
Abstract
Midline laparotomy is an emergency surgical operation frequently performed in cases of intra-abdominal pathology. Closure of the incision is usually done by continuous suturing by mass closure. In an emergency operation the intra-abdominal milieu is usually contaminated leading to gut oedema and, hence, an increase in postoperative intra-abdominal pressure. It is complicated by wound dehiscence, burst abdomen, etc. The cause of this complication is an increase in horizontal tensile forces on the site of the insertion of sutures which cuts the sheath. In this technique of reinforced tension line suture peak tensile forces are distributed from the suture base to the surrounding tissue through a horizontal suture, thereby preventing the suture from cutting through the tissue. From July 2007 to June 2009 patients requiring laparotomy were randomly divided into test and control groups by a ‘closed envelope’ technique. Their postoperative intra-abdominal pressure was recorded by urinary bladder catheter manometry. The result of this technique was compared with the incidence of burst abdomen in cases where it was closed by continuous suture. A total of 190 patients underwent laparotomy. In 90 the abdomen was closed by reinforced tension line (RTL) and in 100 patients by continuous suturing. None of the RTL group had a burst abdomen. Thirteen who had closure by continuous suture had a burst abdomen. The analysis of the results was done using the chi-square test. On comparing the incidence of burst abdomen in cases operated by continuous suture technique and by RTL, the P value was found to be 0.0026 which is highly significant. On analysis of the incidence of burst abdomen in cases having a grade II intra-abdominal pressure the P value was found to be 0.0009 which is highly significant. Closure of midline incision by RTL reduces the incidence of burst abdomen. Registration No. PROVCTRI/2008/091/000269 (
Introduction
Midline laparotomy is one of the most frequently performed operations in surgical emergencies such as perforations, obstruction and trauma. In these cases, either the contaminated abdomen or a long-standing obstruction leads to gut oedema during the preoperative and postoperative periods. This causes increased intra-abdominal pressure that frequently leads to various complications such as wound dehiscence and a burst abdomen.
