Application of compression stockings resulted in a decrease in leg volume and circumference for symptomatic patients, but not normal volunteers. Symptomatic patients also reported decreased pain after wearing compression for one week (P < 0.001);
In the non-randomized study by Szendro et al., 34 a group (n = 10) of patients with moderate primary varicose veins showing skin changes were examined. Venous haemodynamics were measured using strain gauge and air plethysmography before and after wearing thigh length compression stockings (30 mmHg) for six weeks. The primary outcome was changes in the pressure-volume relationship of the leg and calculation of the elastic modulus. Wearing stockings was found to improve the pressure-volume curves. Those patients with early to moderate superficial incompetence were found to benefit more, in terms of the restoration of venous wall elasticity, from the application of compression stockings than those with severe disease.
(2) Studies that evaluated the use of compression hosiery compared to other treatments
The study by Anderson et al. 35 was a randomized controlled crossover trial conducted in the UK which included n = 72 patients on a surgical waiting list for venous surgery. The patients were randomly allocated to either stocking (30–40 mmHg) versus Paroven (a Rutoside drug) or placebo versus Paroven plus stocking. The patients had their allocated treatment for four weeks and then crossed-over to the other treatment. The primary outcome measure was subjective symptoms, including pain, heaviness, itching and swelling, measured by VAS. No statistically significant differences were found following any of the four treatments, but the authors concluded that drug plus stocking was better than either treatment alone;
Hartmann et al.‘s 36 study was a randomized controlled trial conducted in Germany. Patients who had varicose veins were randomly allocated to either no treatment (n = 12) or exercise plus compression stocking (n = 12). The treatment group exercised twice a week under the direction of a physiotherapist for 60 minutes while wearing compression stockings (30 mmHg). The primary outcome measures were changes in venous capacity and venous refill time measured by strain-gauge plethysmography. A secondary outcome measure was patient-reported symptom reduction measured using a ‘standardized questionnaire’. The decrease in venous capacity in the treatment group was greater than the control group (P < 0.005) and the venous refill time also increased more for this group (P < 0.001). The treatment group also reported an improvement in their symptoms;
Michaels et al.‘s 37 was a cost-effectiveness study conducted in the UK. The trial included only those with primary varicose veins and had three arms: sclerotherapy versus conservative treatment (n = 34), sclerotherapy versus surgery (n = 77) and surgery versus conservative treatment (n = 246). Conservative treatment was defined as life style advice and urging to wear compression hosiery. No details were reported on those who wore compression and those who did not. Patients were randomized within these arms using a telephone randomization service. The primary outcome measures were cost-effectiveness, health-related quality of life (HRQoL) and symptoms. The trial reported that only the surgery versus conservative treatment arm was large enough to provide clear results. Surgery showed significant improvements compared with conservative treatment at one year in HRQoL and symptoms;
The study by Tisi and Beverley 38 was a systematic review and meta-analysis. Although it concentrated on injection sclerotherapy it also included a comparison of sclerotherapy versus compression stockings. The review found only one RCT conducted in South Africa in 1973. 39 This randomized 101 pregnant female patients with primary or recurrent varicose veins to either sclerotherapy or compression stockings. The primary outcome measure was symptomatic improvement. Sclerotherapy was more effective than compression stockings in terms of improvement in symptoms and cosmesis (RR 1.61; CI 1.19–2.18).
(3) Studies evaluating compliance with compression hosiery for varicose vein patients
Randomized controlled trials:
Chant et al. 40 was a randomized study conducted in the UK that randomly allocated 66 patients with varicose veins on the surgical waiting list to two types of compression stockings. One group (n = 33) wore Sigvaris stocking and the other (n = 33) Medi Plus. No details of randomization procedures are reported. The primary outcome measure was compliance with wearing the stocking determined by home visits at random around six weeks post-randomization to check whether the patient was wearing the stocking. There was a high dropout rate with 33% (n = 22) failing to collect their allocated stocking. A further four withdrew (n = 1 in Sigvaris and n = 3 in Medi Plus) as they had their surgery prior to their home visit, resulting in a 39% withdrawal rate. No significant difference in terms of stocking type and gender were found between those who elected to wear stockings and those who did not. Patients who complied with wearing stockings tended to be older (P = 0.002).
