
Abstract
A lipoma of the small bowel mesentery is a rare pathological entity. It has been shown to rarely cause obstruction and volvulus of the small bowel. We report a case of a 72-year-old man who presented with lower abdominal pain and slightly raised inflammatory markers. Computerized tomography of the abdomen showed small bowel perforation and oedematous terminal ileum. At laparotomy the cause was found to be a mesenteric lipoma causing small bowel perforation. As far as the authors are aware, this presentation is not described in the English language literature.
Introduction
Lipomas are benign lumps of mature fat cells that can occur anywhere in the body. They are commonly seen on the trunk, arms and legs but are rarely described intraperitoneally. 1 Intraperitoneal lipomas are often asymptomatic but on occasion can cause symptoms secondary to intestinal obstruction. We present a case of a mesenteric lipoma causing small bowel perforation that necessitates laparotomy and small bowel resection. While small bowel obstruction and volvulus have been described in the literature, this particular presentation with small bowel perforation, to the best of our knowledge, has not been described in the English language literature.
Case report
A 72-year-old man was admitted as an emergency to the surgical department with acute onset of severe lower abdominal pain. Initial observations were satisfactory and the patient was afebrile. Blood tests showed a white cell count of 15.7 × 109/L and a C-reactive protein of 12 mg/L. Plain radiology was normal. On examination the patient was tender with guarding in the right and left iliac fossa. Over the course of the next few hours the patient's pain worsened. He became pyrexial and sweaty with decreased conscious level and mottling of his extremities. Arterial blood gas demonstrated a profound metabolic acidosis. An urgent computerized tomography (CT) scan was performed which showed pneumoperitoneum and free fluid. The majority of the free gas and fluid was situated in the right iliac fossa. The terminal ileum showed some mucosal oedema and there appeared to be a desmoplastic reaction in the region of the terminal ileum (Figure 1).
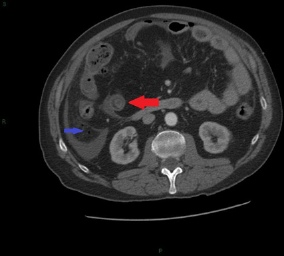
Cross-sectional CT scan of the abdomen demonstrating free gas and fluid adjacent to the distal ileum (blue arrow) with a desmoplastic reaction in the mesenteric fat surrounding the ileum. The distal ileum is seen to be thickened and oedematous (red arrow)
Following resuscitation an emergency laparotomy was performed which showed an inflammatory distal small bowel phlegmon with small bowel perforation. A well-circumscribed area of fullness was noted in the mesentery of the small bowel. A 30 cm small bowel resection was performed and an end ileostomy created.
The pathological specimen showed a portion of small bowel with a definite site of perforation. Surrounding the site of perforation was stranding in the mesenteric fat and a well-circumscribed mass of homogeneous fat (Figure 2). At the site of the mass, the bowel is markedly narrowed and shows evidence of early mucosal ischaemia. Microscopic features of this mass (Figure 3) show mature fat cells lacking atypia, which is in keeping with a mesenteric lipoma, and the mucosal changes relate to mechanical disturbances in the blood vessels around the mass.

This is a cross-section of small bowel demonstrating the well-circumscribed fatty mass in the mesentery. Microscopically this consists of mature adipose tissue lacking atypia. This represents a lipoma of the small bowel mesentery
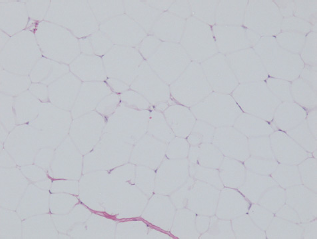
Photomicrograph of the lipoma described. This section demonstrates mature adipose tissue lacking atypia. This is consistent with a lipoma
The patient was initially managed in the intensive care unit before being transferred back to the surgical ward where he made a good recovery and was subsequently discharged.
Discussion
Lipomas occurring in the mesentery are rare with less than 50 cases described in English language literature. 2 The precise incidence of mesenteric lipomas is not known as they are often asymptomatic. There is an increased incidence of lipomata generally in people with diabetes mellitus or hypercholesterolaemia or in those who are obese or have suffered trauma to the area affected.1,3 They either occur in the root of the mesentery or at the luminal edge of the mesentery. These lipomata are soft and mobile masses and do not infiltrate into surrounding structures and as a result allow passage of small bowel content and are usually asymptomatic. 3 If the lipoma becomes large, then it can cause variable symptoms relating to the pressure effects of the lipoma itself, such as vague abdominal pain, distension, anorexia and weight loss.1,3 Rarely, patients present with signs and symptoms of intestinal obstruction and this is usually due to small bowel volvulus caused by the lipoma. 4 Cha et al. 3 reviewed reports of mesenteric lipoma between 1965 and 2007 and did not encounter a case of small bowel perforation caused by mesenteric lipoma. In our case, the patient presented with lower abdominal pain and was found to have a small bowel perforation and peritonitis. This is a rare presentation and to the best of our knowledge the first of its kind in the literature.
A diagnosis of mesenteric lipoma is a difficult one to make and is rarely made prior to laparoscopy or laparotomy. 1 CT is accepted as the imaging modality of choice as it will not only confirm a homogeneous tumour of adipose tissue but will also give information on the effect on the small bowel, whether there is evidence of ischaemia 5 and may demonstrate the typical whirl like pattern of a volvulus.5,6 Interestingly, in our case, CT was reported as showing no soft tissue mass but simply a desmoplastic reaction at the terminal ileum, pneumoperitoneum and free fluid mainly in the right iliac fossa and right paracolic gutter. At operation no evidence of torsion or volvulus was demonstrated, but we can hypothesize that the lipoma caused torsion, small bowel ischaemia and subsequent perforation.
There is no consensus on what the definitive treatment for large or symptomatic mesenteric lipomata should be. Laparotomy and en-bloc resection of the lipoma with the affected small bowel loops is often required. This may also be considered in patients who are asymptomatic with large mesenteric lipomas due to the potential future risk of volvulus or obstruction. 3 Laparoscopy and laparoscopic resection is accepted as being more appropriate for benign tumours in the abdomen due to the reduction in morbidity and better identification of surgical planes under magnified views. 7 However, clearly in certain circumstances – due to size of the lipoma or the extent of small bowel involvement – this is not feasible and an open procedure is required. Liposarcomas have also been described in the literature, rarely arising from the small bowel mesentery. 8 They are the most common sarcoma found in the soft tissue but infrequently arise from a pre-existing lipoma. 9
Conclusion
Mesenteric lipomas are rare and often found incidentally. They should be considered in the differential diagnosis of unusual abdominal pain. They can on occasion cause abdominal symptoms and can even lead to more serious symptoms such as intestinal obstruction, volvulus and, in our case, small bowel perforation. Treatment is either open or laparoscopic surgery with or without excision of the affected small bowel in symptomatic patients and should be considered in asymptomatic patients with large lipomata to prevent future complications.