
Abstract
Objectives
To evaluate the hypothesis that ultrasound-guided subacromial steroid injection produces greater reduction in morbidity than unguided injection.
Design
All patients underwent either ultrasound-guided subacromial injection with 80 mg Depo-Medrone at Bradford Royal Infirmary (group 1) or unguided injection (group 2) by a general practitioner with a specialist interest in musculoskeletal medicine (GPwSI). Patients were clinically and ultrasonically diagnosed with subacromial impingement syndrome.
Setting
Patients in group 1 included both hospital and GP referrals. Patient in group 2 were GP referrals to GPwSI.
Main outcome measures
Comparison was made of pre-injection and six week post-injection Oxford shoulder score and a 0–10 pain score.
Results
Forty-one patients received guided injections (group 1) and 17 unguided (group 2). Group 1 showed a significant mean reduction in the Oxford shoulder score of 9.10 (95% CI 7.07–11.13, P < 0.0001) and a significant change in the mean 0–10 pain score of −3.26 (95% CI −2.51 to −3.88, P < 0.0001). Group 2 also showed significant reduction in the mean Oxford shoulder score of 9.94 (95% CI 6.41–13.47, P < 0.0001) and significant change in the mean 0–10 pain score of −2.94 (−1.95 to −3.93, P < 0.0001). Comparison of groups 1 and 2 for each outcome measure revealed no significant differences.
Conclusion
Our data confirm the efficacy of steroid injection in the management of subacromial impingement, although no significant difference is found when comparing the two groups. We recommend the continued use of unguided injections, with ultrasound used for more practically difficult cases and where there is diagnostic uncertainty.
Shoulder pain is a common clinical complaint and is estimated to account for between 12 and 25/1000 general practitioner (GP) consultations. Approximately one-third of these are related to inflammatory changes in the rotator cuff muscle tendons and associated bursae. 1 Subacromial impingement syndrome is caused by an abnormal contact between the greater tuberosity of the humerus and the under surface of the acromion during abduction of the shoulder. This abnormal contact usually occurs at 60–120° of shoulder abduction resulting in a painful arc in mid-abduction. 2,3
The causes of subacromial impingement are multifactorial. A common contributing factor is weakness or damage to the rotator cuff muscles caused by trauma or age-related degenerative weakness. This results in a vicious cycle where pain limits movement and further weakens the rotator cuff muscles.
Local steroid injection is a widely accepted method of treatment for impingement syndrome, 4,5 although it is not without potential risks including septic arthritis and tendon degeneration leading to rotator cuff weakness or rupture. However, the optimal technique for performing steroid injections is not so clear. Early studies showed greater efficacy if steroid injections were directed to a specific anatomical site within the shoulder rather than the point of pain. 6 This is likely to be secondary to the large variability of symptoms produced by each different shoulder pathology. In subacromial impingement, there is evidence to support greater efficacy of steroid injections if introduced correctly into the subacromial space. 7–9 The most common method of steroid injection in primary care is to use anatomical landmarks to guide the injection to the expected site of the subacromial space. Reported rates of successful injection into the subacromial space vary from 29% to 100%. 7–10 Such variable rates of success are likely to be due to the wide range of practitioner experience and patient factors such as body mass index. Ultrasound can be used to guide injections into the correct compartment under direct visualization. Ultrasound is a safe, cheap and quick modality that may, therefore, increase the efficacy of steroid injections.
In the UK, shoulder pain is increasingly being managed in primary care by GPs with a specialist interest in musculoskeletal medicine (GPwSI). Diagnosis of subacromial impingement is often made clinically in this setting and the decision to perform a steroid injection is frequently made at the initial consultation. Some patients will be referred for a diagnostic ultrasound prior to treatment; however, many will return to the GP for unguided subacromial injection. Other patients will have ultrasound-guided injections performed most commonly by a radiologist.