Non-randomized studies:
The study by Raju et al.‘s 41 was a retrospective study, conducted in the USA, of a cohort (n = 3144) of patients referred to a specialist venous clinic with a diagnosis of CVI. The patients had varicose veins ranging from ‘simple’ to ‘more complex, involving the deep venous system’. The primary outcome examined was patient's reported compliance with wearing compression hosiery based on the patient's initial clinical evaluation after referral to the venous clinic. Only 37% reported full or partial compliance with wearing compression hosiery, the remainder did not use compression or abandoned its use after an initial trial period. Compliance was reported as being 50% (n = 2437) in those who had a history of DVT (P < 0.0001) and a longer duration of symptoms (44% for those with a history of over 10 years of problems compared with 34% in the one to five year group, P < 0.015).
(4) Studies evaluating interventions for varicose veins in pregnancy
Randomized controlled trials:
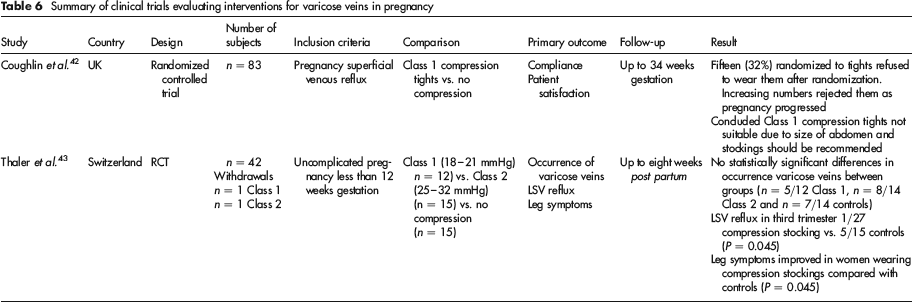
Coughlin et al.‘s 43 was a RCT, undertaken in the UK, that examined the acceptability and usage of prescribed compression hosiery for pregnant women with varicose veins (n = 83). The comparison was between those allocated to wear Class 1 compression tights (n = 46) and those not wearing compression tights (n = 37). No details of randomization procedures were reported. No data were provided on the group allocated not to wear hosiery. Data on the hosiery group's compliance were reported. After initial randomization, 32% (n = 15) refused to wear the tights. Increasing numbers then rejected them as pregnancy progressed. The study concluded that Class 1 compression tights are not suitable due to size of abdomen as pregnancy progresses and that stockings should be recommended;
Thaler et al.‘s 43 , was a RCT, undertaken in Switzerland, that randomized pregnant women between wearing Class 1 (18–21 mmHg) compression stockings (n = 12), Class 2 (25–32 mmHg) stockings (n = 15) and not wearing stockings (n = 15). Women were stratified on the basis of presence or absence of varicose changes. The primary outcome was the occurrence of varicose veins. No statistically significant differences in occurrence rates for varicose veins were found between the groups. Leg symptoms improved in women wearing both types of compression stockings when compared with controls (P = 0.045). Although no details of sponsorship are provided, it was reported that the randomization was performed by the stocking manufacturers (Ganozzi SA, Switzerland).
(5) Guidelines and consensus statements for the use of compression hosiery for varicose veins
American Venous Forum, American College of Phlebology, European Venous Forum, International Union of Angiology guidelines for the management of chronic venous disorders of the leg.17,44
The guidelines aimed to cover all aspects of CVI including varicose veins, lymphoedema and venous ulceration. Evidence from both randomized and non-randomized trials, and consensus statements were reviewed. No details of the search strategy were reported. Evidence was graded based on level of evidence (Level 1–3) and grade of recommendation (A-C). Level 1 and Grade A recommendations were those based on RCTs, where the results were clear cut. A general review of the evidence was given in the paper detailing all of the CVI symptoms 44 and a more specific paper that concentrated on compression therapy for venous and lymphatic disease was also published. 17 In the assessment of the effectiveness of therapies related to compression hosiery, they endorsed the recommendations of a consensus meeting 45 that water displacement volumetry should be viewed as the gold standard to prove and compare efficacy of treatments to reduce oedema. The authors highlight a ‘paucity’ of methods that can be used in the selection and application of compression therapy. No trials directly related to the use of compression hosiery in the treatment of varicose veins were cited. However, only one paper that compared physical therapy and compression was related to varicose veins. 36 The paper was graded at level C. The other papers examined evaluated compression postsurgery and sclerotherapy, use of drug treatments and compression, and pneumatic compression that are outside the remit of this current review.
