
Abstract
Ideally those at highest risk of fracture should be identified prior to fracture occurrence to reduce mortality, morbidity and costs. Case-finding strategies for those at high risk of first fracture or systematic case-finding strategies following fracture are recommended in the UK, rather than population-based screening to identify individuals at high fracture risk. General practices in the UK hold relevant data on individuals beyond fracture history that could allow identification of a wider group of patients at highest risk of fracture. The aim of the paper is to evaluate the feasibility of applying the WHO-FRAX fracture risk calculator to general practice populations using existing recorded data. A cross-sectional study of 2467 women aged 50 years and older (mean 66.2 years, standard deviation = 11.3) registered with two Scottish General Practices with low deprivation (one semi-rural, one urban) was undertaken. Patient data were extracted from the two general practices’ patient information databases and the WHO-FRAX calculator was applied to these data. WHO-FRAX calculation was possible on 1872 patients. Of these, 687 patients were found to have a high fracture risk (risk of major facture ≥15% and or risk of hip fracture ≥3% – 37% of the WHO-FRAX assessed cohort) and should be considered for follow-up. In conclusion, use of the WHO-FRAX calculator using general practice-held data is feasible and can help to identify a patient group at higher fracture risk. Further evaluation and treatments can then be targeted at this group.
Introduction
Osteoporosis-related fractures are a major cause of morbidity and mortality.1–3 One in two women and one in five men will suffer a fracture after the age of 50 years. 4 The annual incidence of fractures in the UK is estimated at 310,000 with costs of some £1.8 billion in 2000 rising to £2.2 billion by 2020. 5
The appropriate use of bisphosphonates has been shown to reduce the risk of vertebral, non-vertebral and hip fractures, both in patients who have never fractured before and in those who have already sustained one or more fractures.6,7 However, the majority of patients who are at high risk of fracture are currently undiagnosed and/or untreated.8,9
Case-finding tools can be used to select patients who are at a high risk of fracture for referral for dual energy X-ray absorptiometry (DXA) scanning to diagnose osteoporosis. Case finding has been shown to be more cost-effective than population-based screening of bone density.7,10 However, case finding has been shown to be specific but not sensitive. 11 Ideally an evaluation tool needs to be sufficiently sensitive to indicate those needing further assessment of fracture risk and yet specific enough to accurately target those for assessment. An ad hoc case-finding approach has generally been the preferred way to identify patients who might be at high risk of fracture 12 although recently, systematic approaches, such as the development of Fracture Liaison Services, have been shown to be more successful. 13 It is now becoming clear that while ad hoc case finding is attractive in principle, this is not an effective way to find high-risk patients. If global fracture risks are to be reduced, then more systematic approaches to case finding need to be developed. 14 While Fracture Liaison Services go some way to identifying a population of patients at higher future fracture risk, there remains a large population who have not sustained a recent primary fracture, but who also have a high future fracture risk. 15
Categorizing fracture risk for individual patients in a primary care setting may address the lack of sensitivity of case finding while avoiding the pitfalls of mass (population) DXA scanning.
WHO-FRAX (www.shef.ac.uk/FRAX) is a computer (web) based algorithm which can be used for the assessment of fracture risk. It can be used both when bone mineral density (BMD) data are and are not available. Risks are calculated over a 10-year interval for major fractures (clinical spine, forearm, hip or shoulder) or for hip fracture alone. WHO-FRAX is designed to be used with the patient in consultation with their clinician.
In the UK, general practices have been computerized for many years and have coded data on their patients. 16 If the correct codes can be extracted from practice population data, then the WHO-FRAX algorithm could be applied to individuals and allow identification of those at high risk of fracture. Further investigation or treatment might then be considered in these patients.
We conducted a study to investigate whether data currently available to general practices are adequate to allow a WHO-FRAX calculation and therefore identify individuals at risk of fracture.
Methods
Two general practices were approached to carry out the study. A semi-rural practice and an urban practice, both with low deprivation (Scottish Index of Multiple Deprivation Score <8%). 17 Both practices have been computerized for at least five years and have scored maximal points in the ‘Qualities and Outcomes’ Framework (QOF) for general practice, suggesting good administration and data recording. Both practices use GPASS (General Practice Administration System for Scotland; www.gpass.scot.nhs.uk), the government supplied and currently the most frequently used GP software in Scotland.
