
Abstract
In recent years, minimally invasive endovenous treatments have gained popularity in the treatment of superficial venous reflux. The perceived advantages of endovenous therapy include reduced pain, high vein occlusion rates, and early return to work and normal activities. Endovenous radiofrequency ablation (RFA) involves the delivery of thermal energy from a bipolar catheter to the venous segment to be treated. This technique has been available since 1998 and numerous devices and catheters are now produced. Numerous prospective and randomized studies have compared the effectiveness of RFA with traditional and endovenous procedures. In this article, the available evidence for clinical effectiveness, quality of life and cost gains following endovenous RFA is summarized. The scientific principles behind RFA and technical procedural considerations are discussed and standards of care for the delivery of endovenous RFA are proposed.
Keywords
Introduction
The desire to reduce the operative risks and morbidity following varicose vein treatment has been a powerful driver in the development of minimally invasive endovenous techniques for the correction of superficial venous reflux. Radio-frequency energy is commonly used for the ablation of aberrant electrical pathways in the heart and neoplastic lesions, particularly in the liver and kidney. Radiofrequency ablation (RFA) for the treatment of superficial venous reflux has been available since 1998 and is now established as a safe and efficacious treatment modality for the ablation of refluxing superficial and perforating veins. According to device manufacturers, over 300,000 patients have been treated with endovenous RFA worldwide.
In recent years, the available technology has evolved markedly and there are now numerous RFA manufacturers and devices available. Significant advances in the other available venous treatment modalities, and the increasing emphasis on quality of life and cost-effectiveness, have added further confusion for patients and clinicians regarding the optimal strategy for the treatment of varicose veins. The aim of this article is to summarize the available evidence for the clinical and quality-of-life outcomes and cost-effectiveness following RFA for superficial venous reflux. Standards of care for the delivery of endovenous RFA within a varicose vein service are proposed.
Methods
A systematic review using Pubmed, Embase and Cinahl databases was performed to identify relevant clinical studies up to July 2008. The initial search terms ‘RFA’, ‘radiofrequency obliteration’ and ‘VNUS’ were used in combination with ‘varicose veins’, ‘endovenous’ or ‘venous’ with appropriate search limits. Prospective studies, randomized clinical trials and meta-analyses reporting clinical, quality-of-life outcomes or cost-effectiveness were scrutinized.
Principles of radiofrequency ablation
Scientific principles
The underlying principle of RFA involves the delivery of thermal energy derived from an electric current to the venous segment to be treated. This is achieved using a bipolar endovenous catheter with a typical power of 2–4 W, which is used to generate temperatures of 85–120°C. As the procedure relies on direct contact between the RFA catheter and the vein wall, it is essential that the vein is emptied of blood during ablation (achieved using Trendelenberg position, use of tumescent anaesthesia and extrinsic compression). There is an in-built feedback mechanism, which evaluates the vein wall impedance and can adjust the energy delivery accordingly to ensure that the fibre temperature remains consistent.
Ex vivo histological studies of venous segments treated with RFA demonstrated homogeneous intimal and medial thermal ablation and disintegration. This differed from veins treated with endovenous laser ablation, where major perivenous tissue ablation and vein wall perforations were present. 1
Available devices
The current market leader for endovenous RFA devices is VNUS® Medical Technologies Inc. (San José, CA, USA). The VNUS ClosureTM catheter has been available for nearly a decade and requires a continuous pullback technique. This was commonly used with a tight compressive rubber bandage (Esmark®, Hygenic Corp., Akron, OH, USA) to facilitate venous emptying during treatment. In 2006, VNUS launched the ClosureFastTM segmental ablation catheter, which allows RFA of superficial veins in 7 cm segments, thus eliminating the continuous pull-back technique (Figure 1). The segmental ablation has the theoretical advantages of greater consistency in the vein treatment and increased speed of ablation as each 7 cm segment can be treated in 20 seconds. It should be noted that VNUS also market a specific stylet device (VNUS RFSTM stylet) for the ablation of incompetent perforating veins. All VNUS catheters may be used with the VNUS RFG PlusTM generator (Figure 2).
Illustration of the segmental ablation technique using the VNUS ClosureFastTM catheter. VNUS RFG PlusTM radiofrequency generator with ClosureFastTM segmental ablation catheter.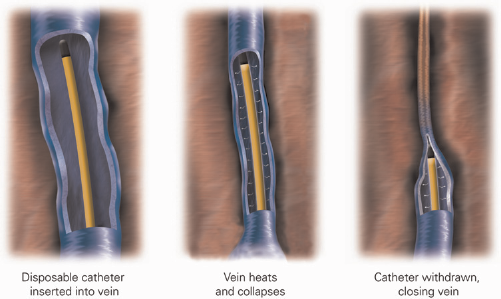

The Olympus Celon RFITTTM (Olympus Medical Systems, Hamburg, Germany) is an alternative RFA system which has been upgraded recently (Figure 3). The system uses the continuous pull-back technique and claims to treat venous segments at a pull-back speed of 1 cm/s, although clinical studies using this new device are scarce.