Although various techniques have been described for the closure of the abdomen, the incidence of these complications is very high. Horizontal tangential pressure on the suture, which cuts the tissue, leads to a burst abdomen. This horizontal force on the suture is much greater than the vertical forces when the midline laparotomy is closed by a continuous suture, thereby leading to excessive pressure at the site of suture insertion. This pressure is distributed parallel to the fascial margin, with the peak pressure at the site of suture insertion that further tears the tissue (Figure 1).
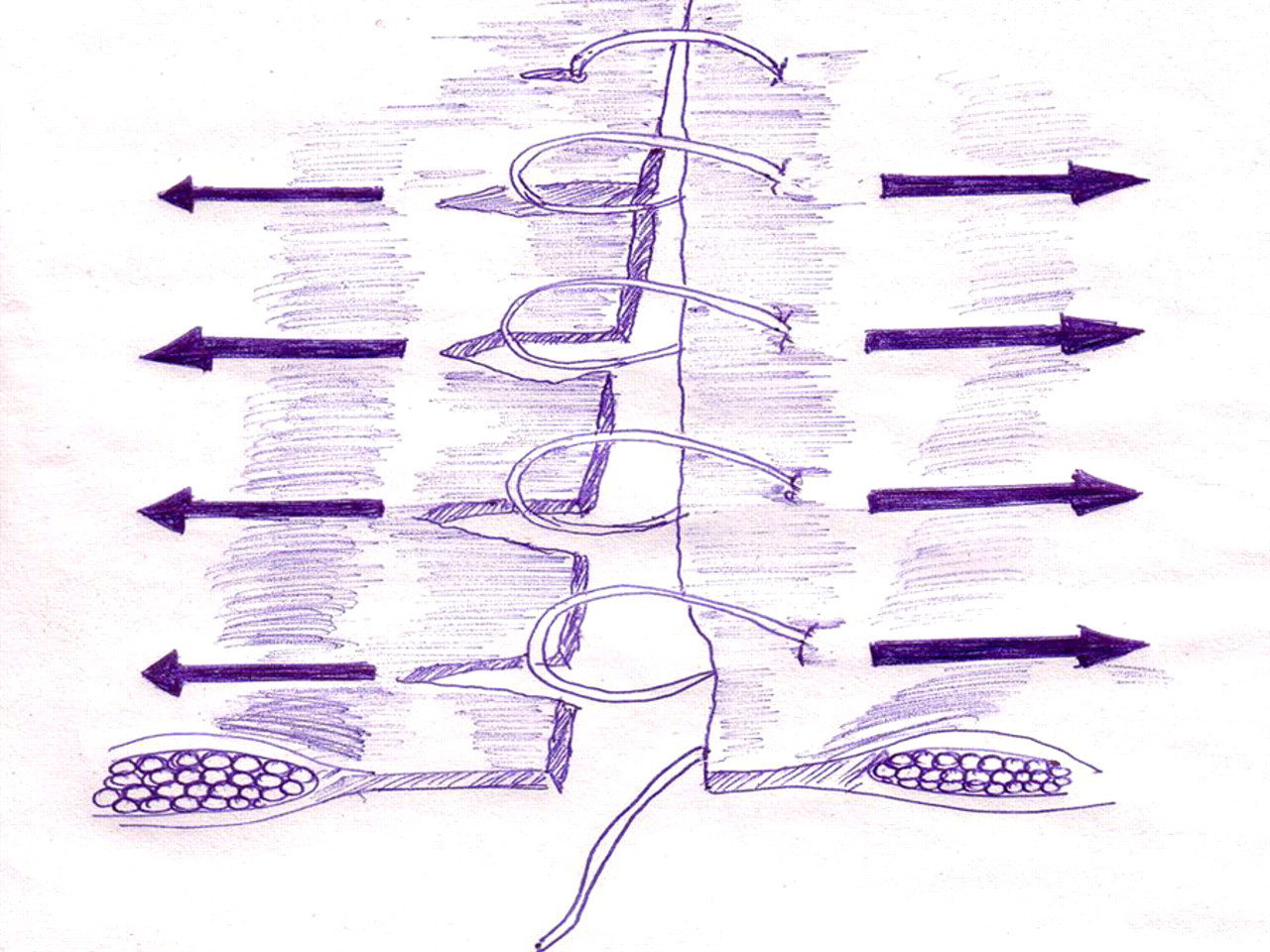
Tearing of the tissue at the site of suture insertion
We have developed an abdomen closure technique in which we connect the peak pressure points so that this peak pressure is uniformly distributed along the entire tissue and not only exerted at the site of suture insertion. This technique reduces the incidence of tissue tear.
The aim of this study was to evaluate the feasibility of the reinforced tension line (RTL) suture in midline abdominal closure and to compare it with the conventional continuous suture method in terms of postoperative abdominal pressure and the development of a burst abdomen.
Methods
The study was carried out in our emergency department on patients undergoing a midline laparotomy for various conditions (peptic perforation, volvulus, colonic perforation, obstruction-induced rupture of liver abscess, appendicular perforation and traumatic intestinal perforation).
From July 2007 to June 2009, patients requiring laparotomy were randomized into test and control groups by a sealed envelope technique. The study is a double-blinded prospective study.
Our surgical technique is as follows: the rectus sheath is cleared about 1.5 cm laterally linea alba. The longitudinal suture (polydioxanone) is inserted using a 65-mm 1/2 needle parallel to the linea alba, starting at the lower end of the incision, as a continuous suture on both sides, after first clearing the fat about 2 cm from it (Figures 2 and 3). The ends are held by haemostats inferiorly. Then the continuous suture (again polydioxanone) is placed using again a 65-mm 1/2 needle, taking care that the points are introduced laterally to the longitudinal suture. This suture is tied and knotted. The longitudinal suture is then made taut and tied, taking care not to pull it excessively as the function of this suture is to distribute the pressure on the tissue, akin to the concept used in the construction of tall buildings where the pressure is distributed by using pressure beams within reinforced concrete. Too much tightening will lead to bow stringing. Care is taken that no bowel loops are caught within either suture.
