
Abstract
We describe the successful use of hydration with sodium bicarbonate and N-acetylcholine to prevent contrast-induced nephrophathy in a patient with a kidney transplant undergoing endovascular native renal artery aneurysm exclusion. The implications for surveillance studies for endovascular procedures are discussed.
Prevention of contrast-induced nephrophathy (CIN) and deterioration of renal function are important in all patients, particularly in patients with preexisting renal insufficiency. Generally recognized preventive measures include use of alternative contrast agents, such as carbon dioxide, and use of alternative imaging techniques, such as duplex ultrasonography. If iodinated contrast media is required, protective measures that can be used include using the minimal dose necessary for adequate imaging, adequate hydration, treatment with N-acetylcholine (NAC), and use of low-osmolar contrast media (LOCM).
Although the use of hydration and NAC in the prevention of CIN is well established in patients with preexisting renal insufficiency, 1,2 there are few guidelines regarding use in patients who have previously received a kidney transplant. There are few data describing the incidence of CIN in renal transplant patients; however, these patients may be particularly vulnerable to CIN owing to the underlying disease that originally produced their end-stage renal disease and the potential interactions with medications that may produce synergistic renal toxicity with the administration of contrast. We describe the successful use of hydration with sodium bicarbonate and NAC to prevent CIN in a patient with a kidney transplant undergoing endovascular native renal artery aneurysm exclusion.
Case Report
A 55-year-old, 209-pound man with Alport's syndrome and a 22-year history of successful renal transplant presented with abdominal pain. A computed tomographic (CT) scan revealed an aneurysm in the native left renal artery. An abdominal aortogram and a selective left renal arteriogram demonstrated a large aneurysm arising from the proximal left renal artery; the aneurysm lumen was 33 × 30 mm, without