Olympus RFITTTM RFA generator
Description of technique
Although there are broad similarities between the various endovenous therapies, the location of treatment, type of anaesthetic and numerous other factors will be dictated by the personal preference of clinicians (see Delivering a radiofrequency ablation varicose vein service below). The generic technique for RFA can be summarized in the following steps:
Preoperative planning and consent
As occlusion of the treated venous segment is widely accepted as a measure of treatment success, preoperative duplex imaging should be performed prior to any endovenous intervention. Preoperative marking of the incompetent venous segment and junction with the deep vein should also be considered, as this may aid intra-operative catheter placement. Patients should be warned about the potential risks of recurrence, nerve damage, skin burns, deep venous thermal injury and deep vein thrombosis (DVT) (see Adverse events and potential hazards below).
Patient positioning
The patient should be positioned supine for great saphenous or anterior thigh vein ablation and in the prone position for ablation of small saphenous or Giacomini veins. The operating table or trolley should allow Trendelenberg and reverse Trendelenberg positioning.
Cannulation of vein to be treated
In the reverse Trendelenberg position, the refluxing superficial vein should be cannulated with a 7F sheath using the Seldinger technique under ultrasound guidance. Ideally, the cannulation site should be at the most distal point of venous reflux and cannulation may be facilitated using proximal venous compression (to promote venous distension) or surgical cut down.
Positioning of radiofrequency catheter using ultrasound
For the treatment of GSV or SSV reflux, device manufacturers recommend that the catheter tip should be placed no closer than 2 cm from the saphenofemoral or saphenopopliteal junctions, respectively.
Tumescent anaesthesia
The aim of tumescent anaesthesia is to provide a thermal buffer around the vein to be treated and also offer perioperative analgesia. A dilute mixture of lidocaine in normal saline may be used. Fifty millilitres of 1% lidocaine with 1:200,000 adrenaline is used in 500 mL 0.9% saline for unilateral procedures, or in 1000 mL 0.9% saline for bilateral procedures. The same preparations are used for procedures performed using local or general anaesthesia. The anaesthetic should be delivered under ultrasound guidance either by hand using a needle and syringe, or using a pump device. Volumes of tumescence administered may vary, but are commonly in the region of 75–100 mL per 10 cm of vein. Care should be taken to ensure adequate tumescent infiltration between the proximal GSV and deep vein near the saphenofemoral junction. With procedures performed using tumescent/local anaesthesia alone, the use of local anaesthetic cream along the length of the vein to be treated may aid the administration of tumescence.
Radiofrequency ablation
For continuous pull-back systems, the catheter should be gradually withdrawn according to the recommendations of the specific catheter manufacturer. Using the VNUS ClosureTM catheter, a slow infusion of heparinized saline via the catheter is recommended during pull-back. With the VNUS ClosureFastTM segmental ablation catheter, the vein is ablated in 7 cm segments with extrinsic compression applied using a roll of crêpe bandage. The manufacturers recommend double treatment of the most proximal venous segment (near the SFJ) and single treatment of subsequent venous segments. Immediately following the ablation, the patency and compressibility of the femoral vein (for GSV ablation) should be verified with ultrasound.
Postoperative management, follow-up and outcome surveillance
There is no consensus on optimal type or duration of compression following RFA, but TEDS, or class I or II above knee compression stockings worn for one to two weeks are common regimens. Recent guidelines from the American Venous Forum for the reporting of studies of endovenous treatment recommended early (<1 month) and late postoperative duplex scans. Clearly, local resource availability and clinician preference will dictate local follow-up and imaging protocols. It should be noted that the most recent NICE guidance for RFA was published in 2003 and this concluded that the procedure was safe and efficacious, but commented on the lack of long-term studies and recommended audit of outcomes.
Results following radiofrequency ablation
When interpreting these results, it should be noted that the vast majority of published studies report outcomes using the VNUS ClosureTM continuous pull-back catheter, whereas the VNUS ClosureFastTM segmental ablation catheter is the device primarily marketed by VNUS and growing in popularity. A total of 23 published reports, consisting of three randomized trials, two meta-analyses and 15 prospective observational studies were included in this review. Only one prospective case series using the VNUS ClosureFastTM catheter was identified. Details of the studies included are presented in Table 1.