We aim to compare the outcome of unguided injections with those performed under ultrasound guidance for the specific condition of subacromial impingement syndrome. We, therefore, hope to evaluate the theory that ultrasound-guided injections are more accurately injected into the subacromial space and, therefore, will produce greater therapeutic effect. To the best of our knowledge, our study represents the largest comparison of guided versus unguided steroid injections in patients with subacromial impingement.
Methods
The need for ethical approval was discussed with the local ethics and research and development committees. We were informed that as the only change to the patient pathway would be the completion of patient questionnaires (as explained later), there was no requirement to approach the committees formally.
Patients eligible for inclusion in the trial comprised two groups. The first group included all patients referred for ultrasound-guided subacromial injection at Bradford Teaching Hospitals NHS Trust between April and December 2009 (group 1). Injections were performed by either an experienced consultant radiologist (CG, MC) or a senior registrar under their direct supervision. The site of injection was confirmed by direct visualization in this group using ultrasound. The second group comprised patients referred to GPwSI in musculoskeletal medicine during the same time period (group 2). Injections were performed by two GPwSI (MB, AC) or a senior physiotherapist (RS). Patients in both groups, regardless of ultimate method of injection, had to have been diagnosed with subacromial bursitis clinically and had the diagnosis confirmed ultrasonically no more than six weeks prior to injection. Exclusion criteria included patients under 18 years of age, patients with rotator cuff tears or patients who had previous shoulder surgery. Patients were all injected with 80 mg Depo-Medrone (Pharmacia, Pfizer Ltd, Surrey, UK) and 3–10 mL of Bupivacaine or Lidocaine. Any difficulties in performing the injection were documented.
