
Abstract
Neurocysticercosis (NCC) is the most common helminth infection of the central nervous system. It is caused by the larval form of the tapeworm Taenia solium and is increasingly recognized as a major cause of neurologic disease worldwide. Epilepsy is the usual mode of revelation. Neuroimaging, including computed tomography and magnetic resonance imaging, combined with serodiagnostic techniques have led to this increased recognition. We report on two cases (one co-infected with the HIV) of NCC diagnosed in 2006 and 2008 at the Omar Bongo Ondimba Army Teaching Hospital. New-onset epilepsy revealed the two cases. Medical treatment with albendazole, anti-epileptic drugs and corticosteroids led to full recovery. NCC should be considered in tropical countries as a leading cause of epilepsy. Moreover, NCC should be included in the differential diagnosis of neurologic infections in HIV patients in endemic populations.
Introduction
Neurocysticercosis (NCC) is a cosmopolitan infection increasingly recognized as a major cause of epilepsy worldwide. 1 The key to this increased recognition is the development and application of non-invasive computerized neuroimaging, including computed tomography and magnetic resonance imaging, combined with immunologic tests to confirm the diagnosis. 2 We report on two cases (one co-infected with HIV) of NCC diagnosed in Libreville, Gabon.
Case history
Case 1
A 30-year-old Gabonese man presented with a first presentation of generalized tonic-clonic seizures. History of the disease suggested a two-week fever with headache and altered consciousness. Electroencephalography recorded epileptic seizures controlled with