any patent outflow vessels (Figure 1, A and B). The aneurysm neck was 10 mm, reducing the certainty of successful aneurysm coiling and increasing the risk of coil prolapse into the aorta. One week later, an AneuRx 26 mm–diameter by 3.75 cm–long aortic cuff (Medtronic AVE, Sunnyvale, CA) was placed in the aorta, using an endovascular approach via the left femoral artery, to successfully cover the left native renal artery orifice and exclude the aneurysm. A conventional stent graft was not placed because no abdominal aortic aneurysm was present and to minimize endovascular manipulation, and potential embolism or dissection into, the transplanted kidney present in the right iliac artery.
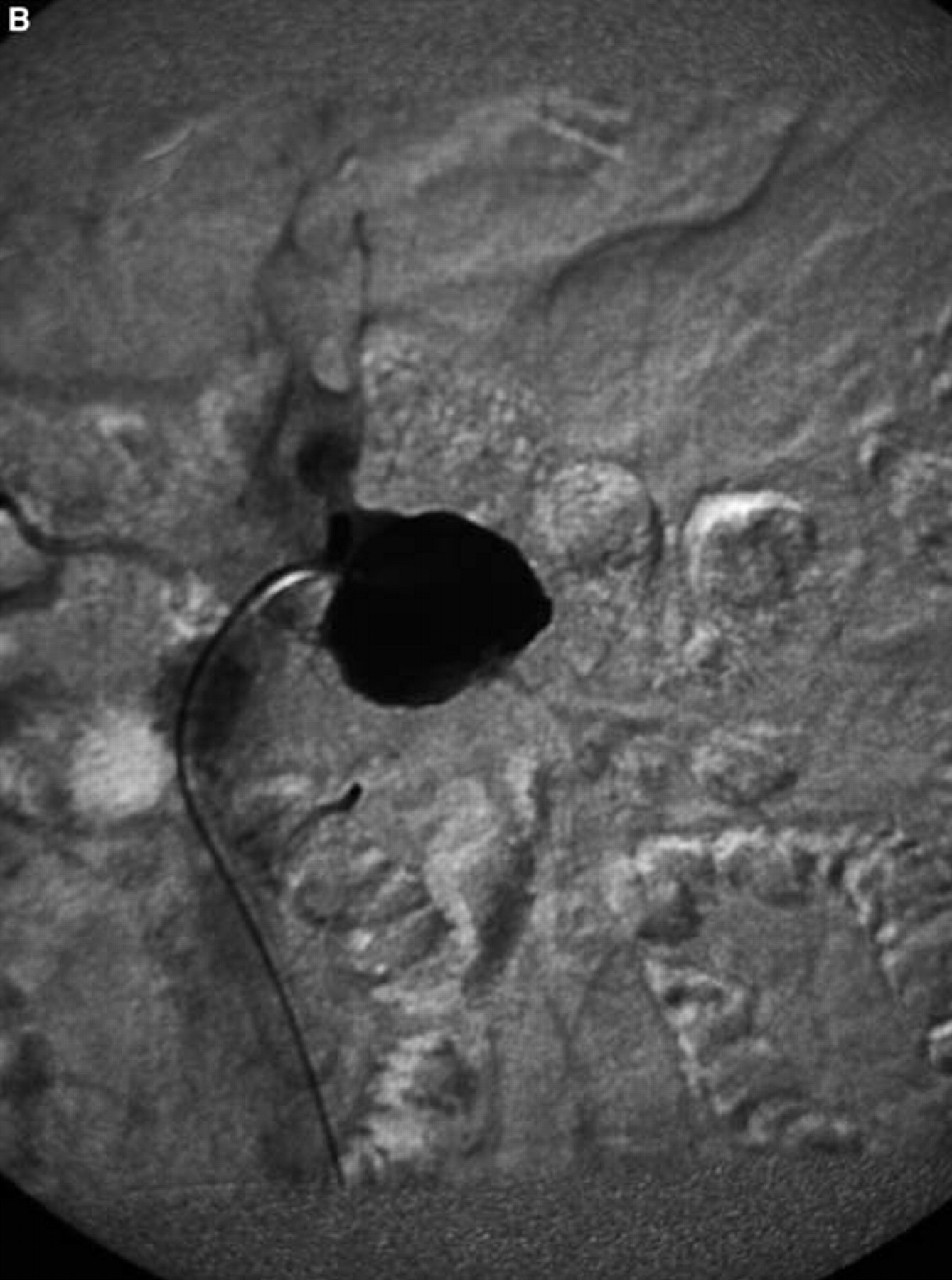
A, Angiogram of the aorta, demonstrating aneurysm in the origin of the native left renal artery, without any patent outflow vessels. The origin of the right renal artery fills. B, Selective angiographic view of the left renal artery aneurysm, demonstrating no patent outflow vessels.
The patient's baseline serum creatinine and estimated creatinine clearance were 1.4 mg/dL and 80.3 mL/min, respectively, before the arteriogram and aortic cuff placement on day 1 of his treatment course (Figure 2). One dose of 600 mg NAC was administered the morning of the arteriogram and another dose after the procedure. Two more doses were administered the next day. Additionally, the patient was hydrated with dextrose 5% in water (with 150 mEq sodium bicarbonate) at a rate of 1.05 cc/kg/h for the day of the arteriogram, for a total of 1.8 L of fluid. For the abdominal aorta endovascular stent graft procedure on day 8 of the treatment course (see Figure 2), the patient received two doses of 600 mg (3 mL) NAC the day before the procedure, one dose the evening after the procedure, and a final dose the following morning. The patient was hydrated with dextrose 5% in water with 150 mEq sodium bicarbonate before and after the endograft procedure at a rate of 0.82 cc/kg/h, for a total of 2.6 L of fluid. The patient received 50 cc of Omnipaque 300 during the arteriogram and 60 cc during the endovascular procedure.
