
Abstract
Objective:
To study the effect of coil embolization of the insufficient ovarian vein (IOV) on varices of the lower limb (VLL).
Method:
From December 2005 until May 2008, we selected all patients with phlebograms that were performed in our hospital to confirm the diagnosis of insufficiency of the ovarian vein. The CEAP (clinical, aetiological, anatomical and pathological elements) classification was used to classify the lower-limb venous disease in each patient. All patients with suspected IOV in combination with VLL underwent a phlebography. If IOV was found, coil embolization of the ovarian vein(s) was performed.
Results:
IOV was found in 43 of 44 patients (98%). After coil embolization of the ovarian vein(s), VLL disappeared in five patients (12%) without any further treatment. Improvement in CEAP classification was measured in 13 patients (31%). In 21 (88%) of 24 patients with vulval varices, coil embolization of the ovarian vein(s) resulted in disappearance of vulval varices.
Conclusions:
In only 31% of the patients with IOV in combination with VLL, phlebography and coil embolization of the ovarian vein(s) did improve CEAP classification. However, coil embolization of the ovarian vein resulted in disappearance of the vulval varices in 88% of the patients.
Introduction
Varices of the lower limb (VLL) are a common problem. About 25–73% of the female population will experience varices at some point in their life. 1 Recurrence of VLL after surgery occurs in 5–49% of the cases. 2 This can be not only due to re-vascularization or technical errors, but also due to undetected and untreated insufficiency of the ovarian vein (IOV).1,2 Therefore, it is important to correctly define the source of reflux in VLL preoperatively in order to reduce the recurrence rate. IOV is associated with only 8% of all VLL. 3 IOV is often studied in combination with the pelvic congestion syndrome. 4 The signs and symptoms of this syndrome consist of varices of the thigh or vulva, non-cyclic lower abdominal pain for more than six months that can be worsened by walking or postural changes, urinary urgency and dyspareunia.5,6 The accepted surgical treatment of the pelvic congestion syndrome is coiling of the ovarian vein.4,7–9 In most cases, varices which result from IOV are primarily located on the medial side of the thigh and often also give varices of the vulva and labia majora. Because of connections between the pelvic veins and veins of the lower limb, IOV can result in varicose veins of the vulva and leg. 10 In pregnancy, when the vascular capacity of the ovarian vein can rise up to 60 times the normal value, 6 varices of the vulva can arise or worsen. 10 In our clinic we have special interest in the treatment of the combination of IOV and VLL. The aim of this study is to evaluate the effect of coil embolization of the ovarian vein in patients with a combination of IOV and VLL.
Patients and methods
We performed a retrospective search of all phlebograms performed in our hospital from December 2005 until May 2008 to confirm the diagnosis of ovarian vein insufficiency. No additional examinations were performed to confirm this diagnosis. In total, 44 phlebograms were conducted to confirm the diagnosis of ovarian vein insufficiency.
All 44 female patients were previously seen in our outpatient phlebology clinic presenting with VLL and with the suspicion of IOV. The CEAP (clinical, aetiological, anatomical and pathological elements) classification was used to classify the lower-limb venous disease in the patients. All patients received a questionnaire by mail. This questionnaire contained the following topics: itching or oedema of the legs before and after the procedure, presence of varices and/or pain after the procedure, use of compression stocking after the procedure and whether they underwent further treatment after the procedure. We also asked whether they would undergo the procedure again if necessary.
The preoperative diagnosis of IOV was based on clinical examination (varices on the medial side of the thigh or varices of the vulva) and/or on duplex scanning, which was used to show the origin of the varices rising from the pelvis. During duplex scanning, we did not score incompetence of the deep or superficial epigastric veins. In 29 of the 44 patients an insufficient vein on duplex scanning was shown to arise from the pelvis. All patients with an IOV with complaints of varices of the limb or vulva underwent a phlebography.
Phlebography was performed by puncture of the right common femoral vein and placement of a 5-Fr vascular sheath. Through this sheath a 0.035-inch guidewire was placed. Then a 5-Fr ‘VSC’-catheter (Cook®) was placed over the guidewire in the left renal vein. Contrast fluid was given while the patient performed a Valsalva manoeuvre. If the left ovarian vein was not visualized, it was assumed that no insufficiency existed and the procedure was repeated at the right side. If the left ovarian vein was shown, the catheter was placed in the left ovarian vein. The patient was asked to do another Valsalva manoeuvre while contrast fluid was manually given with the catheter in place.
If IOV was found, coil embolization (Figure 1) was performed during the same session using Tornado embolization coils (MWCE 35–10/4 Tornado, 12.5 cm [Cook®, Cook Medical Inc, Bloomington, USA]). When technically possible, coiling was started on the distal side of the sacroiliac joint. In the case of collaterals, coil embolization was additionally performed more proximal in the ovarian vein. We used 3–5 coils for each vein, with an average of 3.4 coils. After this procedure, phlebography should show complete occlusion. In one of our patients coil embolization could not be performed because the ovarian vein was too distended. In this case, a plug was placed (Amplatzer Vascular Plug®, 12 mm, AGA Medical®, Golden Valley, USA) in the ovarian vein.