Data (which is used in the WHO-FRAX risk calculator) were extracted from both practices for women aged 50 years and above. These data are shown in Table 1.
Data extracted from practices
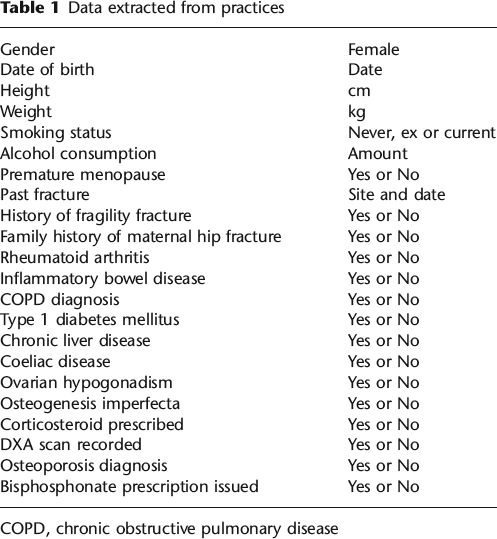
COPD, chronic obstructive pulmonary disease
The extracted data were then manually entered into the WHO-FRAX calculator for each individual, to calculate the 10-year major fracture risk and hip fracture risk.
The records of 2464 female patients aged over 50 years were reviewed. ‘High risk’ of fracture was defined in this study (as per the Greater Glasgow and Clyde Osteoporosis Service) as a greater than 15% risk of major fracture 18 or greater than 3% risk of hip fracture in the next 10 years. 19 Where a choice is to be made, major fracture risk is preferred to hip fracture when considering treatment thresholds. 20
Results
Collation of data within practices
The two practices had similar levels of data recording and disease prevalence, and thus the data were combined (Table 2).
Absolute number and percentage of individuals with information recorded
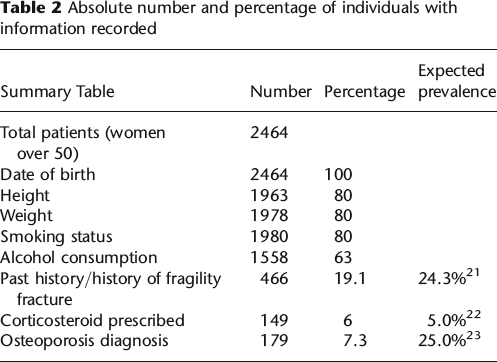
WHO-FRAX includes a section for conditions associated with secondary osteoporosis and with this in mind, the practices’ prevalences were in keeping with the national expected prevalences for the conditions type 1 diabetes mellitus, 24 rheumatoid arthritis, 25 inflammatory bowel disease, 26 chronic liver disease, 27 chronic obstructive pulmonary disease 28 and coeliac disease29,30 (data not shown). Corticosteroid script prevalence was near the national recorded prevalence. 22 The prevalence of identified osteoporosis was in keeping with expected recorded figures, 31 but lower than the true disease burden. 23 The prevalence of previous fractures was in keeping with national figures 21 (19% versus an expected prevalence of 24%).
The national prevalences of premature menopause and ovarian hypogonadism 32 are low, but it appeared that neither practice recorded these data. Osteogenesis imperfecta is a rare condition 33 and neither practice contained an individual with this condition. The national prevalence of a history of maternal hip fracture is 6%, 34 but these data were not recorded by either practice.
The contemporaneous nature of the recorded demographic data was assessed (Figure 1).
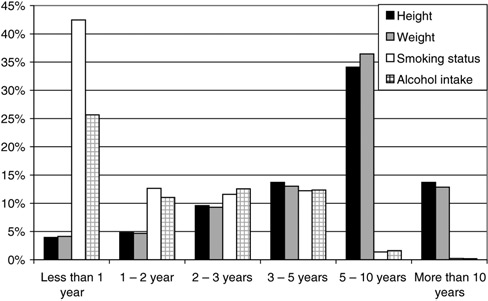
Date of recording demographic data
There were 592 individuals (24%) with no height and/or weight recorded. No WHO-FRAX calculation was performed on these individuals. The remaining 1872 (76%) proceeded to have a WHO-FRAX calculation performed.
Patients identified as high risk of future fracture
Of the 1872 individuals assessed, 513 (27%) had both a 10-year risk of major fracture of >15% and a >3% risk of hip fracture. A further 171 (9%) individuals had a 10-year hip fracture risk of >3% and another three individuals (0.2%) had a 10-year risk of >15% for major fracture. In total, there were 687 patients (37% of the measured cohort) who should be considered for follow-up/further investigation.