diazepam combined with phenobarbital. The ophthalmologic examination and an examination of the cerebral fluid were normal. Screening for HIV and the serologic tests for syphilis and cryptococcal antigen were negative. A computed tomography of the head showed disseminate nodules with perilesional oedema (Figure 1). An electroimmunotransfer blot (ETIB) detected specific antigen of Taenia solium. The long-term treatment combined albendazole (15 mg/kg/day) with phenobarbital (200 mg/day). Corticosteroid was used at 1 mg/kg/day for five days. Five months later, a relapse was indicated by computed tomography abnormalities showing an increase of the lesions with dense calcifications. A second-line therapy of praziquantel (50 mg/kg, third a day) for 15 days and corticosteroids 1 mg/kg/day for five days was conducted. At the one-year follow-up, computed tomography showed a decrease in the lesions (Figure 2) and the cysticercosis serology was negative.
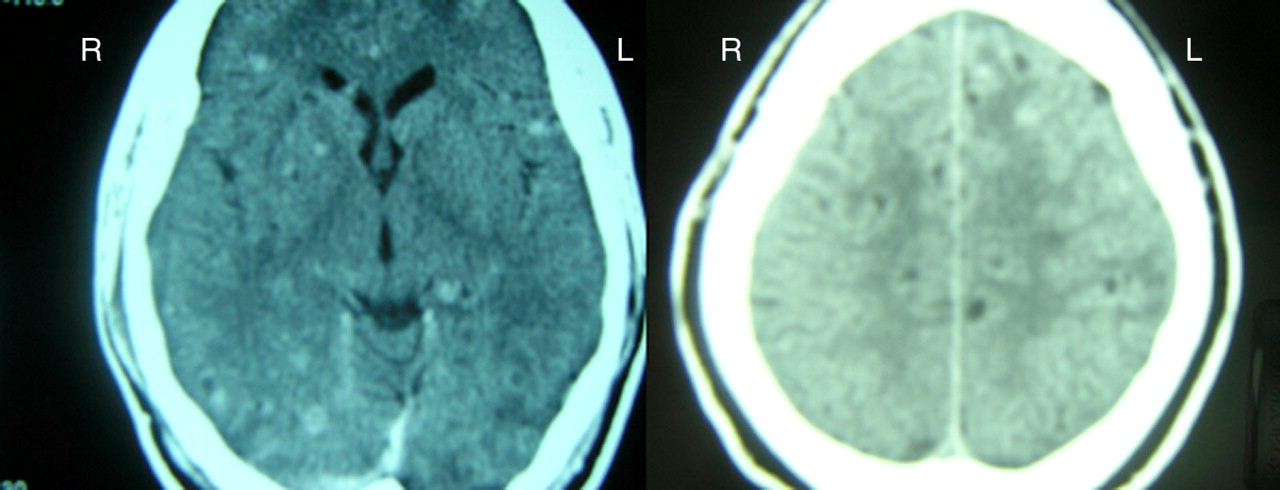
Computed tomography of the head shows multiple cysts with calcifications
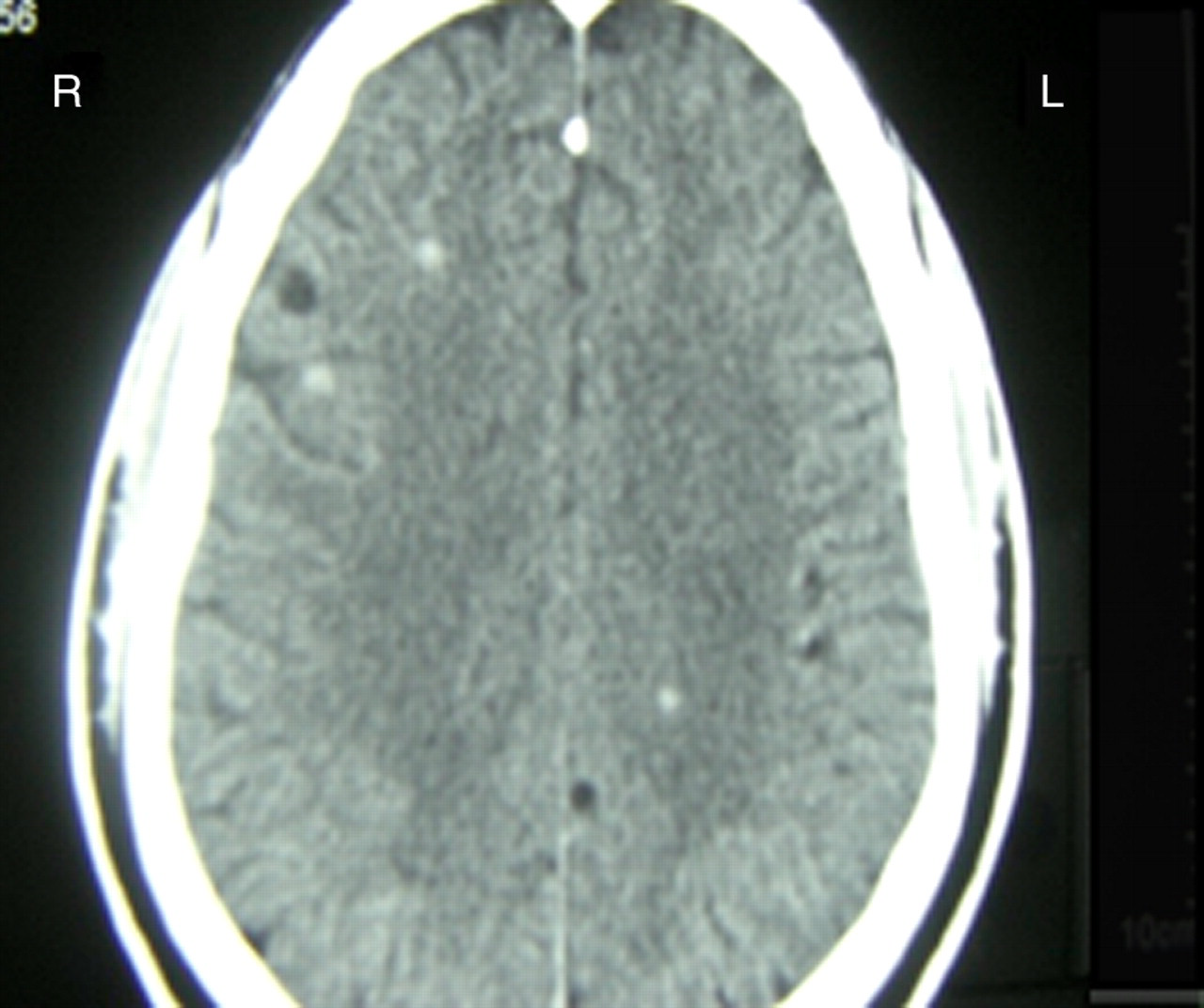
One year after treatment
Case 2
A 27-year-old Gabonese woman presented to the hospital in May 2008 with new onset generalized tonic-clonic seizures. She also complained of headaches, fever (rectal temperature at 38.5°C), oral candidosis, hairy leukoplakia and disseminated papular prurigo. Early treatment with adequate doses of diazepam followed by treatment with phenobarbital controlled the seizures. HIV screening was positive with a CD4 count of 10/mm3. A chest X-ray and serologic tests for syphilis, cryptococcal antigen and toxoplasma IgG were negative.