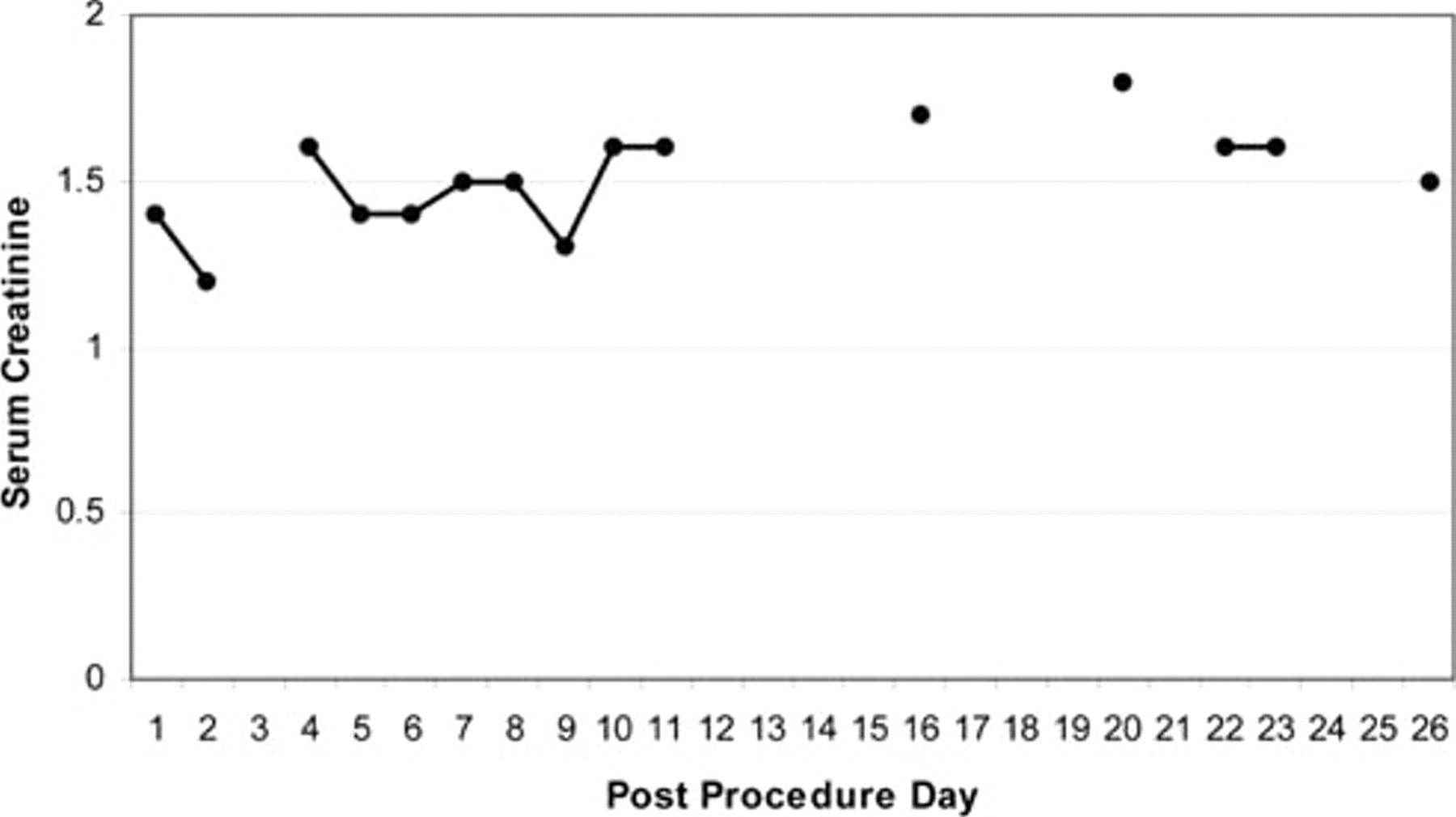
Graph of serum creatinine after endovascular exclusion of the left renal artery aneurysm.
Throughout the time period, including the morning of the arteriogram until 72 hours after the endovascular operation, the patient's serum creatinine varied from 1.3 to 1.6 mg/dL, from a baseline of 1.4 mg/dL measured immediately before the arteriogram. Since the definition for CIN is an increase of either ≥ 25% from baseline or an absolute increase from baseline of ≥ 0.5 mg/dL within 72 hours of administration of iodinated contrast media, this patient never met the criteria for CIN. Using the formula for estimated creatinine clearance, (140 − age [yr] × weight [kg]/[72 × serum Cr [mg/dL]), the patient's estimated creatinine clearance varied from 86.5 to 70.3 mL/min, consistently below the normal range (normal range 90–136 mL/min). In a subsequent hospitalization for fever on postprocedure day 20, for catheter-related urosepsis, the serum creatinine levels peaked at 1.8 mg/dL (see Figure 2). This value is ≥ 25% above the baseline of 1.4 mg/dL but, at 12 days from the endovascular procedure, also does not meet the criteria for CIN. Of note, the patient was taking azathioprine and prednisone to prevent rejection of the renal graft and was, therefore, immunosuppressed during this time.