Prior to injection all patients completed a questionnaire asking them to record all previous therapy for the painful shoulder and any current analgaesia. Following this, the patient completed the Oxford shoulder score and a pain score (0 = no pain at all, 10 = worst pain ever). The Oxford shoulder score is a validated questionnaire comprising 12 questions evaluating pain, night pain and impact on daily activities. 11
Guided injection was performed with the patient sitting upright with the affected arm behind the patient's back. The subacromial bursa was identified in longitudinal or transverse section and a point approximately 1 cm lateral to the transducer was marked. A 21 G green needle was inserted into the subacromial bursa under direct vision using an aseptic technique. The steroid followed by the local anaesthetic was then injected via a connector. The needle position and bursal distension were confirmed immediately by ultrasound, confirming selective injection and preventing inadvertent glenohumeral joint injection (Figures 1 and 2).
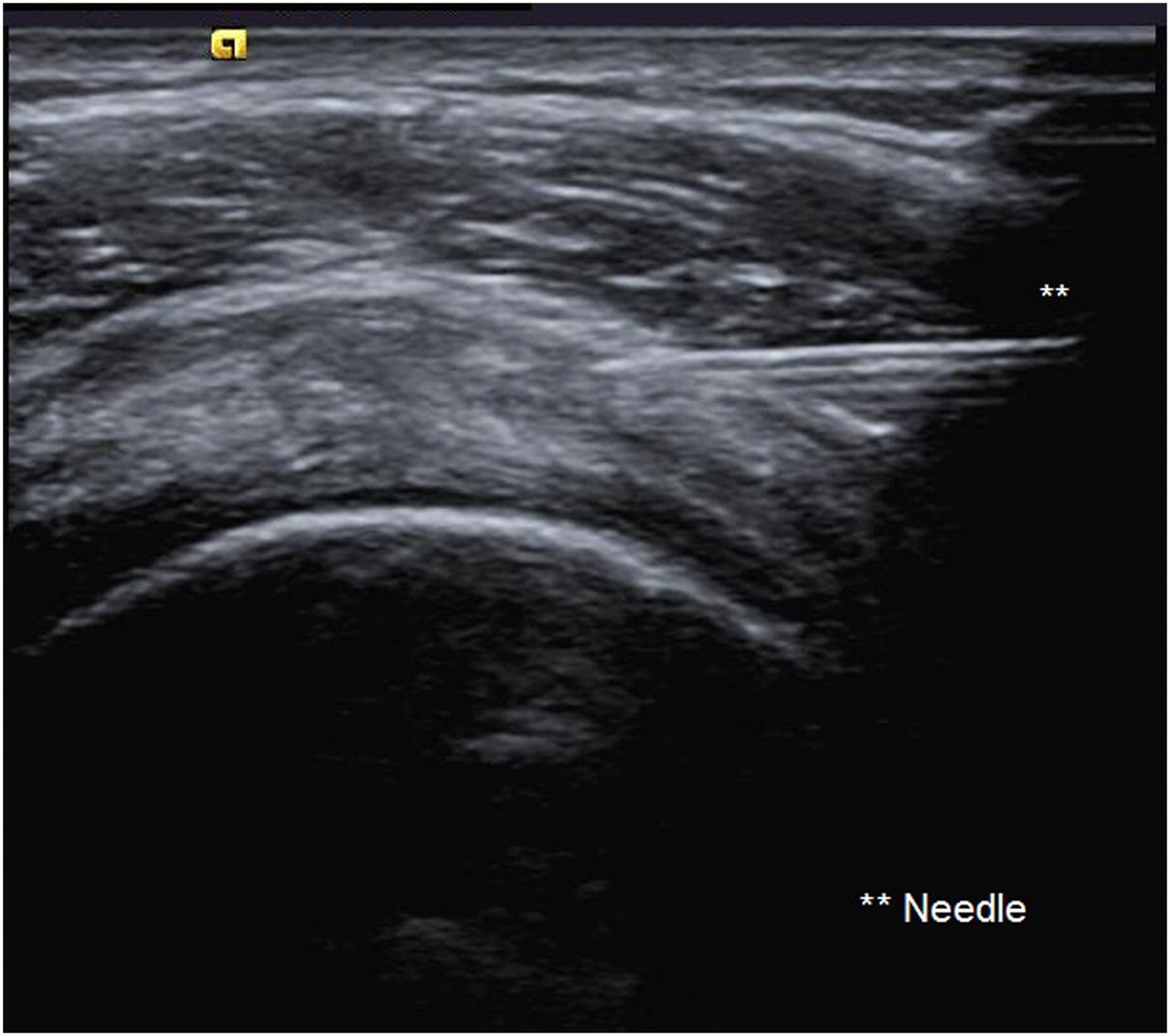
Image showing the needle with its tip within the subacromial space
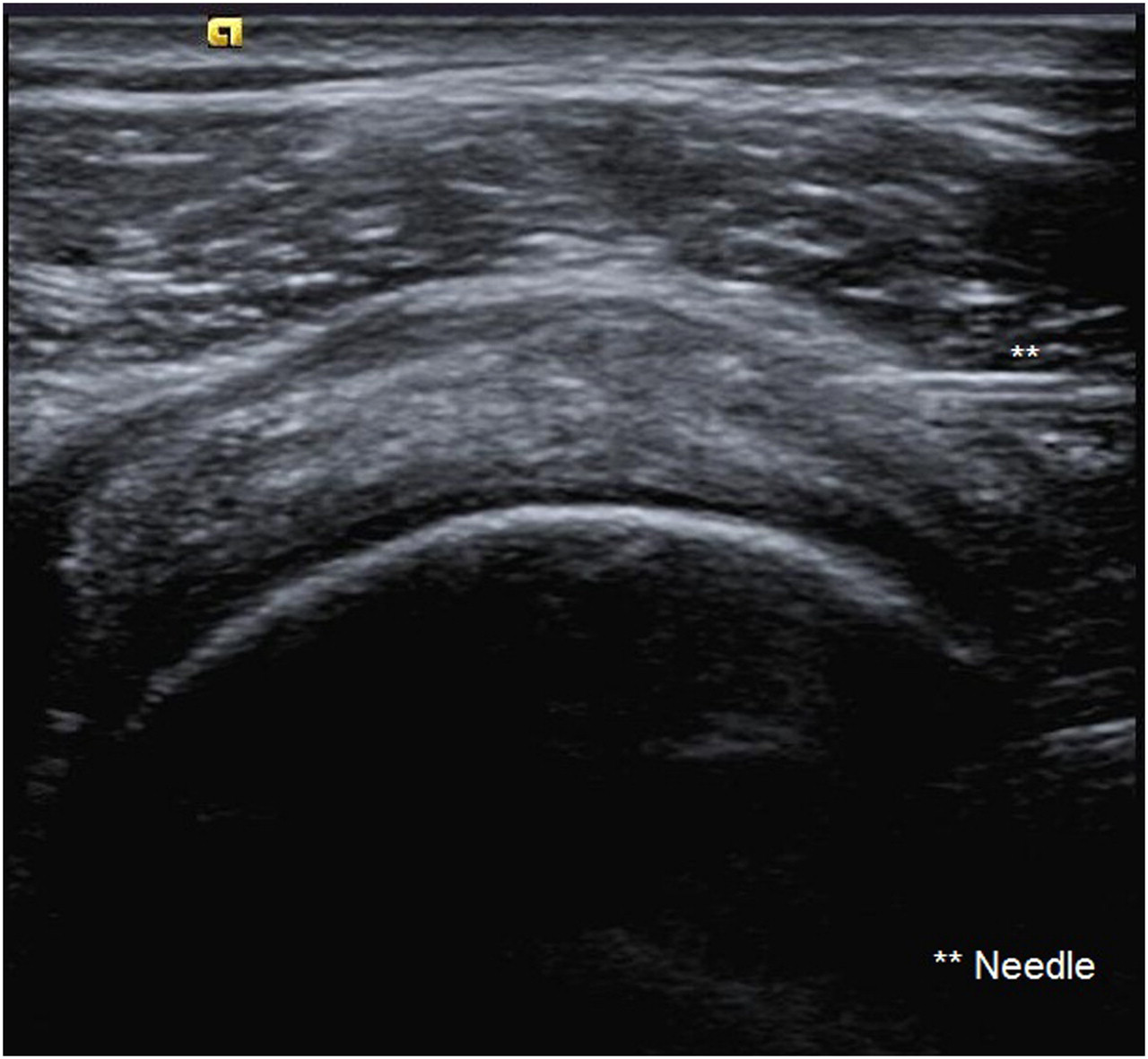
Image showing bursal distension following injection of corticosteroid
Unguided injection was also performed with the patient sitting upright with the affected arm behind the patient's back. The acromion was palpated and its anterior and posterior borders marked. A position 2.5 cm below this was also marked. A 21–23 G needle (depending on body habitus) was