Published prospective clinical studies of endovenous radiofrequency ablation (RFA)
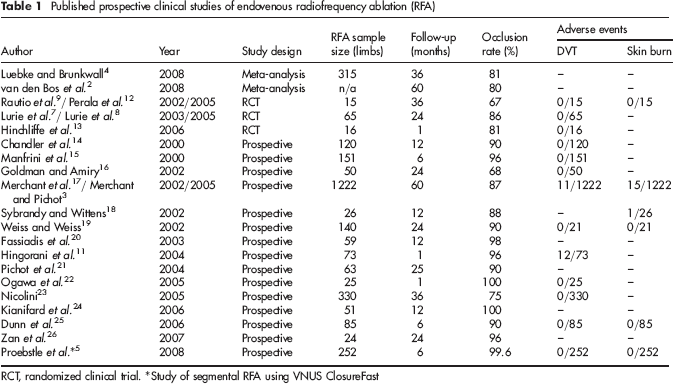
RCT, randomized clinical trial. *Study of segmental RFA using VNUS ClosureFast
Technical success and clinical outcomes
Although there is significant heterogeneity between clinical studies and variations in reported outcomes, recanalization of the treated venous segment is commonly reported as a marker of technical success.
VNUS closure
Reported vein closure rates vary between 67% and 100% (Table 1). In a recent meta-analysis, the early technical success following RFA was found to be 89% (3 months), reducing to 80% after five years. 2 These figures compared favourably to traditional surgery and foam sclerotherapy, but were lower than endovenous laser ablation. By far, the largest patient series treated by VNUS ClosureTM was published in 2005 and reported five-year clinical and anatomical outcomes following RFA in 1006 patients (1222 legs). 3 Data were collected from a prospective international registry and occlusion rates of 87.2% were seen at five years. Significant improvements in pain, fatigue and oedema were seen up to five years and interestingly, these improvements were present despite recurrent truncal reflux. Recurrent varicosities were seen in 27% of patients at five years and anatomical failure of RFA was an independent risk factor for varicosity recurrence. 3 Within randomized studies, recurrent varicosities were seen in 48/217 (22%) of patients at four years. 4
VNUS ClosureFastTM
The only published study reporting outcomes following VNUS ClosureFastTM was published in early 2008. The occlusion rate following segmental RFA was 99.6% at two years and 70% of treated patients did not require any analgesia postprocedure. 5 A direct comparison of postoperative pain scores between RFA and laser ablation has been conducted in the Recovery trial sponsored by VNUS (unpublished data), but preliminary results showed significant lower pain scores following VNUS ClosureFastTM. 6
Quality-of-life changes
Studies of quality of life are scarce, but significant improvements in disease-specific quality-of-life following RFA were reported in the EVOLVeS study, using the CIVIQ2 questionnaire.7,8 Moreover, these quality-of-life gains were greater than patients treated with traditional venous surgery.
Cost-effectiveness of treatment
To date, there have been few studies assessing the cost-effectiveness of RFA for the treatment of varicose veins. In a small randomized study of 28 patients, a basic cost-analysis demonstrated that VNUS Closure was more expensive than conventional surgery in terms of direct costs, but the costs to society were significantly lower in view of the rapid return to work in the RFA group. 9 A subsequent decision-tree analysis also suggested that RFA performed in an office setting may be cheaper than traditional surgery 10 Clearly the cost of procedures will be heavily influenced by clinician preferences on type of anaesthetic, the use of concomitant ambulatory phlebectomy and whether to perform bilateral procedures in a single sitting, thus saving the cost of an additional RFA catheter. For the treatment of unilateral great saphenous vein reflux, office-based RFA using only tumescent anaesthesia is likely to be cheaper than traditional GSV-stripping under general anaesthesia, and this has been the main component of the NHS business case produced by VNUS to support the use of their catheters. However, further well-designed studies of cost-effectiveness are urgently needed to guide those having to make decisions about treatment commissioning and rationing.
Potential hazards and adverse events
As with all endovenous interventions, RFA may be associated with technical difficulties in cannulation, guide wire and catheter advancement. These issues are likely to resolve with increasing experience and familiarity with the equipment and technique. Specific complications including DVT, skin burns, superficial thrombophlebitis, neuralgia and bruising have been reported following RFA, but the incidence of these problems appears low. In one study, 12/73 limbs (16%) developed DVT within 30 days of RFA, 11 but the incidence of DVT in the majority of studies is <1%. Of the 1006 patients recorded in the Closure international registry, the reported complications were DVT (0.9%), phlebitis (2.9%) and skin burn (1.2%), although the majority of burns occurred in patients not given tumescence. 3 The influence of the volume of tumescence and post-procedure compression on the incidence of these complications is poorly understood and warrants further investigation.