Of those in whom WHO-FRAX assessment was possible, 28% (21% of the study cohort) had a 10-year risk of major fracture of greater than 15% (Figure 2).
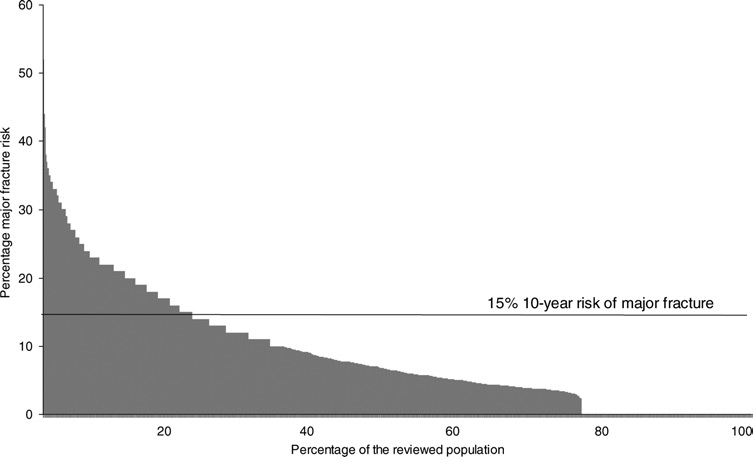
WHO-FRAX calculated 10-year major fracture risk
Of those in whom WHO-FRAX assessment was possible, 37% (28% of the study cohort) had a 10-year risk of hip fracture greater than 3% (Figure 3).
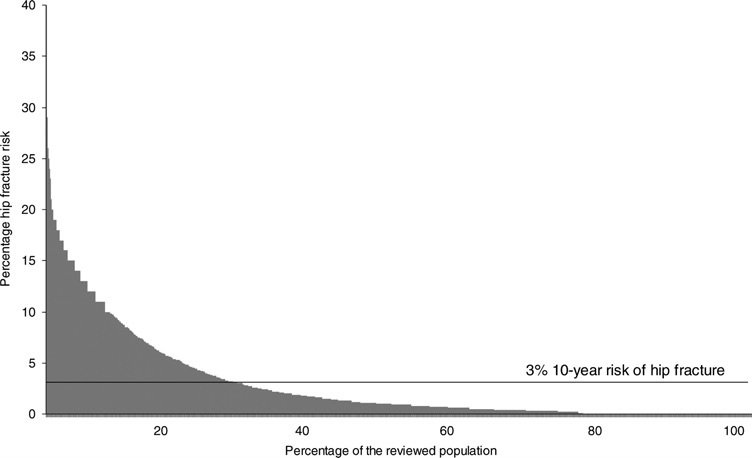
WHO-FRAX calculated 10-year hip fracture risk
Of the 687 individuals who were identified as having a 10-year risk >15% for major fracture or a >3% risk of hip fracture, only 255 individuals (37%) had a fracture history.
Discussion
In this study the WHO-FRAX calculator identified 37% of the patients studied as having a high risk of major fracture, hip fracture or both. The prevalence of identified and recorded osteoporosis (by DXA scanning) in our cohort was 7.3%. This is in keeping with previous studies, 31 but contrasts with the expected disease burden of 25%. 23 Therefore, there is a large group of patients (29.7%) who are at a sufficiently high risk of fracture to justify further investigation and/or treatment. These patients are not being identified and assessed at present.
In theory there is sufficient data held in primary care computerized information systems to identify those at high risk of fracture using WHO-FRAX. Our study's strength demonstrates how WHO-FRAX can readily be applied to patients in general practice, using information already available. Interrogation of a database can only include coded conditions, whereas a face-to-face consultation might enable additional WHO-FRAX parameters to be identified. Any data not considered (when using coded information) will underestimate rather than overestimate fracture risk. It follows that the patients with the highest risk would be identified if WHO-FRAX was used as a screening tool.
We found that the two practices in this study had sufficiently accurate coded data to enable WHO-FRAX to be used as a screening tool. However limitations existed. Most general practices take a pragmatic approach to coding data and rather than coding all data, only code information that may be useful or affect clinical care. Of the cohort in this study, 24% could not be assessed due to missing data. In general, smoking, alcohol history, height and weight data are all well recorded, but these data are often not contemporary. This limited the accuracy and ability to perform the WHO-FRAX calculation.