inserted angling slightly underneath the acromion process. Steroid followed by local anaesthetic was then injected in the expected location of the subacromial bursa using the same needle but a different syringe. While inadvertent glenohumeral joint injection could not be excluded in this group of patients, this reflects the real practice of unguided injections.
Telephone follow-up was performed at 6–8 weeks following injection. Details of any previous treatments were confirmed and details of new therapies, including any changes to analgaesia were recorded. The Oxford shoulder score and pain score were repeated.
Statistical analysis using a paired t-test was performed to assess the significance of outcomes following injections in the individual groups. Comparison of the resulting confidence intervals and analysis using an unpaired t-test was performed to evaluate any difference between the two groups.
Results
In total, 80 patients were entered into the study between April and December 2009. Of these, a total of 22 were excluded, 20 from group 1 and two from group 2. The reason for exclusion included 13 patients who were unable to be contacted during the follow-up period, six who were unable to complete the follow-up telephone call due to language difficulties, two due to previous surgery and one patient who was on long-term steroids.
Of the remaining 58 patients, 41 were in group 1 and 17 in group 2. No significant differences in gender, age or history of previous injections were present between the two groups (P > 0.05). Furthermore, no significant difference was present in the pre-injection Oxford shoulder score and pre-injection pain score between the two groups (P > 0.05). The two groups combined included 22 men and 36 women with a mean age of 54 years (range 25–80).
