
Abstract
We assessed the involvement of vitamin A deficiency (VAD) and anaemia as co-morbidities associated with severe forms of protein-energy malnutrition in hospitalized children. In a descriptive case series study of 57 children, one clinical case of xerophthalmia was diagnosed: 44.0% had levels of serum retinol <20 µg/dL and 88.0% had Hb <11 g/dL, of whom 30.0% had haemoglobin levels below 7.0 g/dL.
Introduction
Protein-energy malnutrition (PEM) in childhood still constitutes a serious problem worldwide 1 due to the magnitude, biological consequences and social damage it can cause. 2
The most common micronutrient deficiencies in the world are vitamin A deficiency (VAD), anaemia and PEM, which frequently occur together, 2 with their common epidemic factors and aetiopathogenic interactive processes. As such, any preventive or healing approach should take into account the interdependence of these three deficiency conditions.
From this perspective, we evaluated the co-existence of VAD and anaemia in children with severe PEM in a large hospital in the state of Pernambuco which was linked with the Ministry of Health Department as a regional referential centre in north-eastern Brazil.
Materials and methods
We carried out a descriptive case series study of 57 children under 60 months of age who were hospitalized at the Instituto de Medicina Integral Prof Fernando Figueira (IMIP), with severe forms of PEM (weight-for-height lower than −3 scores Z), 3 and/or the presence of bilateral feet oedema, during the period August 2004 to May 2005.
The cases included hospitalized children who had participated in a validated adaptation experience according to the World Health Organisation (WHO) protocol for the treatment of severe malnutrition, 4–6 excluding those who had received, on hospital admission, a standard mega dose of vitamin A (100,000 or 200,000 UI).
The weights of the children under two years of age were evaluated on a 5 g accurate scale and their heights were checked using an accurate horizontal anthropometric of 0.1 cm. For children over two years, weight was assessed on an electronic platform 5 g accurate scale by weighing in the mother's arms and then obtaining the weight of the mother in order to determine the difference. Their heights were checked using an anthropometry attached to the scale with a 2 m extension and 0.1 cm precision.
For biochemical proofs, blood samples of approximately 3.5 mL were collected by cubital phlebotomy. Serum retinol concentrations were analysed by high performance liquid chromatography and those under 20 µg/dL were considered to be deficient. 7 Haemoglobin values were obtained using sodium lauryl substrate (SLS) haemoglobin and reagents (sulfolyser and cell clean).
It was considered to be a basal disease and the pathological situation that caused negative and decisive influence in the child's nutritional state, previously diagnosed at admission or during hospitalization. The patients who introduced one of the basal diseases, or other morbid conditions of equivalent pathogenic importance, were considered to be secondary malnutrition cases.
The study was approved by the Ethics Committee in Human Beings Research at IMIP.
Results
A total of 57 children were initially selected for the study but seven (12.3%) were excluded.
The children's ages varied from one to 57 months, with a mean age of eight months (1st quartile = 4 months and 3rd quartile = 17 months). The sociodemographic variables, the feeding history and the occurrence of basal disease are described in Table 1.
Sample of children aged less than 60 months with severe malnutrition hospitalized at Instituto de Medicina Integral Prof Fernando Figueira (August 2004 until May 2005) and their characteristics
*MAR = metropolitan area of Recife
†Minimum wage according to May 2005 = R$ 150,00 (corresponding to US $60.68)
‡Refers to secondary malnutrition
There were nine (18.0%) deaths: three presented with oedema and four presented with the signs and symptoms of septicaemia. Five of the nine deaths did not present with a base disease.
One child presented with a suspicion of xerophthalmia: the child was 48 months old. She had been breastfed until two years of age and had received vitamin A supplements eight months before admission. She was hospitalized with diarrhoea, presenting concentrations of haemoglobin of 9.1 g/dL and serum retinol of 16.5 µg/dL. An ophthalmologic examination with a rift lamp diagnosed bilateral xerosis and cornea ulcer. The child also presented with a hypothetical diagnosis of ectodermal dysplasia.
In 22 cases (44%), the children presented with low levels of serum retinol (<20 µg/dL), compatible with VAD situations. The serum retinol concentrations in the children with severe PEM varied between 11.5 µg/dL and 52.1 µg/dL, with a mean of 21.7 µg/dL (1st quartile = 16.2 µg/dL and 3rd quartile = 28.4 µg/dL).
The haemoglobin concentrations varied from 3.4 g/dL to 15.5 g/dL, with a mean of 8.5 g/dL (1st quartile = 7.3 g/dL and 3rd quartile = 9.3 g/dL). Haemoglobin levels lower than 11 g/dL occurred in 44 cases (88.0%), of whom 30% had levels of less than 7 g/dL (Figure 1).