Almost 1 year after the procedure, the renal artery aneurysm remained successfully excluded, with a smaller thrombus-filled sac without any evidence of flow; there was no evidence of stent graft migration (Figure 3). The creatinine was 1.6 mg/dL.
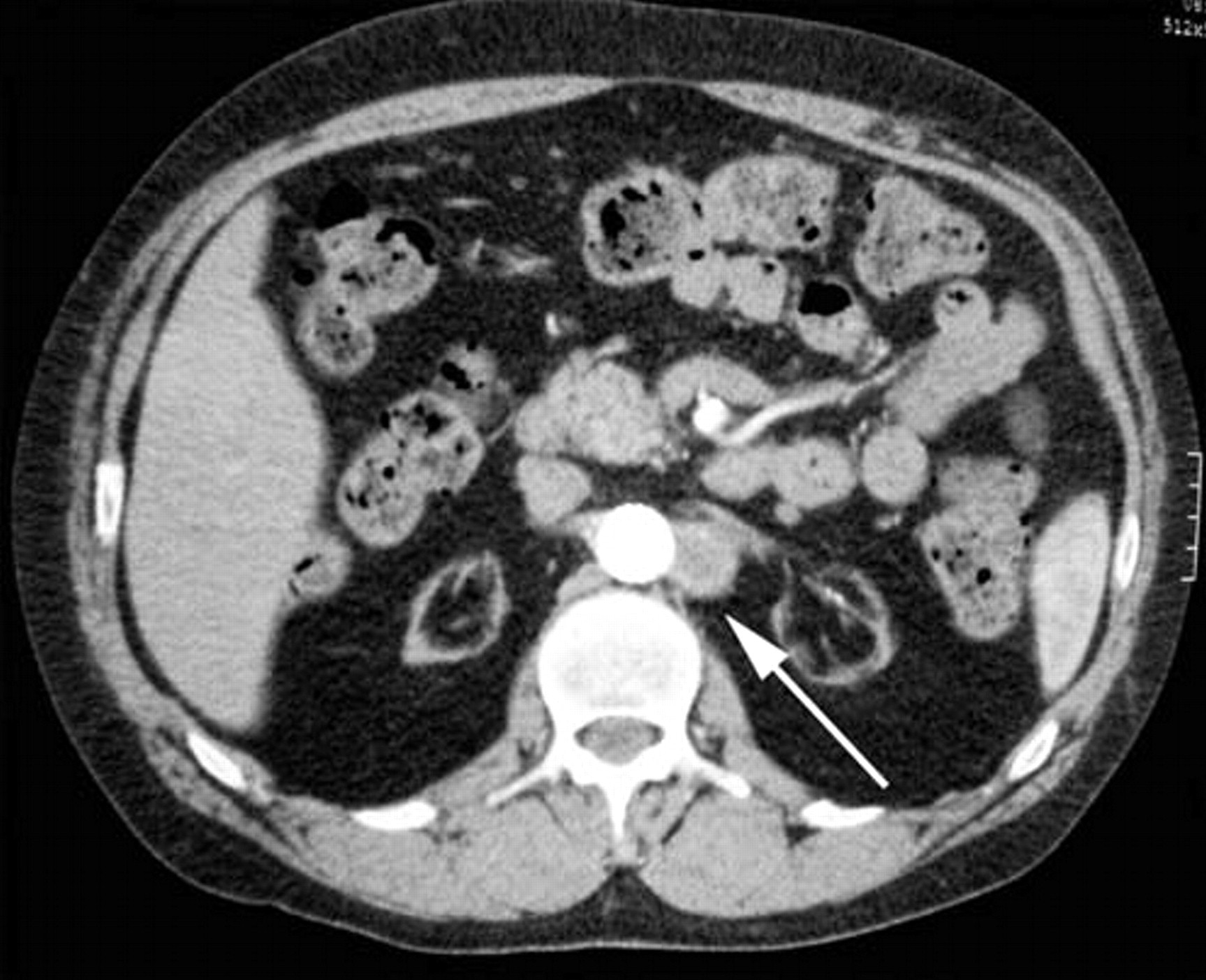
Computed tomographic image of an excluded aneurysm, with a smaller residual sac, in follow-up. The arrow points to the residual excluded left renal artery aneurysm, without contrast.