The development of multicomponent fabrics that offer a higher grade of support on ambulation at a much lower resting present mean that there is a need for clinical trials to assess their effectiveness. In addition, the need for RCTs to assess the clinical efficacy of stockings for relief of symptoms, length of stocking and use of compression post-sclerotherapy and surgery were also emphasized. The evidence that was found related to the effectiveness of compression hosiery was limited and related to their use in the treatment of venous ulcers and DVTs;
International Union of Phlebology guidelines on evidence-based compression therapy 46 This was a position statement rather than a review of the evidence. The paper outlined the criteria that should be used in the evaluation of the effectiveness of compression therapy, and highlighted gaps in the current evidence. The experts then reviewed and commented on the level of evidence and the studies classified as either A, large RCTs or meta-analysis; B, RCT in smaller populations or one RCT only; or C, observational studies or consensus documents. The studies were then commented upon, but no context or recommendations were given. No details were reported regarding the search strategy and methods of appraisal. No additional studies were found that were not also identified by the search strategy used for this paper. For large asymptomatic varicose veins, the paper cited was Hartman et al., 36 which compared physiotherapy and compression hosiery. This was classified as Level C and flaws identified in terms of the small sample size and not providing data on long-term outcomes. The paper cited for large symptomatic varicose veins was Anderson et al., 35 which compared Paroven (a Rutoside drug) and compression hosiery. It was classified as Level C and criticized for having no washout period between the crossover treatments. The final paper reviewed within the area of the current review was Thaler et al. 43 It was classified as level B, but was criticized for poor reporting of stocking type and small sample size;
Wounds UK best practice guidelines for compression hosiery. 10 The guidelines concentrate on the use of compression hosiery in the treatment and prevention of venous leg ulcers and lymphoedema, but the proposals can also be applied to the application of compression in the treatment of varicose veins. They were sponsored by one of the hosiery manufacturers, Scholl. No details are provided regarding search strategy review methods, assessment or level of the evidence included in the guidelines. The guidelines make recommendations regarding training, assessment, application, wear-time and patient education in relation to compression hosiery, which are outlined below:
Training. Health professionals applying compression hosiery have the appropriate knowledge and training. In order to do this they should be able to demonstrate attendance of training in the selection, measurement, application and fitting of compression hosiery;
Assessment. Prior to application of compression patients must be assessed for suitability of compression. This should include Doppler ABPI assessment on a yearly basis in addition to clinical history. Those patients with a reducing ABPI should have ‘more regular checks’;
Product selection. The prerequisite for effective and successful management using compression hosiery is an accurate fit. Accurate assessment of limb dimensions and shape should be undertaken and documented. Health professionals should be aware that there may be variations in terms of the manufacturers recommendations for the measurement of legs;
Application. The first application of compression hosiery should be supervised by a competent practitioner who has been trained in its application. Any difficulties should be identified and addressed, and application aids provided if necessary. The demonstration and outcome should be documented. Newly fitting hosiery should be checked one week after fitting;
Wear-time. Patients should remove the hosiery at night and reapply first thing in the morning. Extended wear-times may lead to poor skin condition. Generally patients should be advised that compression hosiery needs to be worn for life. Patients should be reviewed and re-measured every three to six months or if there is any significant change in limb size;
Patient education. Patients and carers should be provided with appropriate information in an accessible format. They should understand the importance and benefits of wearing compression hosiery.
Methodological quality of included studies
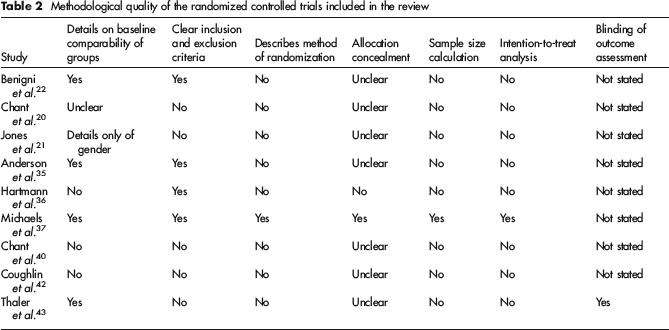
The search strategy identified a total of 25 studies that examined the use of compression hosiery in the treatment of varicose veins. A total of 11 were randomized controlled trials or systematic reviews, 12 nonrandomized studies and two guidelines/consensus statements. Details of the methodological quality of the nine RCTs are given in Table 2.
Methodological quality of the randomized controlled trials included in the review
Randomized trials or systematic reviews were found that investigated the areas of efficacy of compression hosiery19–22 (n = 4), compression hosiery versus other treatments37,38 (n = 2), compliance 40 (n = 1) and use of compression hosiery in pregnancy for varicose veins42,43 (n = 2).