Group 1 had an initial mean Oxford shoulder score of 23.20 and a post-injection mean Oxford shoulder score of 32.29, showing a statistically significant mean difference of 9.10 (95% confidence interval [CI] 7.07–11.13, P < 0.0001). The initial mean pain score in this group was 7.68 and post-injection mean pain score was 4.49, again showing a statistically significant mean difference of −3.26 (95% CI −2.51 to −3.88, P < 0.0001). Therefore, ultrasound-guided injection is found to be beneficial in both outcome measures after a period of 6–8 weeks.
Group 2 had an initial mean Oxford shoulder score of 19.10 and a post-injection mean Oxford shoulder score of 29.12, showing a statistically significant mean difference of 9.94 (95% CI 6.41–13.47, P < 0.0001). The initial mean pain score in this group was 8.47 and post-injection mean pain score was 5.53, again showing a statistically significant mean difference of −2.94 (−1.95 to −3.93, P < 0.0001). Therefore, unguided injection is also found to be beneficial in both outcome measures after a period of 6–8 weeks.
When comparing groups 1 and 2, no significant difference is found for either outcome measure. The Oxford shoulder score analysis reveals a mean difference of only 0.8 in favour of group 2 (95% CI −2.95 to 4.63, P = 0.66) (Figure 3). The pain score analysis revealed a mean difference of only −0.26 in favour of group 1 (95% CI −1.47 to 0.95, P = 0.67) (Figure 4).
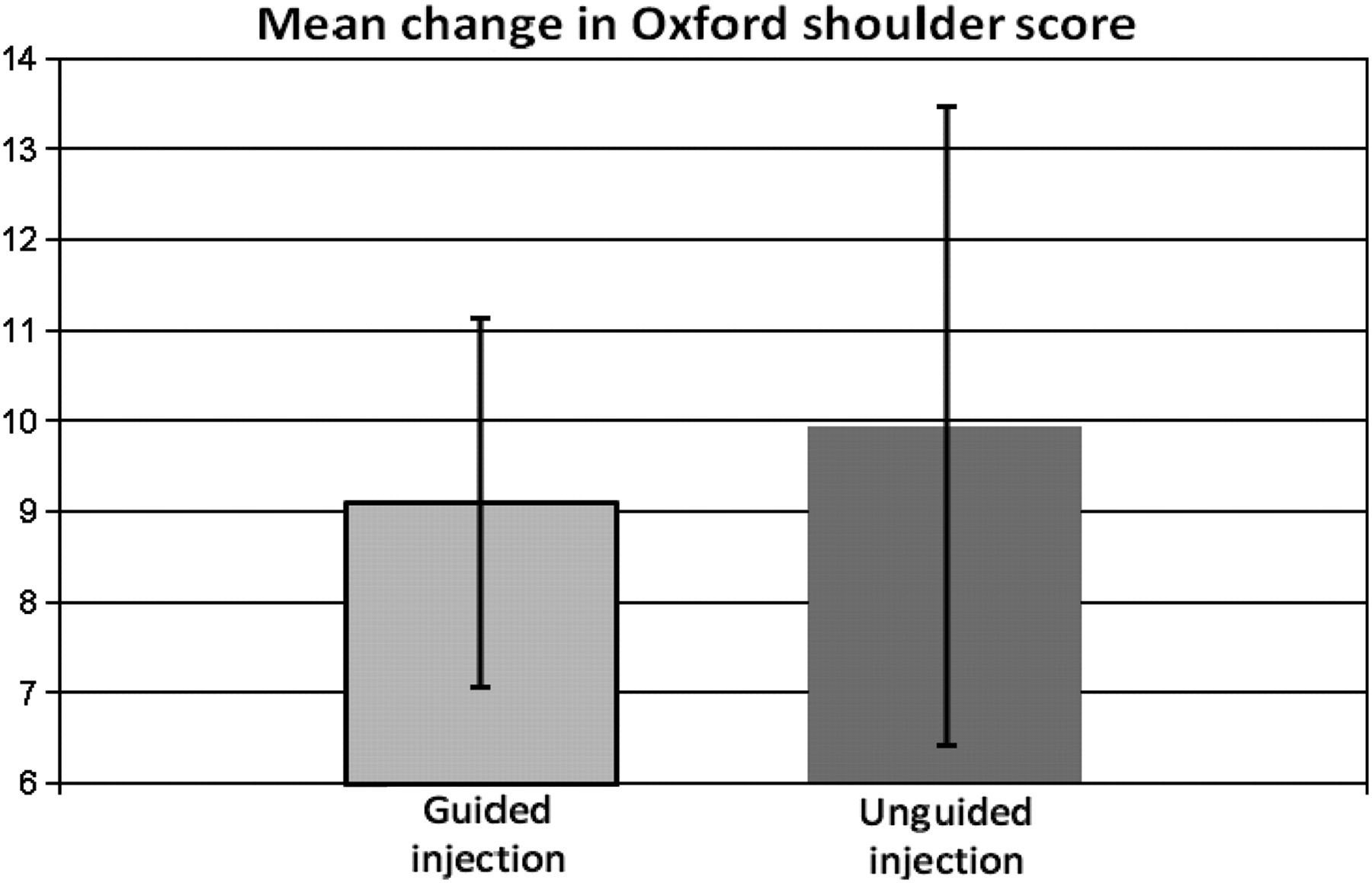
Mean change in Oxford shoulder scores (error bars indicate 95% confidence interval)

Mean reduction in 0–10 pain score (error bars indicate 95% confidence interval)
Two patients in group 1 started new medications during the follow-up period. One patient changed from Pregabalin to Lamotrigine for a separate lower limb pain and the other started new 8/500 co-codamol. One patient in group 2 changed from 30/500 co-codamol four times daily to 50 mg of tramadol twice daily.
Discussion
The use of steroid injections in the treatment of subacromial impingement is a common practice in the UK. It is performed by many different practitioners with varying levels of experience in many settings, including primary care, rheumatology and orthopaedic clinics and the radiology department. Multiple different techniques are used, with varying doses of drugs and at different time intervals. Injections are often combined with other forms of treatment to maximize symptom relief for patients.
