
Abstract
Objective
To investigate the abnormal expressions of Tie1 on the valves of great saphenous varicose vein, and to discuss the relationship between the phenomenon and pathogenesis of varicose vein of lower extremity.
Methods
Varicose veins group 18 samples, normal control group 14 samples. Immunohistochemistry staining has investigated the expression of CD31 and Tie1 in the first valves of great saphenous veins. Semi-quantitative reverse transcription-polymerase chain reaction (RT-PCR) has checked mRNA expression of Tie1. Western blot has checked the expression of Tie1 protein in venous valves.
Results
In normal control group valves, there was no difference between proximal and distal sides endothelium, which expressing CD31 in both valvar basement and valve cusp (positive endothelial cells [ECs] percentage: P > 0.05, P > 0.05). However, the endothelium of the proximal side demonstrates Tie1 stronger than distal side in valvar basement (positive ECs percentage: P < 0.05), which was not found at valve cusp (positive ECs percentage: P > 0.05). In varicose veins group, the endothelium of proximal side cells expresses CD31 weaker than distal side at both valvar basement and valve cusp (positive ECs percentage: P < 0.05, P < 0.05) besides the morphological alteration of valves. Moreover, it expresses Tie1 much weaker than diatal side (positive ECs percentage: P < 0.01). Semi-quantitative RT-PCR showed that valves of varicose veins group expressed Tie1 much weaker than the normal control group (P < 0.01). Western blot could not detect the expression of Tie1 in venous valves.
Conclusion
The decreasing expression of Tie1 may play an important role in the pathogenesis of primary lower extremity varicose veins.
Introduction
Ang (Angiopoietin)/Tie (Tyrosine Kinase with Ig and EGF homology domains) signal pathway plays an important role in the process of angiogenesis and vessel maturation. The Ang family includes Ang1, Ang2 and Ang3/4. Their receptors, Tie family, are made up of Tie1 and Tie2, which are enzyme-1inked receptors. They can phosphorylate tyrosine residue of target protein when binding to the ligand angiopoietin. Tie predominantly was explained by endothelial cells (ECs) and haemopoietic cells and over-expressed in the active tissues such as embryo, healing wound and tumour. The recent researches are mainly focused on Ang/Tie2. There are many evidences demonstrating that Tie2 participates in regulating ECs to recruit pericytes and maintains the integrity of blood vessels. 1 However, there are fewer researches focusing on Tie1, because the ligand of Tiel is still unknown until now. Some animal models targeting Tiel suggest that Tie1 may play an important role in haemodynamics, stabilization of capillary vessel, re-modelling and deterioration of vessel. 2
Varicose vein of lower extremity is a common vascular disease. The incidence rate is up to 16–40% in western human beings. 3 However, the causes of the disease are still not clear. The weakness of vein wall, dysfunction of venous valves, venous hypertension and inflammations in venous intima are important factors in occurrence and development of varicose vein. 4 It is considered that blood reflux occurring chiefly at the first valve in great saphenous varicose vein. 5 With the inspiration based on above researches, our study was to investigate the abnormal expressions of Tie1 on the valves of great saphenous varicose vein, and to discuss the relationship between the phenomenon and pathogenesis of varicose vein of the lower extremity.
Materials and methods
General information
Varicose veins group was made up of 18 patients with primary varicose vein who have accepted the surgical treatments from August 2009 to March 2012. It includes eight men and 10 women, 11 left lower limb, seven right lower limb; aged 37–69 years, median age 52.3 years; course of disease 5–30 years and average course of disease 18 years. Selected standard was referenced the Clinical-aEtiology-Anatomic-Pathophysiological classification system: 6 C, clinical symptoms: C4 level (varicose veins with skin changes, such as pigmentation, eczema and scleroderma lipid disorders) and C5 level (varicose veins with healed ulcer); E, aetiology: all the patients were primary varicose vein, secondary causes may be ruled out; A, anatomical location of lesions: lower-extremity superficial or perforating varicose veins, excluding deep veins lesions; P, pathophysiology: venous blood reflux with valves incompetence, excluding venous thrombosis, history of diabetes and related traumas. Preoperative, all patients were examined by vascular ultrasound with the action of Valsalva 7 to show the reflux of great saphenous vein, the time of blood back flow was over two seconds, and incompetence of the first pair of valves also can be seen; to test the function of deep veins, patients underwent anterograde deep venous angiography. 14 cases only showed the great saphenous vein reflux, the other four cases affiliate with deep venous insufficiency. All patients of varicose vein underwent ‘high ligation of saphenous vein and stripping surgery’.