Efficacy of compression hosiery
A total of 15 studies were found that evaluated the efficacy of compression hosiery. Only four of these were either RCTs or systematic reviews. In this group one of the publications was a systematic review and meta-analysis. 19 However, it concentrated on the use of hosiery for all of the manifestations of CVI ranging from aching through varicose veins to ulceration. There was no separate reporting of results based on the presence of varicose veins. No details were reported of the search strategy, databases searched, limitations or time period searched. The review identified 11 trials, but only four of these could have included patients with varicose veins (Table 3).
Summary of clinical trials evaluating efficacy of compression hosiery
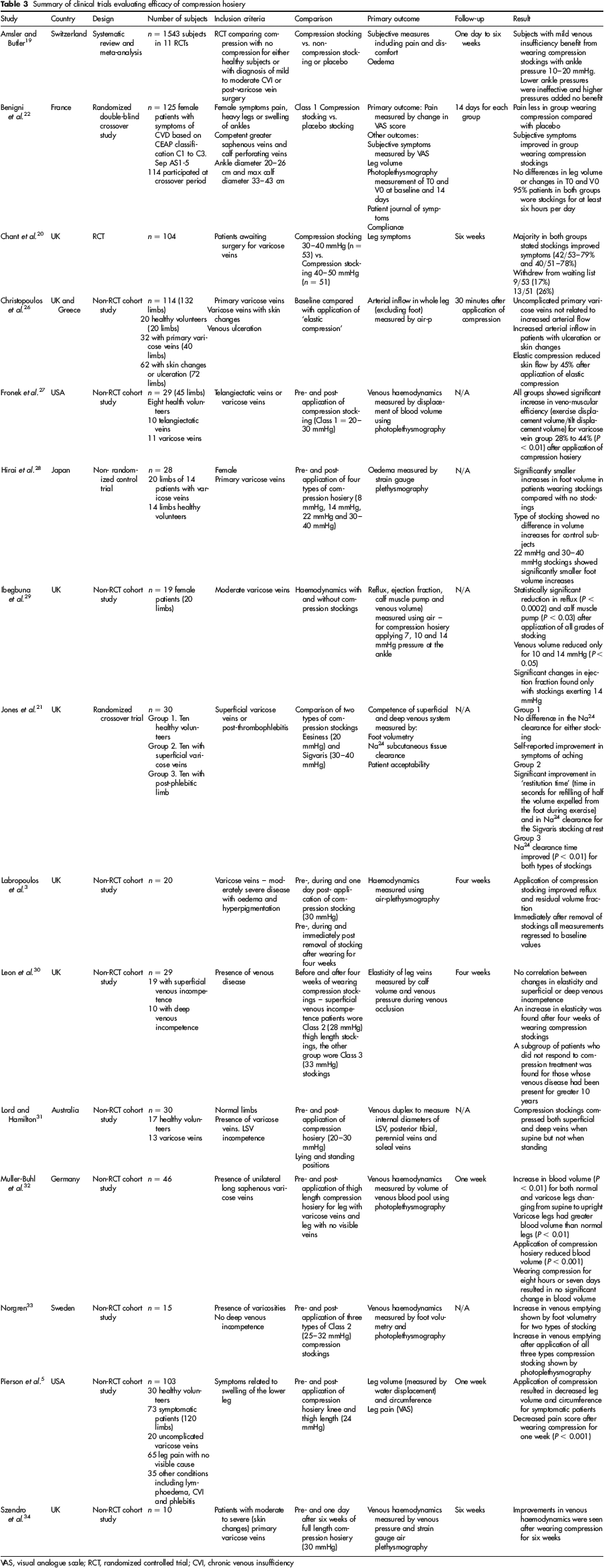
VAS, visual analogue scale; RCT, randomized controlled trial; CVI, chronic venous insufficiency
Two of the three RCTs were crossover trials:21,22 one 22 compared Class 1 and not wearing a stocking, and the other compared two types of stockings. The remaining trial 20 compared different classes of compression. None of the RCTs reported details of randomization procedure or sample size calculation. The primary outcome measure for two of the trials20,22 was a change in symptoms based on VAS, while the other examined venous haemodynamics.
