
Abstract
The association between type 1 diabetes mellitus and autoimmune thyroid disease is well documented in the literature. Both can coexist although one endocrinopathy usually precedes the other. The simultaneous new onset of both diseases is rarely seen. Hyperthyroidism can precipitate and complicate the management of diabetic ketoacidosis by masking its classical clinical features. Persistent tachycardia after correction of acidosis and dehydration, may be the only suggestion of another coexisting illness such as thyrotoxicosis. We describe the case of a previously healthy woman who developed new onset type 1 diabetes mellitus and Craves’ disease, and presented with diabetic ketoacidosis.
Introduction
The association between type 1 diabetes mellitus and autoimmune thyroid disease is well known. Both can present concurrently, atypically and as fulminant medical emergencies. Successful management of diabetic ketoacidosis depends on the prompt recognition and treatment of all concurrent precipitants.
Case report
A 56-year-old woman, with a no significant past medical history, presented with a one-month complaint of increased fatigue, anxiety, polyuria, polydipsia and palpitations associated with 7 kg weight loss. In the 24 hours prior to admission, she had developed abdominal pain and vomiting. She denied any infective respiratory symptoms. A notable family history of type 1 diabetes and hypothyroidism was present.
On presentation, she was extremely lethargic and ketotic, and displayed signs of Kussmaul's breathing. Her respiratory rate was 34 breaths/minute, heart rate 130 bpm, blood pressure 112/65 mmHg, temperature 38.0°C and Glasgow coma score (GCS) reduced at 14. Her clinical examination revealed dry mucous membranes and reduced skin turgor without pigmentation; unilateral exopthalamos was suspected but no goitre was palpable. There was no tremor evident at this point. Chest auscultation revealed bilateral basal crackles – thought to be due to aspiration. Electrocardiogram showed sinus tachycardia and chest X-ray confirmed minor bibasilar alveolar shadowing. Initial arterial gas analysis and biochemistry, demonstrated a marked metabolic acidosis with hyperglycaemia and dehydration alongside raised inflammatory markers (Table 1). Urinalysis was strongly positive for glucose and ketones.
Laboratory data summary
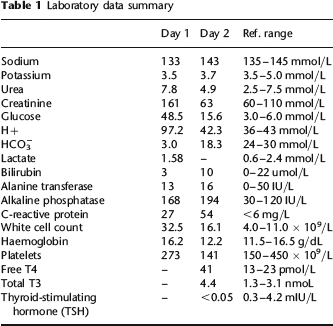
The treatment of diabetic ketoacidosis was initiated with insulin infusion alongside fluid and electrolyte replacement as per local protocol. 1 Empirical intravenous antibiotics were commenced to cover for any potential infective precipitant. Due to the reduced GCS on admission, the severity of the acidosis, and the suspicion of sepsis, transfer to intensive care was arranged.
On day 2, her tachycardia persisted despite correction of her dehydration (evidenced by normalized renal function after over 5 L of fluid resuscitation), rectification of her hyperglycaemia and resolution of her acidosis. A new postural tremor was now noted. Thyrotoxicosis was suspected and subsequently confirmed by thyroid function tests (Table 1). She was commenced on propanolol and Carbimazole. By the third day, the acidosis, tachycardia and tremor had resolved and the patient was stepped down from intensive care to a general medical ward, and discharged from hospital by the fifth day with daily requirements of subcutaneous mixed analogue insulin, propanolol and Carbimazole.
Further immunological results revealed raised antithyroid peroxidase titres; antiadrenal and antitissue transglutaminase antibodies were negative. The thyroid function tests normalized within two months of discharge. Our patient was diagnosed as having a simultaneous new presentation of both type 1 diabetes mellitus and Graves’ disease.
Discussion
The association between type 1 diabetes and thyroid disease is well documented; approximately one-third of patients with type 1 diabetes possess antithyroid antibodies. 2 A shared genetic susceptibility has been identified around the HLA D3 haplotypes. 3 The association is greatest in adolescents and also with white Caucasian women - such as our patient.
To our knowledge, the simultaneous new onset of thyrotoxicosis and diabetes presenting as concurrent endocrine emergencies, has been seen only rarely in the literature.4,5
Diabetic ketoacidosis can be precipitated by hyperthyroidism and vice versa. Our case refreshes the association between the two and underlines the need to search after both causes, particularly in female patients – where the prevalence is higher – and especially where there is a relevant family history. Detection may be difficult as the clinical features of both conditions – such as weight loss – will overlap and other features may be masked. In our case, the features of tremor were initially obscured by dehydration and exhaustion. The presence of persistent tachycardia despite correction of dehydration and acidosis was one of the key signs to suggest underlying thyroid pathology. Unilateral exopthalamos was present in this case but such subtle clinical clues can be missed in an acutely unwell patient with a lowered GCS. Notably, no goitre was evident to suggest thyroid disease.
The prompt recognition of a dual endocrinopathy is essential as the hyperthyroid state will impair glycaemic control, worsen acidosis and disrupt the fluid and electrolyte balance.
Thyroid hormones induce a hypercatabolic state where basal hepatic glucose production is increased, insulin production is reduced and the peripheral effects of insulin are lessened while its rate of degradation is accelerated. These factors collectively raise the total body insulin requirement. The use of propanolol, further exacerbates glucose intolerance. 6 The hyperthyroid state promotes lipolysis in adipose tissues and sensitizes cells to circulating catecholamines. The fatty acids subsequently released, undergo hepatic beta oxidation and are converted to ketones which worsen acidaemia. 7 Hyperthyroidism can directly cause hypokalaemia by direct activity on cellular Na/K-ATPase pumps. If exogenous insulin is administered to treat diabetic ketoacidosis, it will further exacerbate this deficiency. 8 Thyrotoxicosis will worsen fluid losses by increasing in the basal metabolic rate and exacerbate the fluid deficits which have arisen from a hyperglycaemia-induced osmotic diuresis. Thyroid-related sympathetic stimulation of the heart, combined with volume depletion, can induce cardiac failure.
In previous case studies, the deleterious effects of unchecked acidosis, prolonged tachycardia and uncorrected hypokalaemia, have led to ventricular arrhythmias and cardiac arrest. 9 If both endocrine emergencies present simultaneously, the emphasis is placed on rigorous fluid balance and electrolyte monitoring. Some authors have also suggested the pre-emptive use of bicarbonate therapy, although we did not need to use it. 10
Our case emphasizes that new onset diabetic ketoacidosis and hyperthyroidism can present concurrently, and one disease can mask the features of the other, thereby making diagnosis difficult. In a case of type 1 diabetes, persistent tachycardia after correction of acidosis and dehydration should prompt a search for other illnesses like thyrotoxicosis. In such cases, early institution of insulin and fluid replacement alongside antithyroid drugs are essential to successful management.