Demographics and risk factors between varicose vein group and control group
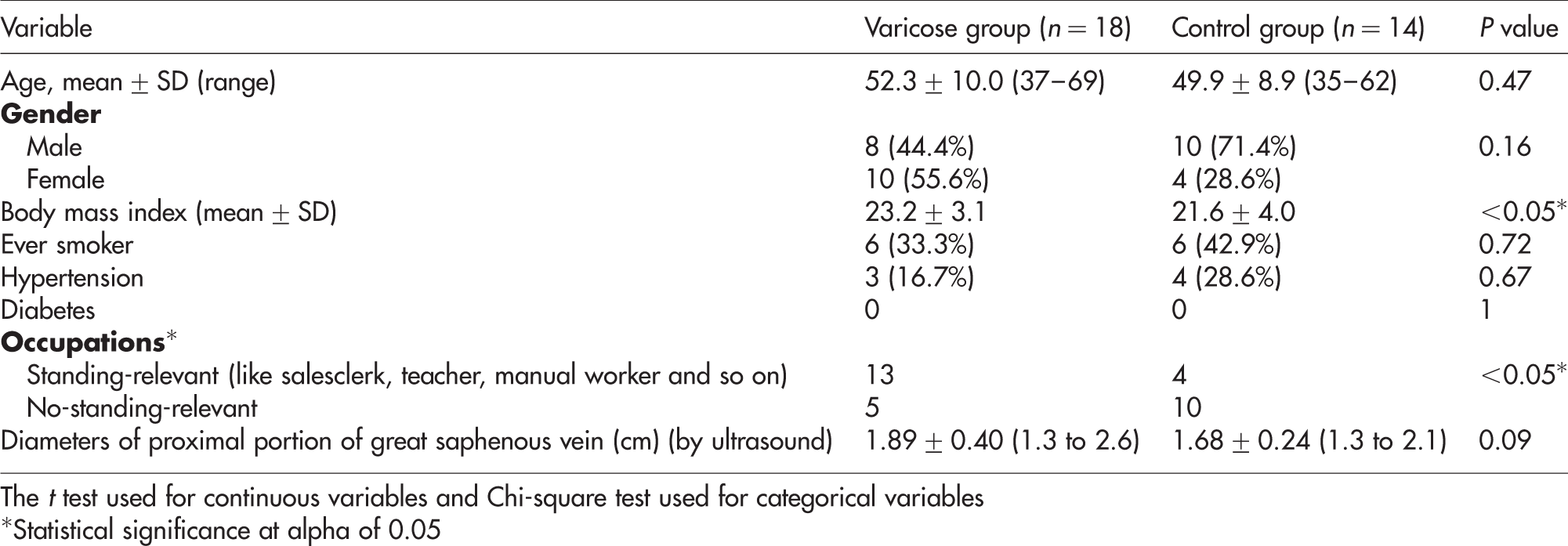
The t test used for continuous variables and Chi-square test used for categorical variables
*Statistical significance at alpha of 0.05
Immunohistochemistry
Immunohistochemical staining of CD31 (platelet/endothelial cell adhesion molecule) and Tie1 was performed by the biotin-linked peroxidase technique. Eight pairs of valves of varicose veins and four pairs of valves of normal veins were collected and marked to identify distal and proximal end, fixed in 4% paraformaldehyde overnight at 4℃, dehydrated and embedded in paraffin. Longitudinal sections (6 μm) of the tissue were prepared. Endogenous peroxidase activities were quenched by incubating sections with 1% H2O2 in methanol for 10 minutes. Then sections were incubated for 120 minutes with primary antibody at room temperature. The signals were amplified using the tyramide signal amplification system PerkinElmer (Waltham, MA), peroxidase activity was developed using 3-amino-9-ethyl carbazole Sigma (St. Louis, MO), and sections were counterstained with haematoxylin before analysis. Phosphate-buffered saline was used in negative control instead of primary antibody. Primary antibodies used in this study include rabbit-anti-human CD31 polyclonal antibody Abcam (Cambridge, MA), working concentration 1:100; goat-anti-human Tie1 polyclonal antibody Santa Cruz (Santa Cruz, CA), working concentration 1:100; immunohistochemistry kit box and auxiliary reagents were purchased from Santa Cruz company.
