
Abstract
The aim of this study was to investigate the diameters of the superficial femoral artery (SFA) and the popliteal artery (PA) in patients with type I aneurysmosis (diffuse aneurysm in the aortoiliac-common femoral segments combined with arteriomegaly of the femoropopliteal segments). The ratio between these diameters (SFA/PA index) was calculated. A retrospective study was carried out on 76 limbs of 38 patients with type I aneurysmosis. The SFA/PA index calculated on these patients was compared with the index of a control group: 76 limbs of 38 patients with abdominal aortic aneurysm. The SFA/PA index proved to be < 1.00 in the limbs of patients with type I aneurysmosis, whereas it was ≥ 1.00 in all patients with an abdominal aortic aneurysm. There was a statistically significant difference between the type I aneurysmosis group and the control group (p < .001). This finding can be considered a complementary sign in the diagnosis of type I aneurysmosis.
As we have already stated, confusion often occurs among three different conditions of arterial dilatation, both in clinical practice and in the literature. 1 These conditions are aneurysm, arteriomegaly, and aneurysmosis, and they have several practical and scientific implications, as reported in various studies. 2–7 Although aneurysms are easily recognizable, unfortunately, to date, arteriomegaly and aneurysmosis are not well known. Arteriomegaly, a term coined by Lea Thomas in 1971, 8 defines a condition of diffusely enlarged vessels. The term “aneurysmosis” was first used by Trippel, as reported by Beal in 1968, 9 to denote a diffuse aneurysmal disease. Finally, in 1983, Hollier and colleagues recognized and clearly described this distinct pathologic entity, which is characterized by diffuse aneurysmal disease in patients with arteriomegaly, which they later called “aneurysmosis.” 2,3,5 Their classification describes three types, depending on the location and extent of the aneurysmal disease: type I includes aneurysms of the infrarenal aortic, iliac, and common femoral arteries with arteriomegaly of the superficial femoral artery (SFA) and popliteal artery (PA); type II includes aneurysms of the common and superficial femoral and popliteal arteries with arteriomegaly of the aortic and iliac arteries; and type III includes aneurysms of the infrarenal aortic, iliac, femoral, and popliteal arteries with arteriomegaly of the arterial segments that are not aneurysmal. This classification has been adopted by other authors 4,6 and by us, 7 but the disease and its incidence are still poorly understood.
Although the suggested standards for reporting on arterial aneurysms published in 1991 10 did not mention aneurysmosis, we believe that this pathologic entity still warrants scientific attention to improve clinical and basic knowledge. Paying attention to this entity in clinical practice has allowed us to notice that the diameter of the superficial femoral artery is smaller than the diameter of the popliteal artery in patients with type I aneurysmosis.
The aim of our study was to verify this peculiar finding by means of a retrospective analysis of our cases. If proved, this finding could be used as a complementary sign for the diagnosis of type I aneurysmosis, a condition that is frequently mistaken for aneurysm.
Methods
Type I aneurysmosis in this study was considered a pathologic entity according to the definition by Hollier and colleagues: that is, diffuse aneurysms involving at least three arteries in the aorto-ilio-common femoral segment (eg, infrarenal aorta, common iliac, and common femoral arteries) with arteriomegaly of the femoropopliteal segments. 2 These presented diameters were greater than the values of the normal ones according to our measurements in a consecutive series of healthy subjects (Table 1). Patients with multiple aneurysms (eg, aneurysms of the abdominal aorta and common femoral arteries with other arteries of normal diameter) and/or with PA aneurysms were excluded. Patients with type I aneurysmosis and femoropopliteal obstructive arterial disease were not included in this group.
Diameters of the Superficial Femoral (at Mid-thigh) and Popliteal Arteries (at the Level of the Intercondylar Notch of the Femur) in a Consecutive Series of 38 Normal Subjects*
*Thirty-six males and two females, aged 50 to 86 years (mean age 67 ± 6 years).
Patients with type I aneurysmosis were compared with patients with abdominal aortic aneurysm (on the basis of the standards of the Society for Vascular Surgery and the International Society for Cardiovascular Surgery 10 ) and a femoropopliteal segment with a normal diameter. This group did not include patients with a concomitant PA aneurysm and/or femoropopliteal obstructive arterial disease.