Our aim was to evaluate the specific question of whether ultrasound guidance improves outcomes in the treatment of subacromial impingement. Our results support the view that steroid injection is an effective short-term treatment for subacromial impingement syndrome. However, we found no significant difference in outcome between ultrasound-guided injection and unguided injections.
There is a wide variety of information regarding the use of steroid injections for the treatment of shoulder pain in the published literature, although much of this work has not been done specifically for the subset of patients with subacromial impingement. Patients presenting with shoulder pain now have greater accessibility to diagnostic ultrasound, which allows the exclusion of the main differential diagnosis of complete or partial rotator cuff tear. Subacromial impingement is, therefore, being more accurately diagnosed and an evidence base for treatment of this subgroup is of increased importance.
The management of shoulder pain and subacromial impingement is a complex area. There are various treatments including physiotherapy, heat therapy, transcutaneous electrical nerve stimulation, acupuncture, ultrasonic therapy, non-steroidal antiinflammatories, steroid injections and surgical decompression. The wide variety of treatments for shoulder pain has been investigated by two meta-analyses that indicate support for local injection of steroids only. 12,13 Only limited evidence is available for the remaining treatment options. Both of these meta-analyses were limited by small sample sizes in the reviewed studies and the comparison was limited by variation in injection technique, outcome measures and patient follow-up regime.
Data included in these meta-analyses showed steroid injection to be better than both placebo and non-steroidal anti-inflammatory drugs in the management of shoulder pain. 4,5 These studies made some attempts to exclude patients with rotator cuff tears but, unlike in our study, ultrasound was not performed to confirm this. Some subsequent conflicting published data have found no significant difference in outcomes following injection of steroid/local anaesthetic versus local anaesthetic alone. 14 More focused investigation into patients with suspected subacromial impingement has shown a significant improvement in symptoms with steroid injection, 15,16 a finding consistent with our results.