Semi-quantitative reverse transcription-polymerase chain reaction analysis
Primers used and reaction conditions for reverse transcription-polymerase chain reaction

GAPDH, glyceraldehyde 3-phosphate dehydrogenase
Western blot analysis
Seven pairs of valves from the varicose veins group and the normal control group were harvested and immediately frozen in liquid nitrogen at operations, respectively; 293-T-cells in which Tie1 gene has been transfected were chosen as positive control (a kind gift from Dr He Yulong, Nanjing University), β-actin protein as loading control. Three samples from varicose vein and three from normal control group and 293-T-cells were lysed in the lysis buffer (1% Non-idet P-40, 20 mmol/L Tris-HCl [pH 7.5], 150 mmol/L NaCl, 5 mmol/L EDTA, 2 mmol/L Na3VO4, 100 μmol/L phenylmethylsulphonyl fluoride with proteinase inhibitors cocktail [Roche]), then the lysates were transferred onto nitrocellulose membranes Bio-Rad Laboratories (Hercules, CA). After blocking with 5% fat-free milk solution, the protein of interest were detected by using a primary antibody against Tie1 and a corresponding peroxidase-linked secondary antibody Cell Signaling Technology (Danvers, MA). Blots were developed with electrochemiluminescence (ECL) reagent and exposed on X-ray film. Films were scanned, and Image J software was used to quantitate band density.
Once again, we extracted protein from four valves of varicose group in all, and four valves of normal control group in all, then the same method for Western blotting analysis.
Immunohistochemical semi-quantitative detection
CD31 and Tie1 staining was mainly localized on cell membrane, so the membrane stained brown is considered to be positive staining. Four high-power fields of ECs on both sides of valve at tip and root part were chosen, respectively, to calculate the percentage of positive cells.
Two observers performed the positive cell count in the immunohistochemistry. We also measured the intraobserver variability.
Statistical Analysis
The data were showed as mean ± standard deviation (
Result
Morphological alteration and abnormal expression of CD31 in valves of varicose veins
Valves of normal control group showed upright, normal shaped and both sides of the endothelium were continuous, well-expressed CD31 (Figures 1a and c).The percentage of positive ECs of proximal side (the side against the upstream of the blood) of valve and the distal side (the side following the blood flow) at valvar basement were (93.8 ± 5.6)% and (92.4 ± 3.3)%, respectively; the percentage of positive cells of proximal and distal side at valve cusp were (94.5 ± 3.4)% and (92.9 ± 3.5)%, respectively; and there was no significant difference between the two sides (P > 0.05, P > 0.05). Valves of varicose veins group showed stretching, splitting and adhesion of valve leaflets; staining of distal-side endothelium showed smooth and continuous, however, endotheliums of proximal side were not flat (Figures 1b and d); the percentage of positive ECs of proximal side and the distal side at basement were (72.5 ± 15.4)% and (90.6 ± 3.0)%, respectively, the percentage of positive endothelial cells of proximal and distal side at cusp were (76.2 ± 6.6)% and (88.4 ± 4.1)%, respectively; the endothelial of proximal side expressed CD31 weaker than distal side at both basement and cusp (P < 0.05, P < 0.05).