Therefore, we retrospectively studied all consecutive patients referred to our vascular surgery unit for type I aneurysmosis from January 1990 to June 2003, as well as a series of patients with abdominal aortic aneurysm who were used as controls. Two groups were taken into consideration:
Group 1 consisted of 76 limbs of 38 patients with type I aneurysmosis (37 males and 1 female, aged 53 to 78 years, average age 68 ± 4 years) Group 2 consisted of 76 limbs of 38 consecutive patients with abdominal aortic aneurysm (36 males and 2 females, aged 52 to 80 years, average age 70 ± 2 years)
Evaluation of all cases included ultrasound examination of the abdomen, computed tomographic angiography from the diaphragm to the common femoral arteries, and duplex scanning of the arterial system from the abdominal aorta to the infrapopliteal arteries.
Duplex scanning was used to evaluate the diameter of the SFA with the patient in a supine position. The diameter of the PA was measured with the patient in a prone position. Ultrasound scanning equipment (AU4, Esaote Biomedica, Genova, Italy) with a 7.5 MHz B-mode real-time linear-array transducer was used. Measurements were carried out according to the established technique. 11 Each diameter was measured by a radiologist three times, and the results are shown as mean ± SD. The intraobserver variability of this measurement method was very small; the variability for both groups was 0.15 mm and 0.10 mm for the SFA and the PA, respectively (coefficient of variation < 2%).
The following parameters were studied in all of the limbs of the two groups: The diameter of the SFA at mid-thigh The diameter of the PA at the level of the intercondylar notch of the femur The SFA-to-PA ratio, expressed as the SFA/PA index
All data are expressed as mean ± SD, and statistical analysis was performed using the unpaired Student's t-test. A level of 5% was considered statistically significant.
The two groups were also compared with regard to gender, age, height, weight, blood pressure, and body surface area (BSA), which was calculated by the Du Bois formula (BSA cm2 = weight 0.425 kg × height 0.725 cm × 71.84). The chi-square test was used to compare percentages, whereas the Student's t-test for unpaired data (level of statistical significance < .05) was used for comparison between averages.
Moreover, the two groups were compared with regard to risk factors (carotid disease, coronary artery disease, hypertension, smoking, diabetes, hyperlipidemia, obstructive airways disease) using the chi-square test to compare percentages (level of statistical significance < .05).
The SFA/PA index was evaluated as a test to identify patients with type I aneurysmosis. The sensitivity, specificity, positive predictive values, negative predictive values, and accuracy of this test were calculated.
Follow-up of the two groups of patients was carried out to evaluate the occurrence of subsequent aneurysmal disease in other sites. The two groups were also compared with regard to this event using the chi-square test to compare percentages (level of statistical significance < .05).
This study was approved by the local ethical committee, and there was no conflict of interest.
Results
No statistical significance (p > .05) was found between the two groups as far as gender, age, height, weight, BSA, and blood pressure were concerned.
Table 2 shows the risk factors for each group. No significant differences (p > .05) were observed when group 1 was compared with group 2.Table 3 shows the data regarding the diameters in the two groups we studied.Figure 1 shows the distribution of the values of the SFA/PA index in the two groups.
Risk Factors for Patients with Type I Aneurysmosis (Group 1) and Patients with Abdominal Aortic Aneurysm (Group 2)
No statistically significant difference (p > .05) between the two groups.
Diameters of the Superficial Femoral and Popliteal Arteries in the Limbs of Patients with Type I Aneurysmosis (Group 1), and of Patients with Abdominal Aortic Aneurysm (Group 2)
*Significant difference (p < .05).