A Cochrane review by Buchbinder et al. pooled the data from two studies and concluded that there may be a small benefit with steroid injection in the treatment of rotator cuff disease. 4,5,17 The definition of rotator cuff disease was not made but in light of the papers included this group is likely to include some patients with at least partial rotator cuff tears. Overall, this review concluded that for the general presentation of shoulder pain, there is little current robust evidence for the use of steroid injection in treatment. A further meta-analysis by Arroll and Goodyear-Smith 18 pooled the data from all five studies discussed above and concluded that significant improvement in symptoms was achieved with steroid injection in the treatment of what the review describes as ‘rotator cuff tendonitis’. This meta-analysis, therefore, included studies specifically for subacromial impingement and those that did not fully exclude rotator cuff tears.
A number of studies have evaluated whether correct placement of steroid injection after unguided injection correlates with efficacy in shoulder complaints. Increased efficacy related to correct placement was demonstrated in one study group of 37 patients; however, this was not limited to either subacromial impingement cases or subacromial injections. 8 Studies have been performed in groups clinically diagnosed with impingement syndrome. This includes a study of 53 patients with impingement where correct placement of steroid using an unguided technique was found in 70% of patients. 19 Patients were assessed for response after only 15 minutes. This found no statistical improvement related to correct injection site; however, this may have been due to the short follow-up period. A longer follow-up period of two weeks was evaluated in 48 patients with impingement, which found accurate injection placement in 87% of patients. 9 All patients showed improvement of symptoms when assessed at 30 minutes post-injection; however, only the group with correct placement showed significant improvement after two weeks. Finally, a six-week follow-up was performed in 33 patients with impingement. 20 This group used magnetic resonance imging to assess location of injection and exclude full thickness rotator cuff tears. They found accuracy of injection into the subacromial bursa in 70% of patients. Statistically significant pain relief and improved function was found at 24 hours in only the group with correct placement of steroids. Incorrect placement resulted in increased pain after 24 hours. Follow-up at six weeks showed no significant change in pain for either group. Most of these studies made a diagnosis of impingement clinically and, therefore, may have included patients with rotator cuff tears. Overall, the data are, therefore, mixed with only two studies showing continued efficacy during the follow-up period. Interestingly, ongoing efficacy was found only in the groups where steroid placement was correct.
A small number of studies have compared ultrasound-guided injection with unguided injections. A study group of 41 patients with a mixture of shoulder conditions including rotator cuff tears were evaluated after randomization to either guided or unguided steroid injection. 7 In the unguided group, correct placement of the steroid was found in only 30% of patients. Follow-up performed at six weeks showed significantly greater improvement in the guided injection group.
A further group of 40 patients with sonographically confirmed subacromial bursitis was followed up one week after either guided or unguided injection. 21 This revealed a significantly greater range of abduction in those patients treated with an ultrasound-guided injection. No assessment of pain was evaluated and patients were followed for only one week; therefore, medium- to long-term outcomes were not assessed.
Finally, 16 patients were followed up for only 30 minutes after injections of Lidocaine only. 22 All patients had a clinical diagnosis of impingement, although eight of the 16 patients had bursal sided rotator cuff tears. All patients were treated with a guided and unguided injection at one-week intervals and assessment of pain was made at five-minute intervals up to 30 minutes after each injection. This revealed significantly greater reduction in pain in the ultrasound-guided group. Interestingly, 15 out of 16 patients commented that they preferred the ultrasound-guided injection.
Ekeberg et al. 23 have compared local and distant gluteal steroid injection in 106 patients with rotator cuff pathology. This found no significant difference in outcome between the two groups. As our hypothesis is that unguided injection is more likely to produce a ‘distant’, extra-bursal injection, this outcome is in keeping with our results. Ultrasound was used in this study to direct shoulder injections; however, patients with rotator cuff tears were not excluded. All patients also underwent ultrasound-guided steroid or local anaesthetic injection; therefore, all patients did have image-guided needle puncture of the subacromial bursa with administration of local anaesthetic. This may confound the results as it is not clear what the effect of accurate dry needle subacromial bursa puncture or local anaesthetic administration is.