CD31 expression in venous valves. (a, b) Morphous of valves in normal and varicose veins, arrows indicate the direction of forward flow. (c, d) High magnification of marked area shown in (a, b), respectively, arrowheads point that proximal side endothelial express CD31 weaker than distal side. Scale bars, 200 μm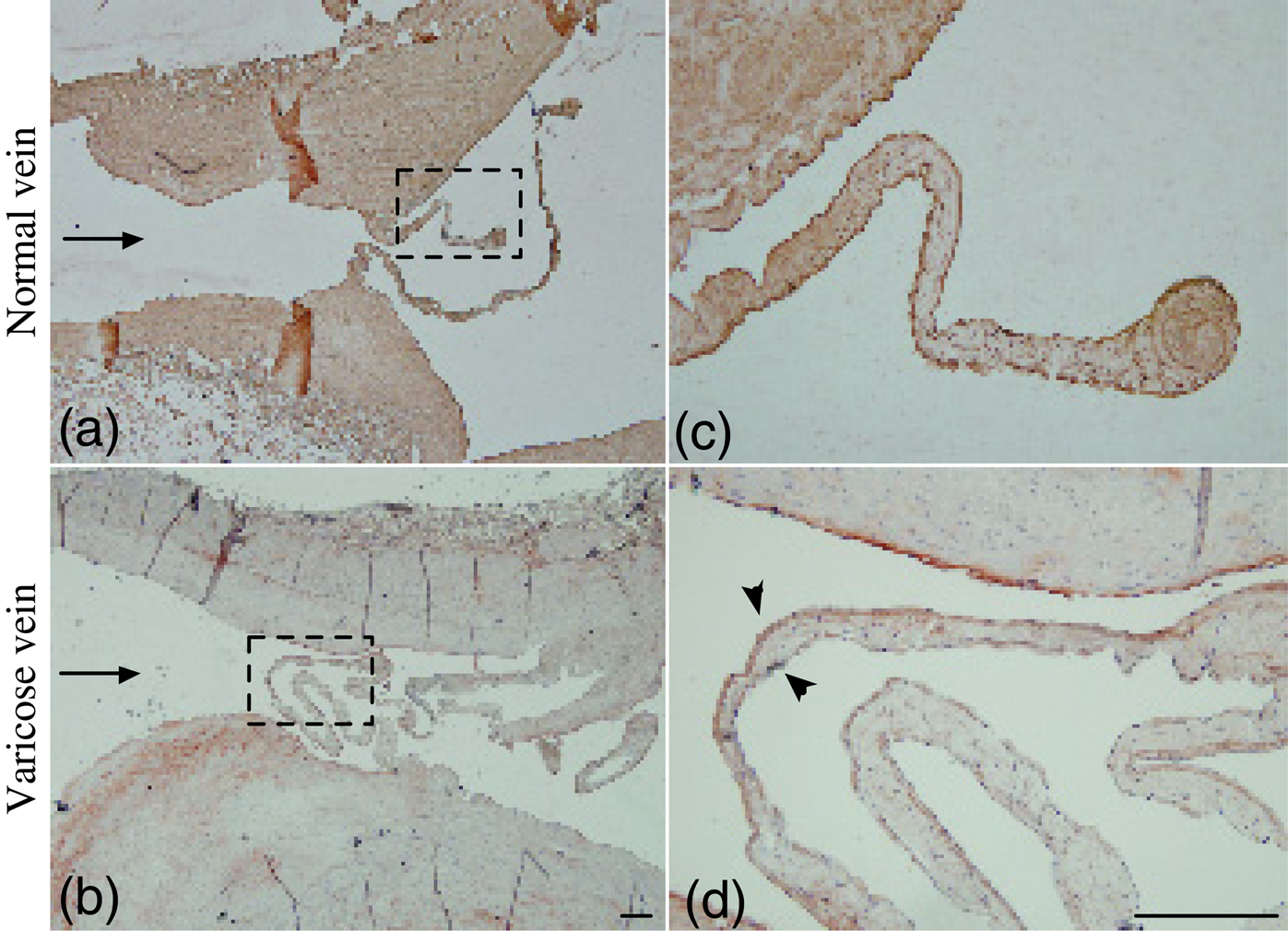
Abnormal expression of Tie1 in valves of varicose veins
Both proximal and distal side endotheliums of valves in normal control group expressed Tie1 completely and continuously (Figures 2a, c and d); at valvular basement, endothelial of the proximal side expressed Tie1 slightly stronger than the distal side (the percentage of positive cells of the two sides were [92.1 ± 8.2]% and [83.3 ± 4.7]%, respectively, P < 0.05); but this difference was not found at valvar cusp (percentage of positive cells of both-side endothelials were [92.2 ± 7.7]% and [90.2 ± 7.5]%, respectively, P > 0.05). In the varicose veins group, the percentage of positive cells of proximal and distal sides were (31.5 ± 9.6)% and (87.3 ± 3.1)%, respectively, at the basement; at the valvar cusp were (33.0 ± 5.7)% and (89.6 ± 4.2)%, respectively; the date showed that the endothelial of proximal side expressed Tie1 weaker than the distal side significantly (P < 0.01, P < 0.01) (Figures 2b, e and f).
Tie1 expression in venous valves. Arrows indicate the direction of forward flow (c–f) are high magnification of marked area shown in (a, b), respectively, arrowheads point that in normal veins, the proximal side expressed Tie1 stronger than the distal side at valvar basement; in varicose veins, the proximal side expressed Tie1 weaker than the distal side at both valvar basement and cusp. Scale bars, 200 μm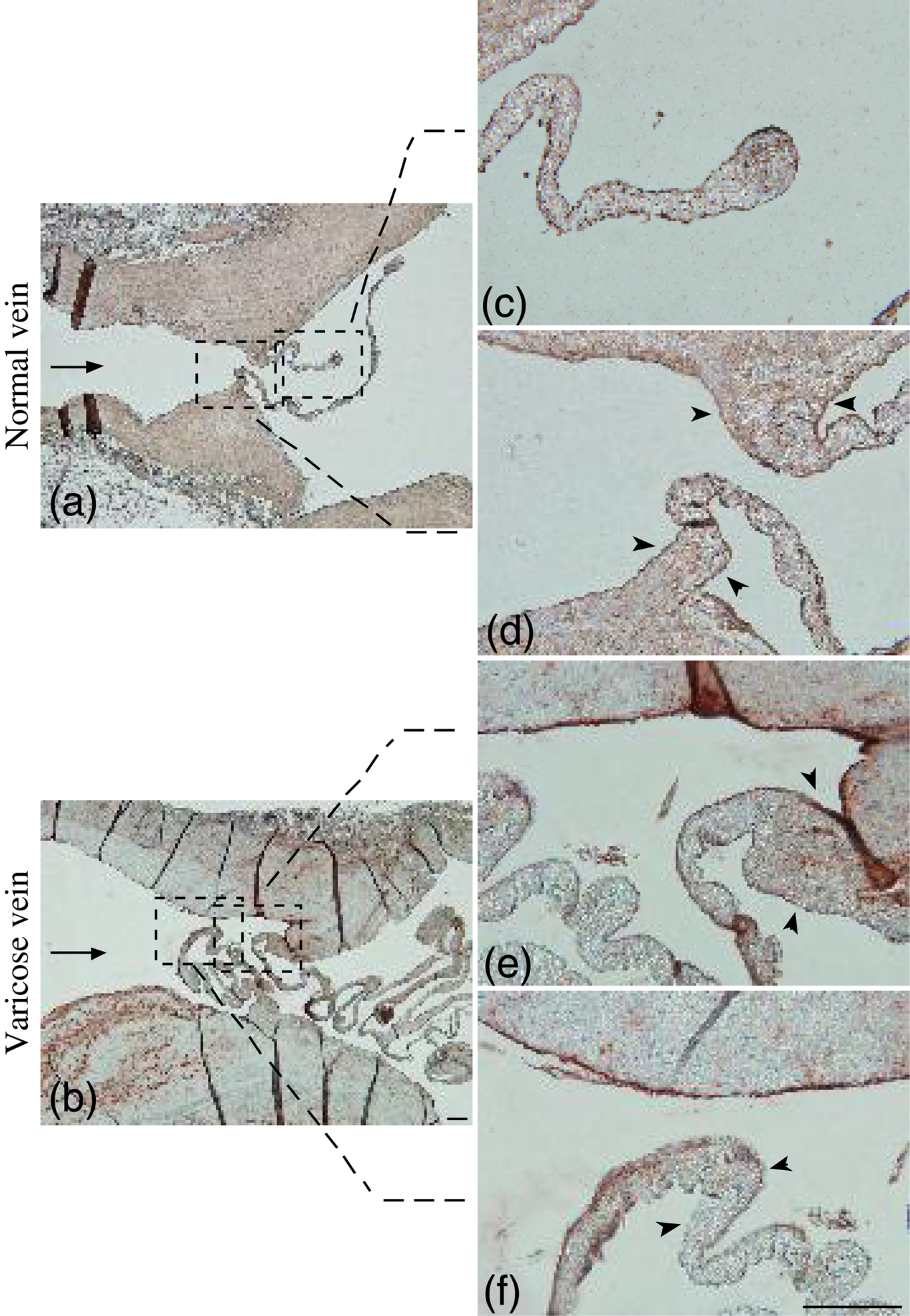