Although an ad hoc case-finding strategy has been shown to be more cost-effective than screening of bone density7,10; the opportunistic use of case-finding tools, such as WHO-FRAX or other such tools,11,35 appear to be used rarely. In day-to-day busy practice, such screening is not practical. A current limitation of using the WHO-FRAX algorithm for screening is that it can only be applied individually, making ‘en mass’ application to practice data impossible. Other ways of using the WHO-FRAX tool for groups of patients would need to be developed.
The presence of a fracture history is a risk for future fracture. However, we have demonstrated that identification of these data alone would miss a sizeable cohort (the majority in this study) of those at risk of future fracture and most notably those at risk of their first fracture.
Risk calculators other than WHO-FRAX have been developed. QFractureScores 36 is a newly released fracture risk calculator that might provide an alternative to WHO-FRAX. However, its use in practice has yet to be determined and there are concerns with its construction. 37
Both practices in this study had low deprivation status. In practices with higher deprivation, the quality of coding of data is likely to be similar as in this work. However, if the actual data differed, the levels of fracture risk could be different. A lower socioeconomic status has been shown to increase hip fracture incidence 38 and also to be associated with lower BMD assessment rates. 39
The WHO-FRAX derived fracture probability at which BMD testing or intervention is required, remains controversial. There appears to be wide variation in recommendations. 40 In the UK it is estimated to be cost-effective to offer intervention at a greater than 7% WHO-FRAX major risk of fracture over 10 years. 20 On the other hand, the National Osteoporosis Foundation (USA) recommends that intervention is offered where there is a WHO-FRAX risk of major fracture of greater than 20% over 10 years and hip fracture greater than 3% over 10 years. 40 Clearly a cost-effective intervention is different from a clinically appropriate intervention level.
What is clinically appropriate remains uncertain. In this study we opted for a greater than 15% level of WHO-FRAX major risk of fracture 18 and/or a >3% risk of hip fracture 19 to identify patients at sufficiently high risk to justify further investigation. These levels are those adopted by the Greater Glasgow and Clyde Osteoporosis Service. Assessment of patients at risk requires measurement of BMD, a risk factor which can be modified by drug therapy.41,42 BMD is routinely used as an essential prerequisite for identifying patients who might benefit from antiosteoporosis drug treatment.43,44 Our local policy is not to start treatment on the basis of risk alone, but to refer patients who have ‘high-risk’ WHO-FRAX scores for BMD assessment. This allows assessment of ‘modifiable risk,’ i.e. that part of the risk profile that can be altered by bisphosphonate therapy.
Some groups advocate starting anti-osteoporosis treatment in individuals presenting after fracture without further BMD assessment.45,46 In this present study, patients presenting with fracture accounted for a total of 19% of the population assessed. It is clear, however, that those who present after a low trauma fracture can be considered at ‘high risk’ for a further event over a 10-year period. This is especially true in those under the age of 60 years at the time of their index fracture. Furthermore, even those individuals who are shown to be at high risk of a further fracture using WHO-FRAX may not have low BMD. In this situation, it may not be possible to modify their high-risk status by bisphosphonate therapy.
Currently the WHO-FRAX algorithm can only be applied on the website one patient at a time. It is easy to see that if the algorithm was applied ‘en-mass’ to data held in primary care, it would allow rapid screening and identification of individuals who might require further bone health assessment. The use of the WHO-FRAX calculator as we have described, may not be an entirely accurate use of the tool and may underestimate fracture risk. We appear to have identified a cohort figure similar to the expected prevalence for osteoporosis. Fracture risk and osteoporosis are not necessarily the same entities but there will be considerable overlap between the two groups.
WHO-FRAX's use has been considered in primary care, 47 but not yet been applied as a screening tool for fracture risk. However, we have demonstrated that existing data held in primary care can be used to screen rapidly and easily. In well recording practices the application of WHO-FRAX, despite some limitations, can help to identify patients at greatest risk. In this way the missing cohort of those at risk of fracture may be more readily identified and searched for on a regular basis, thereby reducing future fracture related morbidity, mortality and costs.
Footnotes
Acknowledgements
We thank Prof DH Lawson for stimulating the project and reviewing the manuscript. We also thank Dr D Skelton (School of Health, Glasgow Caledonian University) and Dr PR MacLean for their advice on the manuscript.