
Abstract
With an estimated 5.7 million people living with HIV/AIDS, India has the highest HIV/AIDS prevalence in the world, according to UNAIDS. Due to similar routes of transmission, co-infection of HIV with hepatitis B and hepatitis C viruses is a common event with significant clinical implications. The present study was undertaken to highlight the profile of patients of HIV with HBV/HCV co-infection, as literature from India on this topic is sparse. Out of 1953 patients suffering from HIV registered at our centre during the study period, 80 patients were co-infected with HBV/HCV. HBV co-infection was detected in 2.61% of patients and HCV co-infection in 1.69% of subjects. Our study demonstrates low HIV /HCV/HBV co-infection rates in Delhi as compared to most other studies from India, which is partly attributable to low incidence of intravenous drug use and infrequent transfusion-related infections in our study group.
Introduction
Chronic viral infections are a global health burden. At the end of 2005 1 there were 38.6 million people with HIV, 400 million with hepatitis B virus (HBV) and 170 million with hepatitis C virus (HCV) infections worldwide. 2,3 Due to their similar routes of transmission, co-infection with these viruses is a common event. Among HIV-infected patients, 2–4 million are estimated to have chronic HBV co-infection and 4–5 million are co-infected with HCV. 2
With an estimated 5.7 million people living with HIV/AIDS, according to UNAIDS 1 India has the highest HIV/AIDS prevalence in the world. The epidemiology of hepatitis C in India has not been studied systematically and the prevalence of 0.29–1.85% has largely been estimated from studies conducted in blood banks. 4 The average carrier rate of hepatitis B in the general population of the Indian subcontinent is around 4%. 5,6
There are significant clinical implications for patients with HIV and HBV/HCV co-infection. With the institution of highly active antiretroviral therapy (HAART) for HIV, the mortality resulting from opportunistic infections and malignancies has reduced substantially with progressive liver disease now being the most common cause of death among patients infected with HIV. 5 There is more likelihood of hepatotoxicity associated with the antiretroviral agents in patients co-infected with HBV/HCV leading to significant diagnostic confusion. 7
The present study was undertaken to highlight the profile of patients of HIV with HBV/HCV co-infection as literature from India on this topic is sparse.
Material and methods
The study cohort consisted of all adult patients (>15 years of age) registered at the antiretroviral treatment (ART) centre of the GTB Hospital from December 2005 to June 2009 after being tested positive for HIV following pre-test counselling and informed consent. The patients were screened for hepatitis B surface antigen (HBsAg) and antibody to hepatitis C virus (anti-HCV) using ELISA kits as part of their pre-ART work up.
Descriptive statistics are presented with median (and range) or proportions, for continuous or categorical variables, respectively. The statistical package for social sciences (SPSS, Version 13.0) software was used for the analysis of the data. A P value <0.05 was considered statistically significant.
Results
A total of 1953 patients aged >15 years registered at the ARTC-GTBH from December 2005 to June 2009. Eighty patients were co-infected with HBV/HCV; HBV co-infection was detected in 2.61% and HCV co-infection in 1.69% subjects (Table 1). Four tested positive for both HBsAg and anti-HCV antibodies. The majority were male (72.5%) and the median age of the subjects was 32 years. Most of the co-infected patients were from the 25–34 years age group (36.25%) followed by the 35–44 years age group (32.5%). Overall, 55.95% were heterosexual, 22.62% were intravenous drug users (IDUs), 7.14% were blood transfusion recipients, 8.33% were homosexual and 5.95% had an unknown source of infection. Among the HIV/HBV co-infected patients the predominant mode of transmission observed was heterosexual (70.58%) in contrast to HIV/HCV co-infected patients where the predominant mode of transmission observed was IDU (45.45%; Figure 1). At the time of registration, the majority of patients 47.5% were in the World Health Organization clinical stage II.