Abnormal expression of Tie1 at mRNA level in valves of varicose veins
We detected the expression of Tie1 in three valves of varicose veins and normal veins, respectively, by semi-quantitative RT-PCR analysis. Figure 3 shows that the expression level of Tie1 mRNA was much lower in varicose veins.
Semi-quantitative reverse transcription-polymerase chain reaction (RT-PCR) analysis of Tie1 expression in venous valves. RNA from these valves was isolated and subjected to RT-PCR analyses. (a) The PCR products were electrophoresed in an ethidium bromide agarose gel and visualized under ultraviolet light. (b) Quantitative data (means ± SD) from the gels were normalized to glyceraldehyde 3-phosphate dehydrogenase (GAPDH). These data are based on three independent experiments. *P < 0.01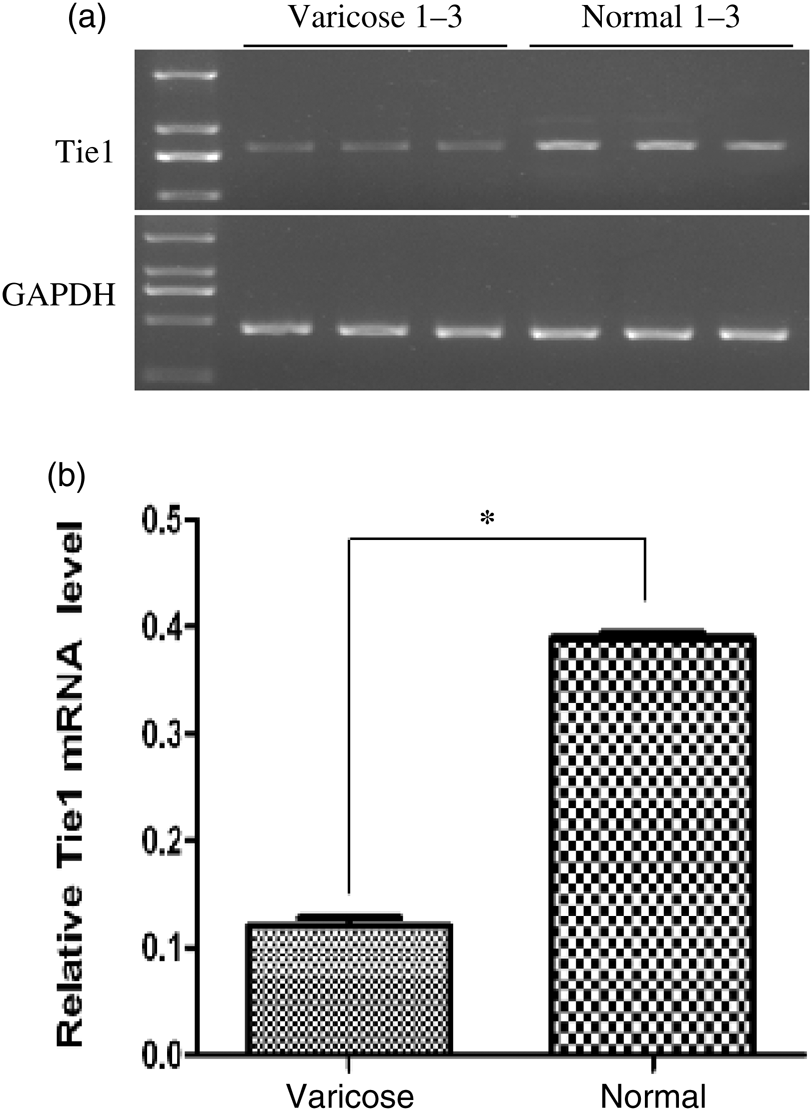
Tie1 protein of venous valves could not be detected through Western blotting
As Tie1 protein in one pair of valves was too low to be detected by Western blot, so we put four pairs of valves together to extract protein, but Western blotting still failed to detect Tie1 protein; Tie1 expression of Tie1-transfected 293-T-cells showed well (Figure 4).
Western blot analysis of Tie1 protein in venous valves. Western blot failed to detect Tie1 expression in venous valves, Tie1-transfected 293-T-cells were chosen as positive control, β-actin as loading control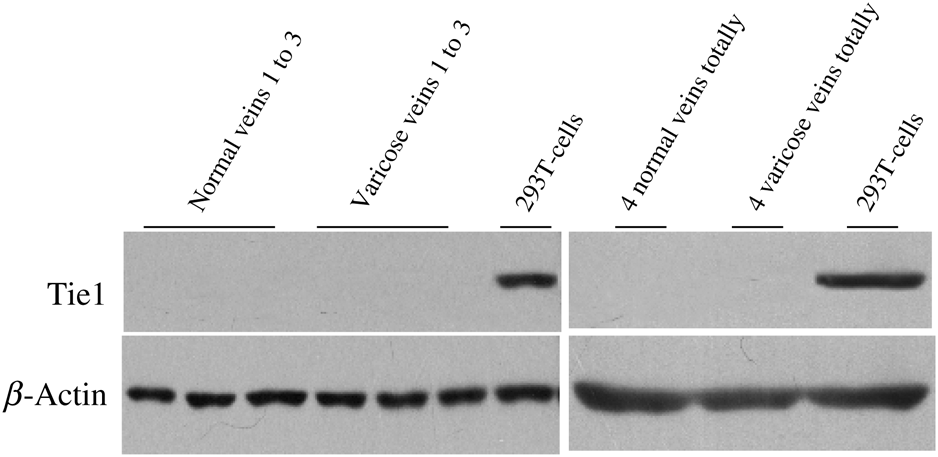
Discussion
Porat et al. 8 have found that the distal-side endothelial of the aortic valve (the side against the upstream) expressed Tie1 stronger than the proximal side in mouse models, indicating that there is a certain relationship between Tie1 expression level of valvar ECs and the blood pressure or shear stress; some researches also showed that the expression level of Tie1 determined its phosphorylation level. 