
Abstract
Summary
Plasmodium vivax, thought to be benign until recently, has been associated with severe malaria and its complications. This retrospective study describes severe and complicated P. vivax malaria in children. It affected almost all of the organ systems and the most commonly found complications were thrombocytopenia and severe anaemia. All children with malaria, including malaria caused by P. vivax, should be monitored for such complications.
Introduction
About 247 million people per year are affected by malaria worldwide and there are 0.88 million deaths per year due to malaria. 1 Children are more likely to suffer from severe manifestations of the disease and of these almost 85% of deaths occur in children under five years of age. 1 Until recently, mono-infection by Plasmodium vivax was presumed to cause benign tertian fever and an uncomplicated course of disease. However, it has been noted that P. vivax can cause severe morbidity and even death.2,3 In this retrospective study we report our experience of managing severe and complicated malaria due to P. vivax infection in children.
Materials and Methods
The study was conducted at the Department of Paediatrics of a tertiary care centre in northern India between August 2010 and October 2011. Patients up to 14 years of age who tested positive for P. vivax malaria by blood smear examination and who had been admitted for treatment in the Department of Paediatrics were eligible for inclusion in the study. Children infected with P. falciparum, both P. vivax and P. falciparum, treated on an outpatient department (OPD) basis, empirically treated for malaria (negative for malaria parasite) and with other co-infection (tested when clinically indicated) were excluded from study. Data listing the demographic profile and the general and systemic examination findings were noted for all included patients. Complete blood counts and renal function tests were performed for all patients. Liver function tests, blood gas analysis and other tests (blood culture, serum Widal, dengue serology, etc.) were performed as clinically indicated.
Children with P. vivax infection were assessed for complications. Severe malaria and complications were defined as per the World Health Organization (WHO) criteria.4,5
Results
A total of 62 cases of malaria were admitted during the study period. Of these, 19 were excluded (15 with P. falciparum infection; 2 with both P. vivax and P. falciparum infection; 1 with P. vivax and enteric fever; and 1 with P. vivax and hepatitis A infection). The remaining 43 cases of P. vivax infection were included in the study. The mean (± standard deviation [SD]) age of children was 6.2 (±3.9) years (range, 6 months to 14 years). Just over half (53.5%) of the children were in the 0–5 year age group. There were 28 (65.1%) boys and 15 (34.9%) girls. Twenty-six (60.5%) were from rural areas and 17 (39.5%) were from urban areas. Fever was the main presenting complaint and was present in all patients except one (who presented with anasarca without fever). The mean (±SD) duration of fever before presentation was 6.8 (±3.9) days (range, 1–15 days). Chills and rigors were present in 23 (53.5%) and 18 (41.9%) and were absent in five (11.6%) and nine (20.9%) patients, respectively. Data regarding chills and rigors were not available for 15 (34.9%) and 16 (37.2%) patients, respectively. Presenting complaints other than fever and physical findings at admission are shown in Table 1. The diagnosis of P. vivax malaria was made by peripheral blood smear tests in all patients. The rapid card test were performed in four patients (P. vivax, 1; P. falciparum, 2; and both P. vivax and P. falciparum, 1) and these results corresponded with the peripheral blood smear results. The mean haemoglobin, total leucocyte counts and platelet counts of the patients are shown in Table 2. Serum calcium, phosphate and alkaline phosphatase (available for 10 children) and the coagulation profile (done for 7 patients) were within normal limits. Blood culture (17 patients), serum Widal (17 patients) and dengue serology (9 patients) were negative.