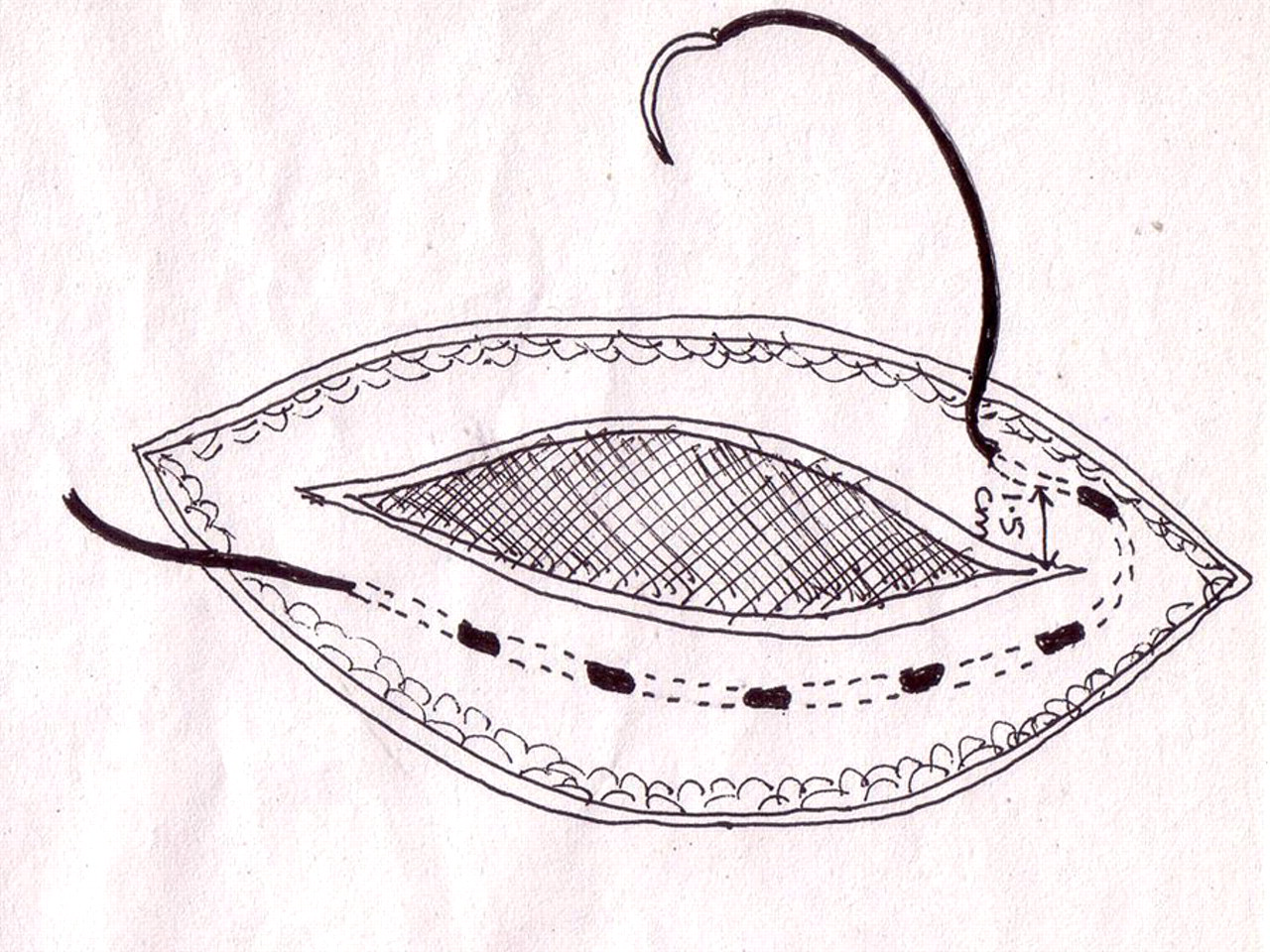
Technique of inserting reinforced tension line
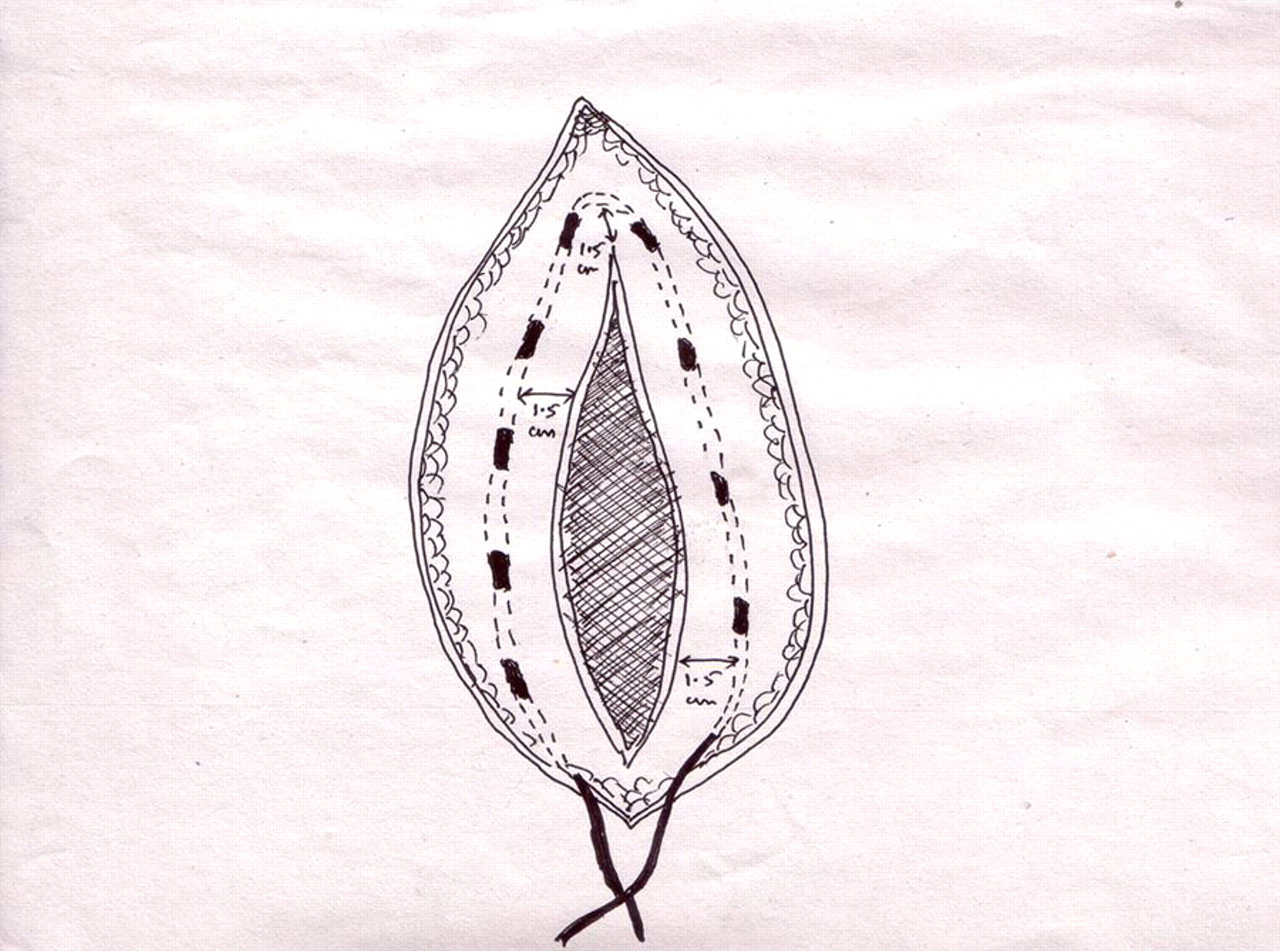
Reinforced tension line completed

Completed reinforced tension line and increased points of dispersion of the peak force
Finally, the subcutaneous sutures and skin sutures are used to close the wound. A simple suture loop polydioxanone (PDS) was used as suture material and a 65-mm 1/2 needle was used in all patients who underwent abdominal closure by simple closure.
All patients were administered a second-generation cephalosporin, metronidazole and aminoglycoside in cases of intestinal pathology. They were catheterized and their intra-abdominal pressure was measured by connecting the catheter to a manometer on the 3rd, 5th and 7th postoperative days. The patients' haemoglobin and albumin levels were measured and resuscitative measures were carried out simultaneously when necessary.
Results
From July 2007 to June 2009, 190 emergency surgical laparotomies were carried out in our emergency department. RTL suture was used in 90 cases. In 100 cases, the abdomen was closed by continuous sutures. There were no cases of burst abdomens in the RTL group (Table 1).
RTL, reinforced tension line
In our series, 118 patients had an abdominal pressure in the range of 10–15 cm H2O (grade I intra-abdominal pressure) and 69 patients had an abdominal pressure reading ranging between 16–25 cm H2O (grade II intra-abdominal pressure) on the 3rd to 5th postoperative day.