Mode of transmission of infection in HIV and hepatitis co-infected patients. BT, blood transfusion; MSM, men who have sex with men. Baseline characteristics of HIV and hepatitis co-infected patients TG, transgender; IDU, intravenous drug user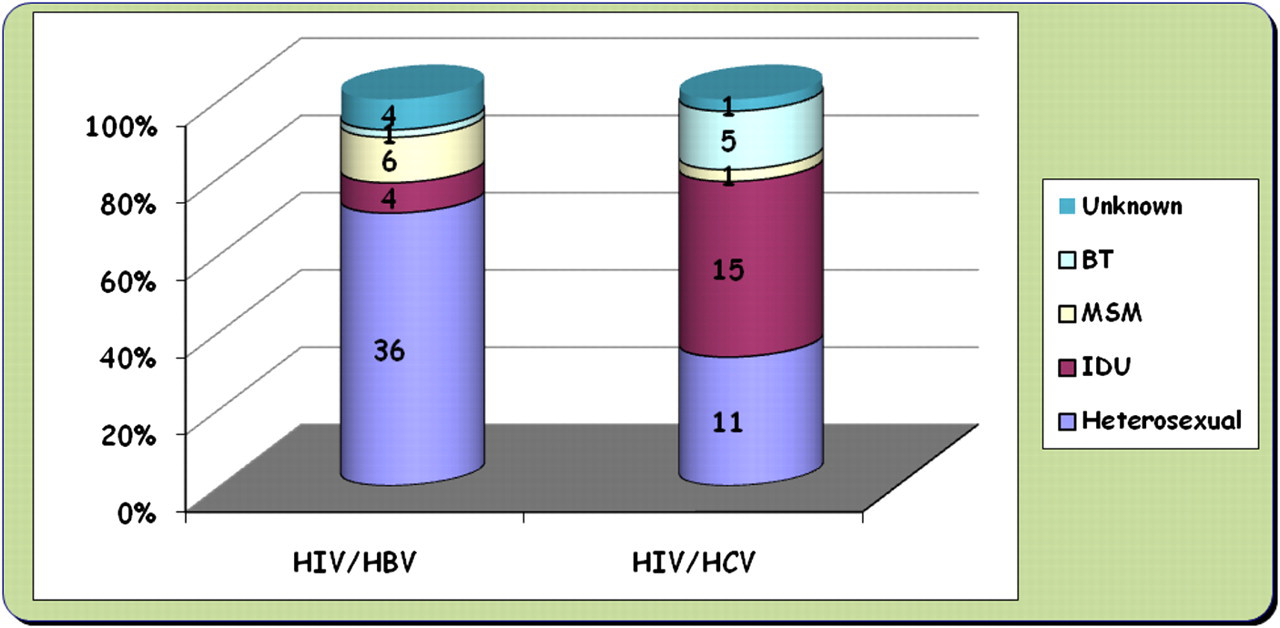
Discussion
Our results indicate that HIV-infected men and women are at risk of viral co-infections, as illustrated by the prevalence of HBsAg (2.61%) and HCV (1.69%) antibodies. HBsAg and HCV antibody prevalence is similar to studies from North India. 8 HCV prevalence in our study group is lower than observed in studies from South and North India. 9,10 Studies showing higher prevalence have a larger number of IDUs and relatively more transfusion transmitted infections. Another factor responsible for the low prevalence is that we were unable to perform HBV-DNA or HCV-RNA polymerase chain reaction in our patients. Similar to studies by Saravanan et al. 9 from South India and Tripathi et al. 8 from North India, our study group also predominantly comprised of heterosexually acquired HIV infections. The higher percentage of IDUs (22.62%) in our study is in contrast to lower percentages (5.35% and 4.1%) seen in studies by Saravanan et al. 9 and Tripathi et al., 8 respectively and probably accounts for the relatively higher number of hepatitis C and HIV co-infected patients (39.3%) in our study. Intravenous drug use was predominantly responsible for the HIV/HCV co-infection in our study as against the heterosexual mode in the studies by Saravanan et al. 9 and Tripathi et al. 8 This probably indicates that the problem of IDUs is considerably greater in metropolitan cities like Delhi due to the easy availability of drugs, social stress and influence. Similar to the above studies, the incidence of blood transfusion related infections is very low. The maximum levels (36.25%) of co-infection for HBV/HIV and HCV/HIV occurred in the 25–34 group, which is the age group where HIV positivity is reportedly higher according to the Indian literature. 8–10 The percentage of males was significantly higher (72.5% versus 20%) than females (P < 0.05) which concords with previous reports from other parts of the country. 8,10 The sex distribution is also marked by the presence of six transgenders. The HIV/HBV co-infected patients had lower CD4 counts compared to HIV/HCV co-infected patients, albeit statistically insignificant, which could be due to the smaller number of cases, wide range of CD4 counts and the subjects being at different stages of the HIV disease.
Our study has certain limitations. As it was largely a cross-sectional study, a causal relationship between the time of exposure and infection could not be established. There was no HIV negative control group and ELISA for HBeAg, PCR for HBV DNA and RT-PCR for HCV RNA could not be performed due to cost constraints. The study cohort comprised of patients attending a tertiary care hospital and may not, therefore, be representative of those seen in a community setting.
Conclusion
Our study demonstrates low HIV/HCV/HBV co-infection rates in Delhi compared to other studies from India which may partly be attributable to the low incidence of IV drug use and infrequent transfusion-related infections in our study group, and partly to some false-negative cases which could have been identified if HBV-DNA and HCV-RNA were estimated.