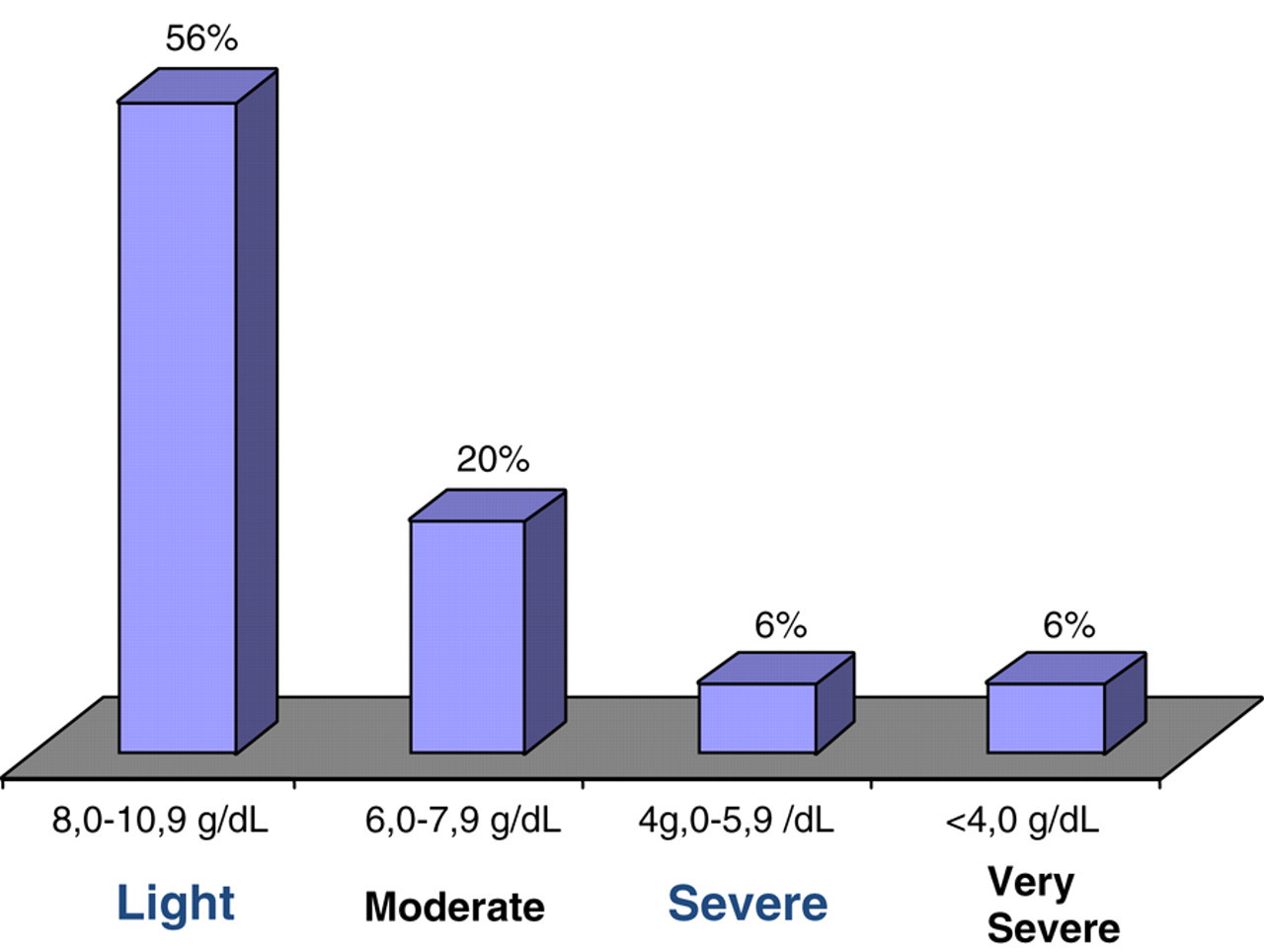
Distribution of anaemia cases according to haemoglobin levels4 in children with severe forms of PEM, hospitalized at Instituto de Medicina Integral Prof Fernando Figueira (August 2004 until May 2005)
Discussion
The implementation of the WHO protocol for the treatment of severe malnourished children at IMIP had great clinical relevance. 5,6,8 The actions and care proposed in a referred protocol consisted of treatment for diseases that habitually represent co-morbidities implicated with severe levels of malnutrition. The results exposed here offer some interesting results. There were no serum retinol concentrations below 10 µg/dL, an indication of hepatic vitamin A depletion. However, the detection of 44% of cases under 20 µg/dL reflects a considerable risk situation, as the largest tolerable occurrence in a population for this level would be 10%. 7
The only registration of severe xerophthalmia highlights a fundamental importance, as the occurrence of one corneal lesion case in 10,000 observations, in a random sample of the population, would have been indicative of an important problem in collective health regarding VAD. 7
It was also observed that 40% of the children presented with bilateral feet oedema, particularizing a severe manifestation which is similar to the results of another study with the same objectives, developed in Colombia 9 , in which this oedematous form of malnutrition was shown to be an important death risk factor.
The association of anaemia with cases of severe malnutrition was even more notable, since 88.0% of the children were anaemic. In this series, that two children were hospitalized due to the severe anaemia and that often haemoglobin levels under 4 g/dL could demand, in the context of each clinical case, an emergency blood transfusion due to the risks for severely malnourished patients.
A fundamental bibliographic evaluation of the conjugated risk of severe malnutrition, VAD and anaemia in hospitalized children is currently unavailable. However, if the combined effects of the three-deficiency problem on hospital mortality still cannot be safely explained, the potential risks could and should be properly considered to be essential to the success of the treatment.