The process of coil embolization of the insufficient ovarian vein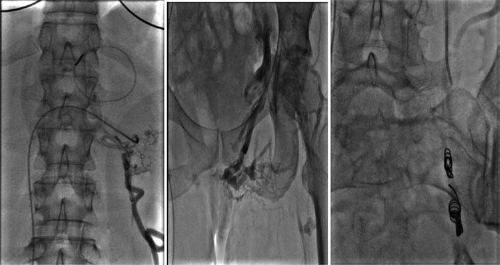
Then also the right ovarian vein was visualized using a 5-Fr Simmons 1 catheter (Cook®). The catheter was placed in the inferior vena cava and minimal contrast fluid was given to show the ostium of the right ovarian vein. The further procedure was similar to that of the left side. Again, the procedure was ended when obliteration of the vessel was shown.
After the procedure the sheath was removed and manual compression was performed for 3–5 minutes. The diagnostic procedure was not performed with any table tilt. Afterwards we instructed patients to remain in bed for at least an hour. Patients were discharged from hospital the same day and the next day all physical activities can be restored. To evaluate the effect of the procedure all patients were seen in our clinic three months after the procedure. During this visit, patients were again classified according to the CEAP classification.
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences. Within-subject changes in CEAP classification were tested using McNemar's test. A χ 2 test was used to compare differences in the presence of IOV between the left and right ovarian veins.
Results
The mean age of the patients at the time of the phlebogram was 45 years. Insufficiency of one or both of the ovarian veins was found in 43 of 44 patients (98%). In one patient no IOV could be detected. In the first 12 patients incompetence of the internal iliac vein was investigated, but because this did not lead to a new intervention, it was not performed as a standard procedure in the other participants. In 19 patients (44%) there was insufficiency of the left ovarian vein, in three patients (7.0%) of the right ovarian vein and in 21 patients (49%) both ovarian veins were insufficient. The observed left/right ratio 19/3 of IOV differs significantly from an expected ratio of 11/11; P = 0.001 (Table 1).
Patients’ characteristics at entry into the follow-up study
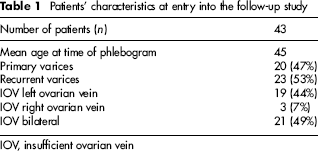
IOV, insufficient ovarian vein
Technical success as in occlusion of the ovarian vein after coil embolization was 100%. No major complications (death, major bleeding or infection) were encountered.
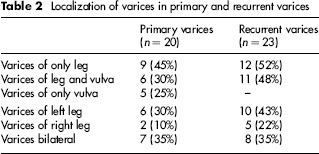
Twenty (47%) patients had primary varices. In this group, nine patients (45%) had varices of the leg only, six patients (30%) of the leg and vulva and five patients (25%) only of the vulva. Primary varices were located in both legs in seven patients (35%), in the left leg in six patients (30%) and in the right leg in two patients (10%) (Table 2).
Localization of varices in primary and recurrent varices
Insufficiency of the greater saphenous vein was found in 38 patients with varices of one or both legs. None of the patients who only had varices of the vulva had insufficiency of the great saphenous vein.
Twenty-three (53%) patients had recurrent varices after previous surgical treatment for varices. In this group 12 patients (52%) had varices of the leg(s) alone and 11 patients (48%) the leg and vulva. Recurrence of varices was bilateral in eight patients (35%), situated in the left leg in 10 (43%) and the right leg in five patients (22%).
Patients were first seen in our clinic three months after the procedure. For further follow-up patients were contacted by letter. The follow-up rate was 98%; one patient was lost during follow up. This patient was diagnosed as C3 before coil embolization and had vulval varices. The patient with no signs of IOV on phlebogram was only asked if she experienced the phlebography as stressful. The follow-up period was 1–3 1/2 years, with a mean of 1.8 years.
Patients were classified as C2 (32 patients, 74%) and C3 (11 patients, 26%) according to the CEAP classification.
In six patients (14%, 4 patients classified as C2 and 2 as C3), VLL disappeared after coil embolization of the IOV without any further treatment. Twenty-seven patients (63%) underwent further treatment in the form of sclerocompression therapy, phlebectomy or compression stockings for more than three months. In 10 patients (23%), VLL did not disappear, but these patients underwent no further treatment. Varices were still visible even after further treatment in 33 patients (77%) (Table 3).