A total of eight patients had a leakage from the intestinal anastomosis which was diagnosed clinically and confirmed by a water soluble oral contrast X-ray of the abdomen. Of these, five responded to conservative treatment. Three had to be treated surgically by creating a stoma and, later, a stoma closure.
There were 13 cases of burst abdomen between the 5th to the 9th day and in all these cases the abdomen was closed by continuous sutures. They were managed by resuscitation and by performing a laparostoma and, later, by a secondary closure. The intra-abdominal pressure at which burst abdomen occurred ranged between 14 and 22 cm H2O.
The intra-abdominal pressure in the RTL group was 10–26 cm H2O, reaching a peak value of 28 cm H2O in four cases on the 3rd to the 6th postoperative day (Table 1). The patients were closely monitored for signs indicating the development of abdominal compartment syndrome. Three patients had to be re-operated: laparostoma was created and the closure was done at a later date.
This whole procedure of RTL took about 10 min more than the standard procedure.
The analysis of results was done by using a chi-square test. On comparing the incidence of burst abdomen in patients operated by continuous suture technique and those operated by RTL suture technique, the P value was found to be 0.0026, which is highly significant.
On analysis of the incidence of burst abdomen in cases having grade II intra-abdominal pressure, the P value was found to be 0.0009, which is highly significant.
Discussion
Midline laparotomy performed in a contaminated abdomen is frequently complicated by wound dehiscence and burst abdomen during the immediate postoperative period and by incisional hernia during the late postoperative period. 1–5
Although laparotomy surgery has advanced in terms of technique, abdominal fascial closure often reflects a surgeon's reliance on tradition, experiment and experience. The effectiveness of closure is measured by the incidence of burst abdomen and wound dehiscence.
Ideally the closure should be fast and easy to perform, cost-effective and prevent early and late complications. Various techniques of fascial closure have been reported, such as layered closure, mass closure, retention closure, continuous closure and interrupted closure. However, an ideal technique of abdominal closure is yet to be universally accepted.
In layered closure, different layers are closed separately. It had been suggested that it is better in terms of preventing postoperative adhesions, wound dehiscence, etc. However, at the same time, it has been criticized for being a time-consuming procedure. Recent data suggest no difference in the incidence of wound dehiscence between this and other techniques. 3,6–9
Retention sutures were hypothesized to have additional strength but recent studies have shown no extra advantages. They have also been shown to cause more postoperative pain. 10
Continuous sutures evenly distribute the tension along the suture line. Mass closure by continuous sutures has been advocated for its superiority over layered closure as the former takes less time and has a lower incidence of burst abdomen. 7–12 However, even continuous sutures are known to tear the tissue in cases of increased intra-abdominal pressure.
The incidence of burst abdomen has been found to vary in different studies and different regions: 3.2% in USA, 13 10–30% in Asian countries 14 and 0.9–7% 4,6,12,15,16 in elective settings in various studies. Although various postulations have been put forth, the anatomical reason for burst abdomen is tearing of the tissue by the suture. The abdominal wall is a dynamic structure where the muscle contracts and relaxes. In closure of the abdomen by continuous suture, the suture tends to cut through the tissue by the ‘hack saw’ or ‘gigli saw effect’, leading to acute wound failure. This tear happens at the suture base and is attributed to the excessive horizontal tension.
This phenomenon of the ‘hack saw effect’ can be neutralized by increasing the area of contact of the suture with the tissue. One approach to achieve this is by placing the bites closely. 17 However, this will lead to ischaemia of the tissues lying between the rows of the suture and a consequent wound failure.
RTL distributes the peak pressure from the suture bases to the surrounding tissues; the sutures are usually placed approximately 1.5–2 cm apart over the entire tissue. By uniformly distributing this tension it has been shown that the tissue can withstand an additional tension of about 40 N. 18
Our study reveals that RTL prevents burst abdomen even in patients with poor general condition and grade II intra-abdominal pressure 19 (P value 0.0009).
In our study, all the patients who developed a burst abdomen had their wound closed by continuous mass closure at the initial surgery. The intra-abdominal pressure at which the burst abdomen occurred was much less compared to that in the patients in whom the abdominal closure was performed by RTL – and none of the patients in the RTL group had a burst abdomen.