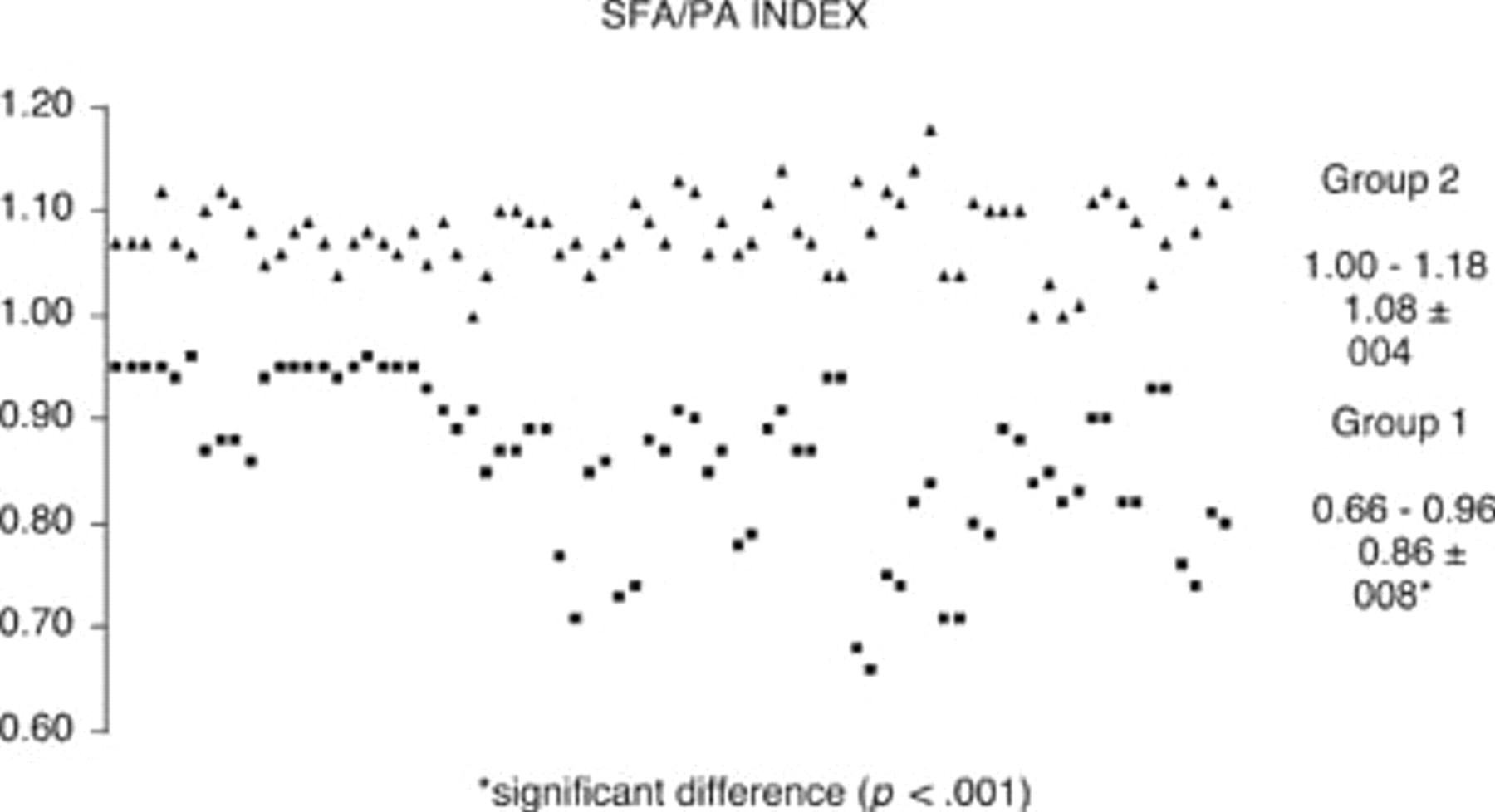
Values of the ratio between diameters of the superficial femoral artery (SFA) and the popliteal artery (PA), called the SFA/PA index, in the limbs of patients with type I aneurysmosis (group 1) and of patients with abdominal aortic aneurysm (group 2), and their range and mean ± SD.
In group 1 (limbs of patients with type I aneurysmosis), the SFA/PA index was < 1.00 in all cases, whereas in group 2 (limbs of the subjects with abdominal aortic aneurysm), it was always ≥ 1.00. Moreover, the differences in mean ± SD of the SFA/PA index between group 1 and group 2 are statistically significant (p < .001).
The sensitivity, specificity, positive predictive values, and negative predictive values of the SFA/PA index are 100%, taking into account the value of 1.00 as the threshold for identifying patients with type I aneurysmosis. The SPA/PA index provided 100% accuracy.