CEAP classification before and after coiling of the IOV and with or without further therapy
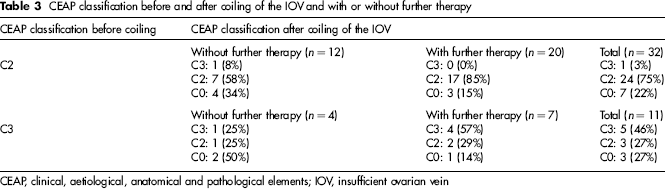
CEAP, clinical, aetiological, anatomical and pathological elements; IOV, insufficient ovarian vein
At the end of follow-up, 10 patients (23%) were classified C0 after coil embolization of the IOV with or without further treatment. Coil-embolization with or without further treatment had resulted in improvement of VLL in 14 patients (33%) with the best result in the C3-subgroup (55% of patients with improvement versus 22% in the C2-subgroup). This improvement in CEAP classification after coil embolization of the IOV with or without further treatment is significant in correlation to the CEAP classification before treatment (P < 0.01) (Table 3).
The best clinical result was observed with respect to the vulval varices. Twenty-five patients (57%) suffered from vulval varices. One patient with vulval varices was lost during follow-up. In the remaining 24 patients, vulval varices disappeared after coil embolization of the IOV in 21 patients (88%) and persisted in only three patients (12%). Coil embolization of the IOV resulted in a significant (P < 0.05) reduction of vulval varices.
None of the patients experienced the procedure as stressful. Forty-one patients (95%) would undergo the procedure again if necessary. The patients who did not want to undergo the procedure again were disappointed with the result (1 patient) or became very nauseous two hours after the procedure (1 patient), possibly due to an allergic reaction to the contrast fluid.
Discussion
We analysed the effect of coil embolization of the ovarian vein on VLL inpatients with IOV, and concluded that treatment of VLL in the presence of IOV remains difficult.
Congestion of varices of the leg may occur by congestion of the pelvic veins through the connection between these veins and those of the leg. These varices are more often located on the inside of the thigh and on the vulva.1,9 Most studies report about IOV in relation to pelvic congestion syndrome.5,7,8 In our study, we analysed patients with IOV without symptoms of pelvic congestion syndrome, but with varices of the lower limb and/or vulva.
In our study, the ovarian vein was insufficient on the right side in three patients (7%), on the left side in 19 patients (44%) and bilaterally in 21 patients (49%). Several factors might account for the higher prevalence of IOV on the left side compared with the right side. Anatomic studies reveal that valves are absent on the left side in 13–15% of the women and only in 6% on the right side.5,7,8 Also, like in insufficiency of the testicular vein in men, the angle in which the left ovarian vein enters the renal vein is much greater than on the right side where the ovarian vein enters the inferior vena cava. 1
The technical success after coil embolization was 100%. Clinical results were, however, disappointing as 33 patients (77%) still had visible varices even after further treatment of VLL. In this group, improvement in CEAP classification (C2 to C0 or C3 to C0 or C2) was found in 33% of patients, with the best result in the C3-subgroup (55%). In 65% of the patients’ CEAP classification did not improve and in only 2% was deterioration observed. So our hypothesis that after coil embolization the congestion would be diminished and VLL would disappear was only partly true. The VLL did not disappear after coil embolization; this is probably because VLL is not due to just one cause, but is the result of insufficiency of multiple venous structures like the great saphenous vein, short saphenous vein and perforating veins.
The effect of embolization of the IOV on vulval varices was very good. In 88% the vulval varices disappeared completely. In three patients (12%) vulval varices remained or re-appeared after some time. Our study also showed that the procedure of coil embolization of the IOV is very well tolerated by the patient. None of the patients found the procedure stressful.
Limitations of the study
In only 12 patients were the internal iliac veins imaged during phlebography. This may have resulted in inadequate treatment of insufficient pelvic veins in the other patients. Therefore, treatment of varices of the lower limb can be improved by the visualizing and treatment of (insufficient) pelvic veins in all patients suffering from VLL. Failure to treat the ovarian vein reflux at the original procedure may have contributed to the high recurrence rate of varicose veins after initial treatment. It is likely that this recurrence rate would be lower if coil embolization of the ovarian vein was performed during the original procedure. However, the effect of treatment of ovarian vein or pelvic vein reflux at the initial treatment on the recurrence of varicose veins should be further studied.
Conclusion
Although coil embolization of the IOV theoretically should improve outcome in lower-limb varices, we observed that most patients still experience varices, even after further treatment. This might be because insufficiency of veins is not strictly limited to one vein, but is a ‘systemic’ problem. It probably affects not only the ovarian vein, but also the great saphenous, small saphenous or perforating veins. Coil embolization has proven its use in the pelvic congestion syndrome, but it remains unclear as to whether it should be used in VLL caused by IOV. The effect of coiling on varices of the vulva, however, is very good, with a clinical success rate of 88%. Because of the low complication rate and the fact that it is very well tolerated by the patient, we recommend continuing this treatment when IOV is suspected even in patients without vulval varices.