The remaining 11 non-randomized studies varied in terms of inclusion criteria, size, methodology and outcome. Five of the studies26–29,31 used the limb as the basis of investigation and the remainder the patient. Three of the studies included patients who had other problems – such as oedema, leg symptoms and telangiectatic veins – in addition to patients with varicose veins. The majority of the studies (n = 7) used either photoplethysmography27,30,32,33 (n = 3) or air plethysmography3,26,29,34 (n =5) to examine venous haemodynamics, but one 31 used venous Duplex. Two others examined oedema using strain gauge plethysmography and water displacement.
Although the majority of the studies aimed to examine venous haemodynamics, there were variations in the outcomes evaluated. The application of compression hosiery was shown to:
The effectiveness of compression hosiery compared with other treatments
Four studies35–38 were found that included a comparison of compression hosiery with other treatments (Table 4). However, all had limitations in terms of the applicability to varicose veins.
Summary of trials comparing compression hosiery with other treatments for varicose veins
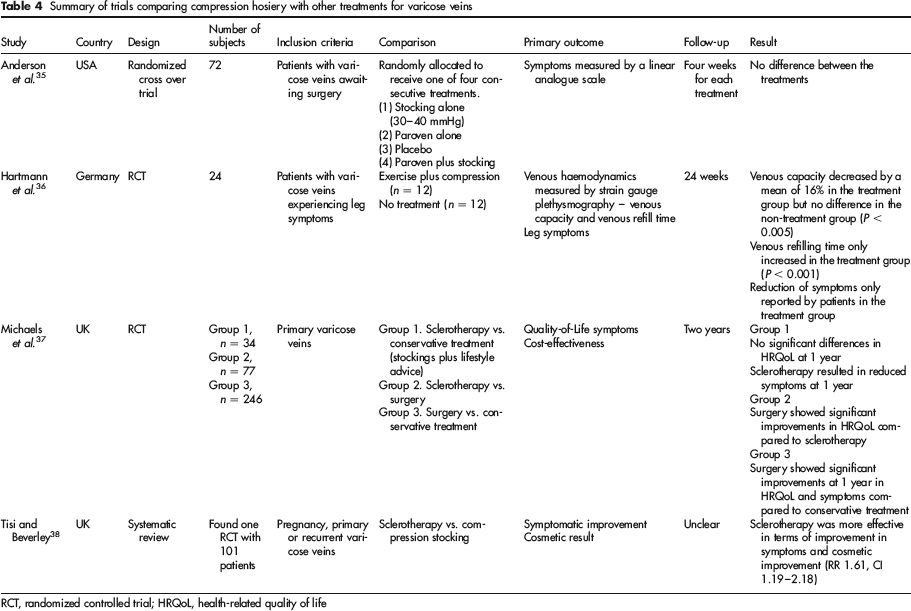
RCT, randomized controlled trial; HRQoL, health-related quality of life
Two RCTs were found that directly compared compression hosiery with other treatments. One 35 compared hosiery with a drug treatment, Paroven, which is an oxerutin that works by reducing capillary leakage. However, the treatment periods were limited to only four weeks and as reported by Partsch et al. 45 there was no washout period between treatments and there were no baseline assessments prior to commencement of the new treatment. The other study 36 consisted of only 24 participants. No details were provided regarding whether the non-treatment group wore stockings. There could also be a measurement error in terms of symptomatic improvement due to the Hawthorne effect in the treatment group.
The remaining two studies were not directly applicable. One study 37 was a cost-effectiveness and RCT that had three arms, two of which compared conservative treatment with surgical or sclerotherapy. However, the conservative treatment consisted of ‘life-style advice and recommendations to wear compression hosiery’. No details were provided regarding the type or strength of stocking or the number of patients complying with the advice. The other study 38 was a systematic review and meta-analysis. The main focus of the review was compression post-injection sclerotherapy, but it did include studies that compared sclerotherapy and compression hosiery. Only one study was found for this comparison, undertaken in 1973 and this was not applicable to the whole population with varicose veins as it only included pregnant women.
Compliance with compression hosiery
One RCT 40 and one non-randomized study 41 were found that examined the compliance of patients in wearing compression hosiery (Table 5).
Summary of clinical trials evaluating compliance with compression hosiery for varicose vein patients
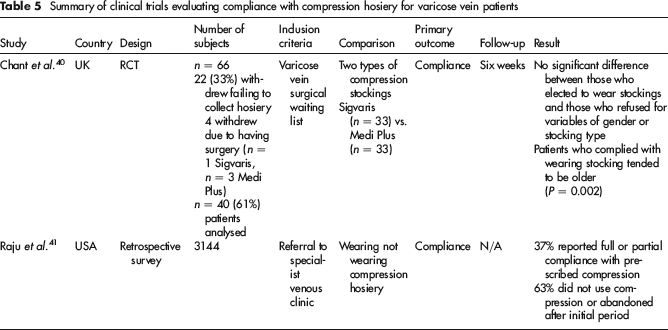
The RCT compared two types of stockings and not stockings versus no stockings. It provided no details of randomization procedure, sample size calculation or blinding of patients or assessors. It also had a relatively small sample size of 66 patients and had a high withdrawal rate of 39% (n = 26).