Baseline computed tomography of the head with contrast revealed multiple calcifications with surrounding oedema located in the two hemispheres (Figure 3). No evidence of hydrocephalus or cerebral hypertension was observed. Magnetic resonance imaging of the brain was not performed. A lumbar puncture with intracranial pressure assessment and cerebral spinal fluid examination was unremarkable. An ETIB detected specific antigen of T. solium.
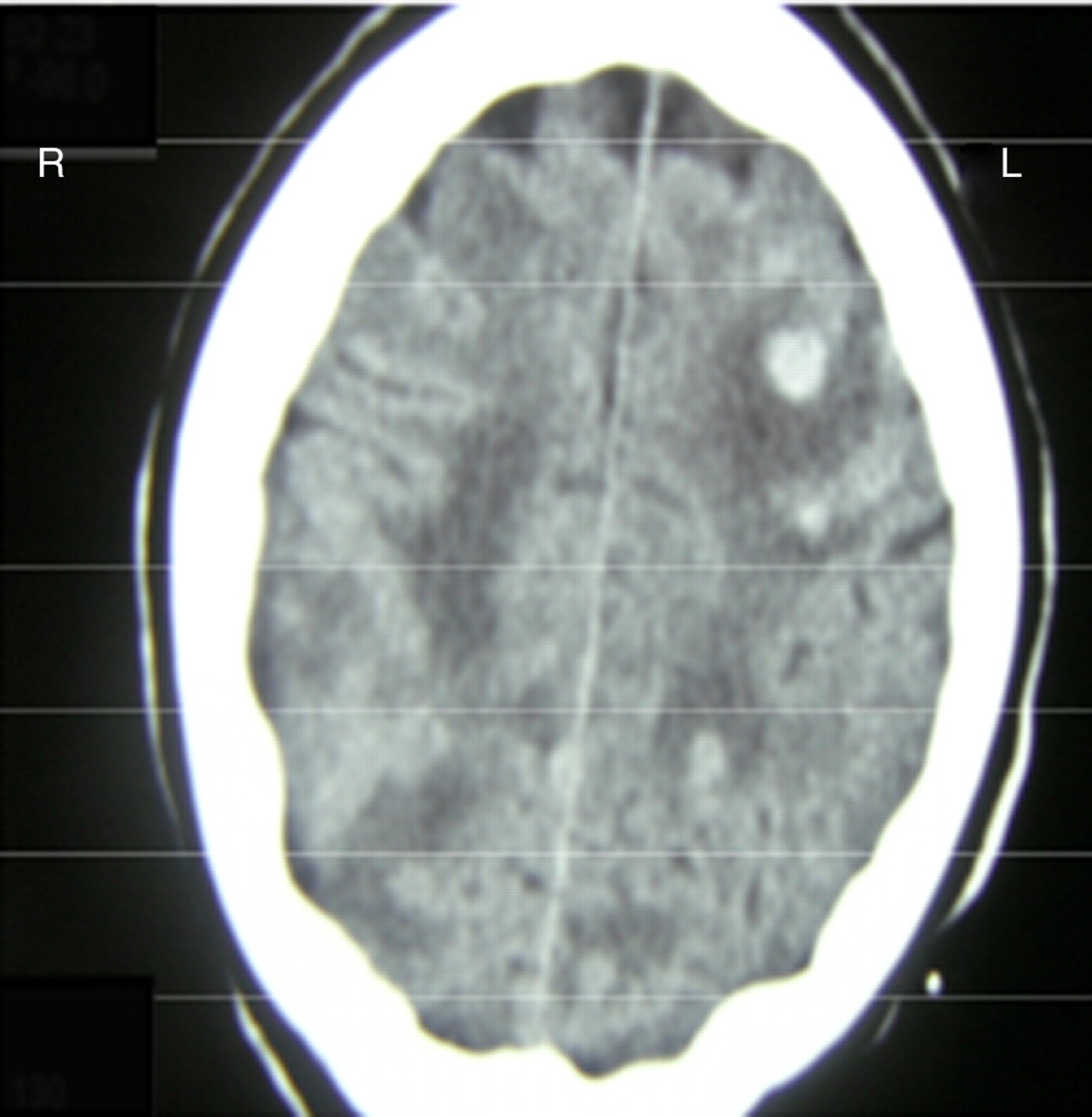
Computed tomography shows hyperdense scolices in the brain parenchyma (left fontal lobe++) surrounded by perilesional oedema
Long-term treatment with albendazole (15 mg/kg/day) combined with phenobarbital (200 mg/day) lead to total recovery. She was given 1 mg/kg/day corticosteroid for five days. A computed tomography of the head was performed five months later and showed that the lesions had disappeared. The patient was lost to follow-up.
Discussion
NCC, caused by the larval form of the tapeworm T. solium, is the most common parasitic disease of the central nervous system and the most common cause of acquired epilepsy worldwide. Improved serodiagnostic, neuroimaging and treatment have led to more accurate diagnoses and improved prognosis for patients.
The host inflammatory response is now recognized as a key element in the pathogenesis of the disease. We report on two cases of NCC diagnosed in 2006 and 2008 in the internal medicine ward of the Omar Bongo Ondimba Army Teaching Hospital, Libreville, Gabon, where data concerning this disease are lacking.
NCC is a growing problem in tropical countries where pigs are raised and it is increasingly recognized as a leading cause of epilepsy. In studies mainly conducted in Latin America, NCC has been shown to be present in 9–18% of randomly selected people in endemic areas and 80% or more selected patients with seizures. 3
