
Abstract
Subacute puerperal inversion of the uterus is preferably managed by surgery. Conservative management by Aveling's repositor or vaginal packing was cumbersome and took long. However, a long surgery scar over the uterus carries a high risk of uterine rupture in the next pregnancy. A series of four village women with subacute puerperal inversion of the uterus were treated with vaginal packing. A twice-daily rigorous routine of dressing and packing of the uterus was followed, along with supportive treatment. The uterus was raised high in the pelvis so as to stretch the round ligaments, which then slowly pulled out the fundus in about a month. The vaginal packing method may be sincerely attempted in young women from remote areas, as this would reduce the riskof uterine rupture in the next pregnancy.
Introduction
While acute puerperal uterine inversion is a life-threatening emergency which is managed by manual reposition or by the O'sullivan's method, the subacute or chronic inversion is managed surgically. However, surgery increases maternal morbidity, is expensive, requires expertise and compromises the future reproductive health of young mothers, especially those from the less developed areas. We report on four cases where conservative management by vaginal packing was successful.
Case histories
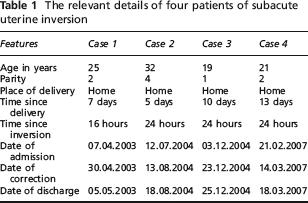
Four rural women had been admitted to the hospital from 2003 to 2007, complaining of something coming out of the vagina some days after delivery. A diagnosis of subacute puerperal inversion of the uterus was established by the inability to feel the cervical rim or to go beyond it. A bimanual examination confirmed the absence of a uterus in the pelvic cavity.
All were severely anaemic and febrile with bloodstained infected discharges. None were in shock (Table 1).
The relevant details of four patients of subacute uterine inversion
The bladder was catheterized using a Foley's catheter. Infection and oedema of the uterus was controlled by cleaning the area twice a day with savlon, hydrogen peroxide and chlorine water. The area was then covered with cotton gauze pads soaked in a 2% glycerine acriflavin lotion. The uterus was bound tightly with a gauze bandage to keep the pads in place and a tight T-bandage was applied. Supportive management with blood transfusions, analgesics and antibiotics was carried out simultaneously. The uterus could be pushed inside the vagina within about a week.
The next stage involved packing the vagina daily with a sufficient amount of cotton gauze pads soaked with glycerine acriflavin lotion, to push the uterus high in the pelvis. This was again followed by a tight T-bandage. Receding of the uterine fundus into the cervix was noted after three to five days. After another 10 to 15 days of packing, the inversion was corrected as confirmed by bimanual examination and ultrasound. The complete correction took 20 to 32 days in all.
Patients were counselled about the 25–40% risk of a recurrence of the condition, the choice of tubal ligation, the necessity to preserve the discharge ticket, the necessity of attending follow-ups when advised and the need for hospital delivery for future births. One patient conceived a year later and delivered at the hospital. Another underwent a laparoscopic tubal ligation four months later. The third and fourth were lost to follow up.
Discussion
The incidence of puerperal inversion of the uterus varies from 1/2000 to 1/23,000 of deliveries. Acute inversion is more common (86%). The term subacute refers to an inversion which occurs 24 hours to 30 days after delivery, while chronic one becomes apparent after 30 days. 1 Manual reposition of subacute or chronic inversion usually fails due to constricted cervix. Surgery is the method of choice but it has to be deferred until the infection and oedema subside.
Furthermore, surgery involves cutting the cervical rim and an extension of incision on the body of the uterus to variable lengths. 2 This not only increases maternal morbidity but produces a long scar which can rupture during pregnancy or labour. It can be a risky procedure for women living in far off villages who have very limited means and a low level of motivation.
The use of Aveling's repositor as a method of conservative management was abandoned because of the discomfort and trauma caused to the patient. Vaginal packing method is also no longer performed. 3 Although Jeffcoate and Kerr agree with the principle of lifting the uterus high in the pelvis, thereby causing the uterine ligaments to stretch and pull out the fundus, they favoured surgery. The disadvantage of the vaginal packing method is the long hospitalization period required, the inconvenience caused to the patient and, often, the surgeon's lack of experience of the procedure. However, conservative management should be tried, especially in young woman from remote areas or with bad obstetric histories. Trials of this method by other clinicians will increase our collective experience.