9 And Tie1 can enhance the junction of endothelial cells, maintain the capability of against blood pressure or shear stress through participating in Ang signalling pathway and impacting on the combination of Ang and Tie2 when Tie1 was at a high phosphorylation level. On the contrary, the low expression of Tie1 would reduce phosphorylation level of Tie1, which would weaken the Ang signalling pathway, impact on the connection of endothelial cells and reduce the capability of against pressure or shear stress. 10
Inspired by the researches above, we assume that there was a certain correlation between the incompetence of venous valve and reduced Tie1 expression in varicose veins disease. In this study, compared with CD31 (a specific marker of endothelial cell) expression, we observed the difference of Tie1 expression on both sides of venous valves. The experimental results seemed to support our hypothesis in normal venous valves, both sides of endothelial expressed CD31 well and no significant difference was found between them; endothelial of the proximal side expressed Tie1 stronger than the distal side at valvar basement, but no such difference was found in the cusp.This phenomenon indicated that blood eddy currents under a normal physiological environment can stimulate high expression of Tie1, in order to tighten the connection among the ECs, and maintain vascular endothelium stability; the situation above may be because of the shear stress at the valvar basement caused by blood vortex being stronger than the cusp. In the varicose veins group, we observed more significant alterations in addition to distorted valvar morphous such as stretching and splitting, but compared with the distal