Training implications
There is currently no structured pathway for the training of clinicians to perform endovenous ablation procedures. Those planning to perform RFA should ensure familiarity with the energy generator and treatment catheters and be able to demonstrate competence in the use of intra-operative colour duplex ultrasound. Depending on local resources and knowledge, attendance at clinical workshops and courses or clinical mentorship programmes may help to achieve competence.
Delivering a radiofrequency ablation varicose vein service
The precise format of a RFA varicose vein service will depend heavily on the personal preference of clinicians. Specific factors dependent on clinician preference include:
Type of anaesthetic;
Treatment strategy for varicosities;
Approach to patients requiring bilateral interventions;
Postprocedure compression type and duration;
Follow-up and surveillance protocol.
Nevertheless, a number of general key issues should be considered and addressed when planning, starting and delivering a RFA varicose vein service. These include:
Training and assessment of competence
The responsible clinician should ensure appropriate theoretical and practical training for core team members prior to starting a service. Local vascular scientists maybe an excellent resource for the acquisition of duplex ultrasound skills and it may be appropriate to perform initial cases with a vascular scientist performing the imaging. Mentorship arrangements involving experienced practitioners and departments with a large throughput of RFA procedures may be useful strategies to acquire and reinforce new endovenous skills.
Trust approval and funding
The clinical team may be required to undertake a risk assessment and produce a business case to justify the introduction of a new technique. Proposals should be discussed with Clinical Governance and Clinical Safety departments. Device manufacturers usually have considerable experience of this process and may be of assistance.
Multidisciplinary team approach
Vascular surgeons, vascular scientists, theatre and outpatient nursing staff are likely to be key members of the multidisciplinary team. They should be consulted and involved at each stage of the planning, training and service implementation processes.
Patient selection and consent
The process and risks of RFA should be openly discussed with all patients as well as the level of experience of the clinical team. Clinical information leaflets should be produced (using local information guidelines) and given to prospective patients. Patients could be directed to the wealth of online information available on endovenous procedures.
Location of treatment
Treatment may be offered in an operating theatre or in an office-based or adapted clinic room setting. The treatment of patients outside the expensive operating theatre setting may seem appealing, but it is essential to ensure that any area considered for RFA treatment has adequate space, lighting, access to equipment and other essential facilities. In particular, the availability of an appropriate operating table or bed is essential.
Treatment algorithm
To ensure that the provision of RFA is consistent, treatment algorithms for the management of patients with varicose veins should be locally agreed and disseminated.
Clinical follow-up, outcome evaluation and audit
Specific follow-up protocols will be dictated by individual clinician preference, but efforts should be made to audit technical and clinical outcomes as with all new interventions.
Proposed standards for endovenous radiofrequency ablation
There are currently no clinical guidelines specifying basic standards in the provision of RFA for superficial venous reflux. In addition to the principles of Clinical Governance, the following benchmarks are proposed as minimum standards of clinical practice:
Intra-operative colour duplex imaging should be performed by an individual able to demonstrate technical competence in vascular duplex imaging;
Pre-operative duplex imaging should be performed by an accredited vascular scientist (or appropriately trained clinician) in all cases;
Procedural documentation should include:
Length of vein ablated;
The vein treated and precise site of cannulation;
Duration of treatment;
Details of energy delivered, power settings and other variables.
Post-procedural follow-up is controversial, but should ideally include clinical assessment and colour duplex imaging to evaluate technical success. This is particularly important during the learning phase as an objective assessment of quality control. Clearly, this policy will be strongly influenced by local resource availability and a more pragmatic approach of scanning only symptomatic patients may be preferred. However, as RFA for the treatment of varicose veins is a novel technique, objective evaluation of technical success may be desirable. Reasons for not implementing a policy of routine postoperative duplex imaging include cost and also the fact that that main determinant of subsequent therapy is likely to be the presence of symptoms, rather than the presence of venous reflux.
Clinicians should prospectively collect audit data including procedural details, adverse events, clinical and technical outcomes. This may be best achieved by using an international registry.
Conclusion
RFA is established as an acceptable and efficacious endovenous treatment modality for the treatment of varicose veins. However, further studies are needed to clarify the advantages of the recently introduced segmental ablation VNUS ClosureFastTM catheter, particularly in terms of postoperative pain and bruising. Although many treatment variables are highly dependent on clinician preference, principles for the safe introduction of a RFA service and standards of care are proposed in this document. Clinicians performing RFA for the treatment of varicose veins should ensure accurate audit of interventions and outcomes. Further consensus is needed on the optimal post-procedural treatment regimen and follow-up surveillance in this patient group.
Footnotes
The authors hereby declare no conflict of interests.