Discussion
The use of NAC and hydration for the prevention of CIN has been studied in patients with chronic renal insufficiency. Tepel and colleagues reported the incidence of CIN among patients with chronic renal failure undergoing CT scans; patients treated with NAC and hydration had a 2% incidence of CIN compared with 21% in patients treated with hydration alone. 3 Other studies have shown a protective effect of NAC and hydration compared with hydration in patients undergoing cardiac catheterization and coronary artery angioplasty. 4,5 Several studies have not shown a protective effect, 6,7 but meta-analysis of randomized controlled trials has concluded that NAC is beneficial when used with hydration to prevent CIN in patients with chronic renal insufficiency. 1,2
Kidney transplant recipients may be particularly vulnerable to CIN following administration of iodinated contrast media because of high rates of diabetes, renal insufficiency, and the use of cyclosporine. Although this has not been widely studied, in 2000, Ahuja and colleagues found that the incidence of CIN was 21.2% (7 of 33 patients) in a retrospective study of renal allograft recipients undergoing intravenous or intra-arterial contrast studies. 8 In patients who received intravenous hydration, the rate was 15.3% (4 of 26) compared with 42.8% (3 of 7) in patients who did not receive hydration. Other studies have shown that carbon dioxide and gadolinium-based contrast media are potentially safe and effective alternatives to iodinated contrast media for endovascular procedures in patients with renal insufficiency. 9 It has also been shown that the use of LOCM can decrease the incidence of CIN in comparison with high-osmolar contrast media, and iso-osmolar contrast media are potentially safe. 10 When administering iodinated contrast media, hydration and LOCM help prevent CIN in individuals with chronic renal insufficiency.
The crystalloid fluid used for hydration is often normal saline, although a recent report described the beneficial effect of sodium bicarbonate in preventing CIN. 11 We used sodium bicarbonate for hydration in concert with NAC; therefore, the particular effects of sodium bicarbonate and NAC cannot be distinguished. However, the use of both sodium bicarbonate and NAC appeared to be safe in our patient. Our patient did have a transient small rise in serum creatinine temporally related to an episode of catheter-related sepsis. Although we cannot exclude a self-limited, delayed contrast reaction, this would be unusual. In addition, this temporary creatinine elevation was unlikely owing to left renal infarction from the procedure because the aneurysm had no outflow vessels and the kidney had no preprocedural function owing to the patient's long-standing Alport's syndrome.
Patients who require studies to monitor endovascular grafts, such as the patient reported here, are often vulnerable to CIN with each contrast study, which may be substantial over time. Although there is no clear consensus, some have suggested baseline CT angiography at discharge, biphasic CT angiography and duplex ultrasonography at 3 months, and yearly CT angiography, plain films, and duplex ultrasonography. In patients with renal insufficiency, magnetic resonance angiography may offer an alternative. 12 Although these patients will be exposed to multiple studies to monitor stent grafts, an effort should be made to minimize exposure to iodinated contrast media by using alternative contrast agents, such as carbon dioxide, or using alternative imaging techniques, such as duplex ultrasonography. The use of gadolinium, however, is controversial and may not be recommended in patients with preexisting renal impairment. 13 If iodinated contrast media is required, protective measures that can be used include use of the minimal dose necessary for adequate imaging, adequate hydration, possibly with sodium bicarbonate, treatment with NAC, and use of LOCM. Further study of the protective effect of NAC, with and without sodium bicarbonate, is required to guide the use of iodinated contrast media in renal transplant patients and minimize CIN.