
Abstract
A 41-year-old, obese, patient was admitted to Accident and Emergency with a history of leg cellulitis. A central line was inserted. Documented aspiration of blood from all lines, central venous pressure trace obtained and correct position noted on the chest X-ray (CXR). The patient became increasingly septic despite antibiotic therapy. He was subsequently commenced on a noradrenaline infusion; however, the blood pressure was unresponsive. On admission to the intensive care unit (ICU), it was noted he had an area of white skin over the right clavicle. The infusions were stopped and a CXR confirmed proximal migration of the line. The central line was re-sited and his noradrenaline recommenced with an improvement in his blood pressure. Acute renal failure developed which required haemofiltration for 24 hours. The condition improved and the patient was discharged from ICU. It took several weeks for his renal function to return to normal, but he was discharged home with no permanent damage.
Case report
A 41-year-old morbidly obese patient was admitted to Accident and Emergency (A&E) following a three-day history of right leg cellulitis. The patient was septic and therefore managed according to the principles of early goal-directed therapy. A central line was inserted into the right internal jugular vein by A&E staff under ultrasound guidance. A postprocedural chest X-ray (CXR) confirmed satisfactory placement; however, the tip of the line was fairly proximal in the superior vena cava (Figure 1). Clinical records indicated that it was possible to aspirate blood from all the lumina. A central venous pressure (CVP) trace was obtained from the distal port. The line had been sutured in at 13 cm to skin. He was commenced on broad spectrum antibiotics following blood cultures through the central line and intravenous pressure fluids were administered through a peripheral cannula. He initially responded to fluid therapy with an increase in blood pressure. Following stabilization, he was transferred to the Medical High Dependency Unit. Over the following two days the patient's clinical condition deteriorated, his cardiovascular system became unresponsive to fluid therapy, and he was subsequently commenced on a noradrenaline infusion. This was administered via the proximal port of the CVP line. The blood cultures indicated appropriate antibiotic therapy. Despite this he continued to show signs of worsening sepsis. His inflammatory markers continued to rise and over the next 24 hours his noradrenaline requirements were steadily increasing with minimal impact on his persistent hypotension. He remained in single organ failure at this point; however, his urine output was gradually deteriorating.
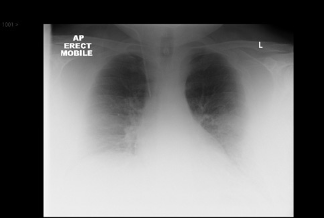
CRX following first central line insertion
He was referred for an intensive care assessment. It was noted that he was hypotensive, with a systolic pressure of no greater than 90 mmHg, despite a noradrenaline infusion at 3.6 mg/hour. He developed oliguric renal failure requiring continuous veno-venous haemofiltration (CVVH). He was admitted to the intensive care unit (ICU) and upon transferring him to the ICU bed he was noted to have an area of white skin over his right clavicle which was non-blanching. All infusions were stopped and only the distal line was noted to be aspirating any blood. An urgent CXR was suggested while a new CVP was set up. This CXR (Figure 2) showed a proximal migration of the central line with some mediastinal widening. A new central line was inserted into the right internal jugular vein (IJV) and a CVVH line was inserted to the left IJV. The CXR showed lines to be in adequate positions and the noradrenaline infusion was recommenced at 0.6 mg/h with good effect. Renal replacement therapy was required for 24 hours prior to the commencement of a spontaneous diuresis. He was discharged several weeks later from the ward as he had persistent renal impairment which took time to recover.
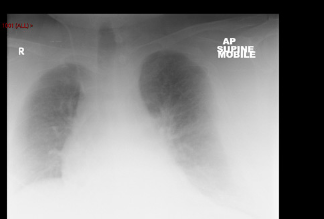
CRX indication the proximal migration and mediastinal Widening
Discussion
Central venous cannulation has become a standard procedure since its introduction to medical practice in the 1950s. Most patients within the ICU have had a central venous line inserted, as they provide dependable intravenous access and enable haemodynamic monitoring. Due to the high number of CVP lines inserted, it is inevitable that the complications associated with this procedure are more commonly seen in critical care areas. We therefore have to put measures in place to not only avoid acute complications, but also to monitor these lines for the potential late complications. Central line safety bundles to prevent line infections are well integrated into clinical practice, but little is done to monitor lines for line migration. Although this is not a common complication, the consequences are serious and potentially fatal.
During our training in central line insertion several methods are taught to ensure correct placement:
Aspirate blood from all catheter lumens to confirm intravascular positioning and to avoid tissue extravasation of drugs from the proximal port due to inadequately inserted catheters.1,2 Flush each port following aspiration.
Obtain a postprocedure chest radiograph to confirm catheter course and tip position prior to using it in non-life-threatening situations.
Malposition is thought to occur in up to one-third of catheter insertions but varies according to anatomical site and the definition of malposition. 2 The distal tip of subclavian and jugular catheters should lie in the lower superior vena cava.3,4 Initial insertion depth for most adults should be 16 cm for right-sided and 20 cm for leftsided internal jugular and subclavian vein catheters. 1 Height-based formulas to determine insertion depth exist, but there are no well-controlled studies supporting their use.5,6
The optimal catheter tip position is controversial and controlled prospective studies are lacking. Catheters generally function well with the tip situated in any major vein. However, tip position may be related to delayed complications including cardiac tamponade, central vein perforation and line migration. It is generally thought that the tip should lie at the level of the carina and right tracheobronchial angle.
One of the main causes of line migration is poor fixation of the line. The catheters should be securely sutured to the skin with a 2.0 silk suture to the catheter hub. Our departmental experience of line migration has been due to loosening at the additional clamp anchor at the skin insertion site. For this reason it seems good practice that all lines should be initially inserted to near the hub and fixated. A postprocedure CXR will confirm whether the line needs to be withdrawn.
Another contributing factor in the risk of line migration appears to be obesity. Some evidence has shown that in the obese population there is a higher risk of line migration, citing 7% of all the documented complications following Hickman line insertion. 7 Due to the increasing trend in obesity in our population, the rate of this complication may rise, which would result in a greater morbidity and mortality. Just as central line-related infection is now monitored closely, maybe it is time we put measures in place to prevent rises in line migrations.
Out of the eight ICUs within the west of Scotland, only one unit, which looks after postbariatric surgery patients, takes measures to detect line migration. They monitored the surrounding tissue for signs of extravasation of fluid, ensured all lines could be aspirated before their continued use and if any doubt was identified a doctor was informed.
The two measures that can be taken to monitor for line migration are:
Education of nursing staff in recognition of a line migration;
Use of the proximal line for monitoring the CVP trace.
Within our department it is now policy to use the proximal line for the CVP measurement. This insures that if proximal line migration occurs, the first indication will be a loss of CVP trace. This will prevent extravasation of drugs and fluids and the potential for associated morbidity and mortality. We have also educated the nursing staff on what clinical features would lead to the suspicion of line migration. We feel that implementing these policy changes will have a beneficial impact on patient safety.