side, the expression of CD31 in the proximal side endothelial has been weakened, and the expression of Tie1 reduced significantly. This phenomenon indicated that low expression of Tie1 on the proximal side decreased the connection between the ECs and weakened tissue structure, which result in valvar incompetence function, blood-flow reflux, venous hypertension, anoxia and inflammation in ECs. In sequence, the persisting venous hypertension also expanded the wall, remodelling the shape of valve and aggravated flow refux, forming a vicious circle.That might be one of the mechanisms of varicose pathogenesis.
We also evaluated CD31 and Tie1 on the vein wall, and there seem to be no noticeable differences. Yet, we still do not know which is primary in the pathogenesis of varicose veins, abnormalities of vein wall or venous valves because there are too many factors in the pathogenesis of varicose veins. So we want to see if these valves changes are also expressed in earlier stages of venous disease specifically in C2 patients. However, patients of C2 usual do not need surgery treatment; we can not get the valves samples, so we do not know if valves of C2 patients express Tie1 abnormally. We will investigate this in our later study.
Through semi-quantitative RT-PCR, we found that the mRNA level of Tie1 was much lower in varicose veins compared with normal control. Combining with the result of immunohistochemistry, it seems that there is a significant difference between varicose venous valves and normal valves.
So we used Western blotting for Tie1 protein quantitative analysis on venous valves, and even expected to observe the alteration of Tie1 phosphorylation level. But Western blot could not detect the expression of Tie1 protein in valves, which may be due to the little number of endothelial cells on the valves and Tie1 only expressed by endothelial cells. So the detection for microexpression of Tie1 protein on venous valves should be researched later in this field.