Symptoms of NCC typically develop after a prolonged latent period. In NCC, there is normally a chronic immune response with multiple cell types that secrete Th1 and Th2 cytokines (inflammatory and anti-inflammatory cytokines). Viable parasites seem to induce Th2 response. In contrast, the death of the cysticerci is associated predominantly with Th1 cytokines. This phenomenon could worsen the clinical condition during the first days of treatment. Seizures in NCC are thought to result from the inflammatory response to the release of parasite antigens at the time of the parasite's death and this response may be mediated by host molecules, including substance P.
Symptomatic therapy is very important in NCC. In fact, the key determinants of seizure recurrence in patients with NCC are the optimal doses of antiepileptic drugs such as phenobarbital used to treat our patients. 4 Increased intracranial pressure, not found in our two cases, must be addressed rapidly, usually by a neurochirurgical approach. Using antiparasitic treatment, only 30–50% of lesions are resolved by six months and antiparasitic drugs and steroids do not affect the formation of calcifications or the risk of chronic epilepsy. 5
One of our two patients had HIV infection with severe immunodeficiency (CD4+ = 10/mm3). In a recent review, NCC-HIV co-infected patients were more frequently associated with multiple parenchymental lesions and other opportunistic infections of the central nervous system such as tuberculosis and toxoplasmosis. The response rate to cysticidal therapy in HIV patients is similar to non-HIV patients. NCC is sometimes associated with immune reconstitution inflammatory syndrome (IRIS) after starting highly active anti-retroviral therapy (HAART) and the case fatality rate (12%) is higher in patients with HIV than in non-HIV patients. 6 NCC should be included in the differential diagnosis of neurologic infections in HIV patients in endemic populations. Given the growing problem of HIV-infection in Gabon, more research on how to treat co-infected patients is needed.
Conclusion
In tropical areas, like Gabon, NCC should be considered as a cause of epileptic seizures. Moreover, in HIV-positive patients, NCC should be included as an alternative diagnosis of central nervous system infections. Performing an HIV test in new onset NCC should be discussed in areas where HIV is endemic.