A recently published cost-efficacy analysis compares training GPs in shoulder injection versus no training. 24 This suggests that training GPs in shoulder injection techniques incurs an extra annual cost of £211, and this produces an extra 0.075 quality-adjusted life-years (QALY) per patient. This equates to an estimated cost of £2813 per QALY. The study concluded that there is a greater than 95% confidence that the true cost is less than £20,000 per QALY. The National Institute for Health and Clinical Excellence has an approximate upper threshold of £20,000–25,000 below which an intervention is deemed cost-effective. 25 It is, therefore, likely that training of GPs would be cost-effective. A comparison with the cost efficacy of ultrasound-guided injection in hospital would be a potential area for further study.
The findings from our study will be of interest to many practitioners who perform therapeutic injections in the primary care setting. While the added initial cost of an injection at the time of first diagnostic ultrasound is unlikely to be significant compared with an initial GP injection, the cost of repeated injections in the hospital setting is likely to be higher than that in primary care. However, a formal cost comparison has yet to be undertaken. Keeping subacromial injections in the primary care setting is also likely to be in the interest of patients, as many find it easier to make repeated visits to their local GP rather than having to make the often longer journey into hospital. This may have the resultant effect of improving compliance and allowing the GP to monitor relative success more closely. Again, these potential benefits have not been formally assessed.
We appreciate that our study is not without limitations. The study required a clinical diagnosis of impingement and an ultrasound to confirm the absence of a rotator cuff tear within the preceding four months. Patients with a history of surgery were also excluded. However, the lack of further exclusion criteria such as glenohumeral degenerative change does introduce a number of confounding factors to our data, although we feel this is more representative of real practice. The differences in referral populations to the two different groups will inevitably introduce some elements of selection bias. While our two groups were not randomized, there were no significant differences in age, gender or number of previous injections between the two study groups. In addition, all patients had an ultrasound within six weeks prior to any injection regardless of which group they belonged to in order to ensure that no patients had a rotator cuff tear. Of more importance was that there was also no significant difference between the pretreatment Oxford shoulder score or pain score between the two groups and, therefore, we feel that a comparison of treatment efficacy between these two groups is valid. In addition, the nature of this study reflects the current clinical practice in most regions of the UK. While a disproportionately large number of patients were excluded from group 1, many of these were due to problems with contacting or language difficulties and we felt it was important to exclude patients from whom we could not gain accurate information in order to ensure fair comparison between the two groups. A further limitation of the study is the small numbers involved and this is particularly true of group 2 (GPwSI group). It would have been possible to recruit more patients into this group had we relaxed the inclusion criteria. However, we felt it was crucial that these patients had had a recent ultrasound to exclude rotator cuff tear so that we were comparing two groups with similar pathologies. No specific assessment was made regarding the incidence of postprocedure complications between the two groups; however, many of these would be encompassed by the follow-up questionnaire. Future study should include a longer follow-up period in order to assess long-term complications such as tendon rupture.
Conclusion
Despite its limitations, our study represents the largest published prospective comparison of guided versus unguided steroid injections in patients with subacromial impingement, and one that we feel accurately represents current UK practice. Our results build on the available data to suggest equal efficacy of both guided and unguided injection of steroid in the management of subacromial impingement syndrome. There is indeed scope for a large randomized controlled trial comparing ultrasound-guided versus unguided steroid injection in patients who have had an imaging-based diagnosis of subacromial impingement or bursitis. In summary, our results support the continued use of unguided injections, while there is certainly a role for ultrasound guidance to be used for more practically difficult cases and where there is diagnostic uncertainty.
Footnotes
Acknowledgements
We would like to thank Dr Mark Brooke (MB), Dr Anne Connolly (AC) and Rose Sutcliffe (RS) for all their help in performing the unguided injections.