Follow-up at 10 years was reached for 22 patients with type I aneurysmosis and 26 patients with abdominal aortic aneurysm. Subsequent aneurysms (of the internal iliac artery in 2 and of the femoropopliteal segment in 9) were seen in 11 cases of type I aneurysmosis and (of the internal iliac artery in 2 and of the popliteal artery in 2) in 4 cases of abdominal aortic aneurysm over this period. The difference between the two groups (11/22, 50%, vs 4/26, 15%) is statistically significant (p < .05).
Discussion
Type I aneurysmosis is easily mistaken for an aneurysm because of the lack of attention to the diffuse arterial dilatation of aneurysmosis, whereas an aneurysm is a localized dilatation, and the coexisting arteriomegaly of the femoropopliteal segments.
As recently stressed by Sandgren and colleagues, to evaluate whether an artery is pathologically dilated, the normal diameter must be known. 12,13 Under normal conditions, proceeding distally, the diameter of the arterial system progressively decreases. In fact, Hollier and colleagues reported 7 and 6 mm for the SFA and the PA, respectively. 2 Callum and colleagues observed 6.8 and 6.0 mm correlated to age and sex. 14
The average diameters of our own patients with type I aneurysmosis (group 1) with femoropopliteal arteriomegaly were 9.8 ± 0.8 mm for the SFA and 11.4 ± 1.0 mm for the PA. These data show a statistically significant difference (p < .05) compared with the diameters of our control group without arteriomegaly (7.6 ± 0.4 mm and 7.1 ± 0.3 mm for the SFA and the PA, respectively). Moreover, as far as comparison of diameters is concerned, the diameters of our group 1 patients are greater than the ones reported by the aforementioned authors. 2,14
In our study, the SFA/PA index was below 1.00 in patients with type I aneurysmosis. This is a recurrent finding in type I aneurysmosis that we would like to stress.
We know that under normal conditions, if we proceed distally, the diameter of the arterial system progressively decreases. In fact, by applying our SFA/PA index to the normal values of the arterial diameters reported in the literature, this index is greater than 1.00. For example, if we apply the ratio of the diameters found by Callum and colleagues 14 between the SFA (6.8 mm) and the PA (6.0 mm), the result is equal to 1.13. These data show that the diameter of the SFA is smaller than the diameter of the PA in patients with type I aneurysmosis. Therefore, the SFA/PA index is < 1.00.
Contrary to observations that have been reported, an SFA/PA index below 1.00 (0.86 ± 0.08) was found in the femoropopliteal segments of our group 1 patients with type I aneurysmosis. Differences in the SFA/PA index between group 1 (type I aneurysmosis) and group 2 (controls) proved to be statistically significant (p < .001).
Therefore, this index can be considered a complementary sign in the diagnosis of type I aneurysmosis. The accuracy of this index as a diagnostic test for type I aneurysmosis was very high (100%).
The clinical relevance of this sign is in its ability to quickly and accurately identify patients with type I aneurysmosis and to distinguish them from the ones with abdominal aortic aneurysm.
Moreover, in our experience, the SFA/PA index has demonstrated important prognostic relevance. An index < 1.00, as was observed in the group with type I aneurysmosis, proved to be a predictive marker for the occurrence of subsequent aneurysms, especially in the femoropopliteal segment.
Recently, a study by Sandgren and colleagues suggested that the generalized vascular dilating diathesis (or arteriomegaly) that is seen in some patients seems to be a specific entity that is not necessarily affiliated with abdominal aortic aneurysm alone. 15 This study might be considered strong support to the theory of aneurysmosis (generalized vascular dilating diathesis with aneurysms) as a specific entity.
In conclusion, owing to the fact that the diameter of the SFA is smaller than the diameter of the PA in patients with type I aneurysmosis, the SFA/PA index (< 1.00) is both a complementary, specific sign of the diagnosis of type I aneurysmosis and a further contribution toward defining this pathologic entity. Further studies are needed to confirm our results and to identify the biochemical and genetic basis of this particular finding.
On the basis of our results, we are even more convinced that aneurysmosis must be considered a distinct entity. Therefore, the classification of aneurysmal disease should be revised to include the category of aneurysmosis, and three pathologic arterial conditions must be taken into consideration: (1) aneurysm, which is localized arterial dilatation; (2) arteriomegaly, which is generalized enlargement of the entire arterial system without aneurysm; and (3) aneurysmosis, which is diffuse aneurysmal disease in patients with arteriomegaly.