The non-randomized study was a retrospective analysis of referrals to a specialist venous centre. The primary outcome was patient-reported compliance with wearing compression hosiery and so could mean that the findings were not a true reflection of actual compliance.
The use of compression hosiery in pregnancy for varicose veins
Two RCTs42,43 were found that examined the use of compression hosiery in pregnant women (Table 6). Neither of the studies detailed the method of randomization or sample size calculations. Thaler et al. 43 did report that assessment was blinded. Coughlin et al. reported a high withdrawal rate of 32% (n = 15) at baseline and then ‘increasing numbers’ refused to wear them as their pregnancy progressed.
Summary of clinical trials evaluating interventions for varicose veins in pregnancy
Guidelines and consensus statements
Two guidelines were found that included the use of compression hosiery for varicose veins. The third paper within this section 46 was a limited review paper.
One of the guidelines was published in two papers17,44 and was an international collaboration between experts and societies based in Europe and the USA. The consensus statement covered the whole spectrum of chronic venous disorders of the lower leg and so large sections were not relevant to the current review. The evidence was graded and critically analysed and consensus achieved based on e-mail responses. No details of the search strategy were reported.
The other 10 detailed the use of compression hosiery and appeared to be targeted at venous ulceration and lymphoedema. No details were reported of the search strategy or review and appraisal methods.
Discussion
Despite the widespread use of compression hosiery for varicose veins, the evidence for their effectiveness in the case of varicose veins was limited. The majority of studies were small, non-randomized studies. Where higher level evidence was available this was often of poor quality or not applicable to varicose veins. Although one RCT 22 was found that compared wearing compression hosiery with wearing a placebo stocking, the sample was heterogeneous and included patients who had symptoms but no varicose veins. Another limitation was that its primary outcome was subjective and measured using a VAS. The hosiery applied was also Class 1 and some authors have suggested that higher compression is needed. 20 Additional trials within this area are likely to be difficult due to the widespread use of compression therapy and the expectation by patients for some sort of intervention to treat their varicose veins. 37
Another challenge for their use in this area is that patients are extremely reluctant to wear them. One of the studies 41 included in the review reported that only 37% of patients were complying or partially complying with wearing their compression hosiery. The reasons cited for not wearing hosiery included that they did not work, felt too tight and made their legs too hot. The patients who seemed to comply tended to be older or had endured their symptoms for longer. This would seem to suggest that there is limited benefit in compression being the first line of treatment or that their use needs to be targeted more effectively.
Compression hosiery has been shown in nonrandomized comparative trials to affect venous haemodynamics in terms of increasing the veno-muscular efficiency, 27 reducing venous reflux 29 and reducing leg oedema. 28 Studies have also shown that the pressure applied by the stockings vary depending on position and activity31,32
The evidence regarding the class of compression needed for the effective management of varicose veins was mixed. Some studies showed that Class 1 had benefit,22,27 while other studies have shown that Class 1 stockings do not compress the veins sufficiently 31 and others have only included Class 2 stockings in any comparisons. No data were found to evaluate whether calf or thigh length stockings were better.
The effect of compression stockings on the symptoms of varicose veins was equivocal. Although some of the studies did report an improvement in leg symptoms,5,22,36 there were limitations in that it can be difficult to accurately measure subjective symptoms, only those that chose to wear compression were included and the mere act of the application of compression and intervention may make patients feel better.
The benefits of wearing compression in order to slow the progression, or prevent the occurrence of, further varicose veins cannot be supported by the current published evidence. Only one trial 43 was found that evaluated this outcome. The trial was small in size, only included pregnant women and found no difference between wearing and not wearing compression hosiery.
Excluded studies
The incorrect application of compression hosiery can have serious consequences. A survey of surgeons reported by Callam et al. 14 found that necrosis due to compression was ‘common’ in Scotland. Guidelines advocate that only those clinicians who have the necessary skills and have undergone appropriate training should be involved in the assessment and application of compression hosiery.
Footnotes
The authors hereby declare no conflict of interests.