Presenting complaints other than fever and physical findings on admission in children with P. vivax infection
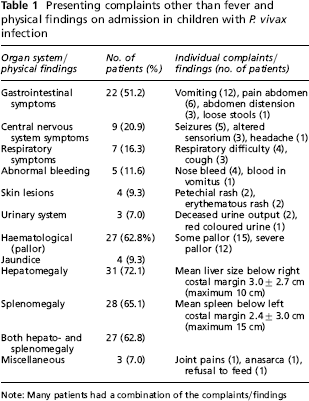
Note: Many patients had a combination of the complaints/findings
A comparison of complications suggestive of severe malaria and other findings in the present study and other studies in children with P. vivax infection
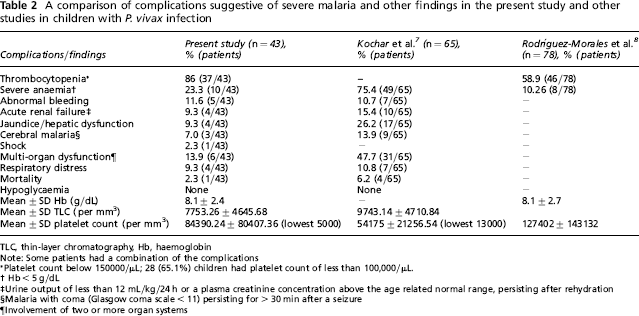
TLC, thin-layer chromatography, Hb, haemoglobin
Note: Some patients had a combination of the complications
Platelet count below 150000/μL; 28 (65.1%) children had platelet count of less than 100,000/μL.
Hb < 5 g/dL
Urine output of less than 12 mL/kg/24 h or a plasma creatinine concentration above the age related normal range, persisting after rehydration
Malaria with coma (Glasgow coma scale < 11) persisting for > 30 min after a seizure
Involvement of two or more organ systems
Glucose-6-phosphate dehydrogenase (G-6PD) estimations were available for 18 patients: one was deficient; three were indeterminate; and 14 were normal. The complications suggestive of severe malaria due to P. vivax infection are summarized in Table 2. All patients had one or more complications with the most common being thrombocytopenia (Table 2).
Oral chloroquine (10), oral artesunate (4), injection artesunate (29) and injection quinine (1) were used as antimalarials. Prophylaxis for relapse was used as per the WHO recommendations. Eight children received packed cell transfusion, three received platelet concentration and three received both packed cell and platelet concentration. Fever subsided within 24 hours of the start of treatment in 20 patients (46.5%) and within the next 24 hours in eight (18.6%). The mean (±SD) duration of hospital stay was 6.4 (±2.9) days with a range of 2–16 days. All except one patient survived. The child who died was admitted with fever, jaundice, seizures and altered sensorium and succumbed due to massive hematemesis and pulmonary haemorrhage.
Discussion
In studies from Indonesia, Papua New Guinea, Thailand and India about 21–27% of patients with severe malaria were associated with P. vivax monoinfection. 6 Most case reports describe complications due to P. vivax malaria in children.
Kochar et al. 7 (from Bikaner, India) and Rodríguez-Morales et al. 8 (from Sucre, Venezuela) presented series on complicated P. vivax malaria in children – cases of only anaemia and thrombocytopenia were included in a later study. The proportion of children with severe malaria in the 0–5 year age group was 53.5% (23/43) in the present study and 75.7% in the study by Kochar et al. 7 The comparison of complications suggestive of severe malaria and other findings of the present study and other studies in children with P. vivax infection are shown in Table 2.
There were some limitations in our study. We were unable to corroborate the species identification by polymerase chain reaction (PCR) as this facility is not currently available at our centre. However, in symptomatic individuals, compared with PCR, microscopy was found to have a sensitivity of 86.6% (95% confidence interval [CI], 77.8–92.4) and specificity of 100% (95% CI, 96.9–100). 9 Thus, it is unlikely that there was any misclassification of the species using blood smear examinations.
Conclusion
The P. vivax malaria which, until recently, was considered to be benign malaria may cause severe malaria in children with significant morbidity and even, although uncommon, mortality. Thrombocytopenia and severe anaemia were the most common complications of P. vivax malaria in children. We suggest that all children with malaria should be carefully monitored, even those with P. vivax malaria.