The function and significance of Tie1 signalling in ECs biology are poorly understood now, primarily because of a ligand having been found. Yet a signal transduction pathway for Tie1 demonstrated that proteolytic shedding of the putative ligand-binding area of Tie1 generates a truncated receptor still capable of ligand-independent signalling. 11 A recent study shows that downregulation of Tie1 in ECs exposed to shear stress in vitro is also accompanied by receptor cleavage. 12 Thus, Tie1 may participate in mechanotransduction of vascular microenvironments experiencing disturbed flow without an exogenous ligand.13,14
Latest research shows that Tie1 also participates in the process of intimal inflammation directly, which plays an important role in the occurrence and development of atherosclerosis in mice model. 15 This indicated the phenomenon that venous valves expressing Tie1 gene abnormally in varicose veins may have a more complex molecular biology role; maybe it is an important reason to cause venous thrombosis and inflammation at a later stage of varicose vein. With regard to the relationship between Tie1 gene mutation and varicose vein, we will discuss in correlated experiments based on larger samples.
Footnotes
Acknowledgements
We thank Dr Yulong He of Nanjing University for the helpful discussion about the work, and Bin Shen, Yanlan Cao and all the staff in Drum Tower Hospital for excellent technical assistance. This work was financially supported by donation from the Key Medical Person Foundation of JiangsuProvince, China.