
Abstract
Persistent hyperplastic primary vitreous is a result of failure of regression of the embryonic hyaloid artery and presents commonly as leucocoria in the first few weeks of life. It leads to abnormal lenticular development and secondary changes in the retina and orbit. We discuss two cases of persistent hyperplastic primary vitreous with unusual findings. The first case is an example of unilateral involvement, and on high frequency ultrasound, the commonly associated retrolental mass was absent. The hyaloid artery was well visualized on colour and spectral Doppler. The second case had bilateral retrolenticular masses. The hyaloid artery could be demonstrated in one side on colour Doppler. Thickening of the choroido-retinal layer was noted in both sides. Retinal detachment or vitreous haemorrhages, which are commonly associated findings with persistent hyperplastic primary vitreous, were not seen in either case.
Keywords
Persistent hyperplastic primary vitreous presents commonly as leucocoria (a white pupillary reflex due to abnormal reflection from retina) at birth or during the neonatal period. This sporadic condition is most commonly unilateral. Rare bilateral cases are usually associated with syndromes. Failure of regression of the primary vitreous results in its proliferation and a retrolental mass is formed. This mass is attached to the optic disc by a fibrovascular band. 1 The artery in this primary vitreous, if not regressed, often causes vitreous haemorrhage in early life. The overall shape of persistent hyperplastic primary vitreous has been likened to a cocktail glass. 2 Retinal detachment is a common association. High frequency ultrasound is the preferred modality for evaluation. Visualization of the artery excludes retinal detachment or retinal haemangioblastoma. Demonstration of the hyaloid artery by colour Doppler on the band is pathognomonic. 3 Complications include haemorrhage and glaucoma. Various surgeries for visual rehabilitation have been described. 4 We describe two cases; one case of unilateral persistent hyperplastic primary vitreous with no retrolental mass and the other having bilateral retrolental masses and thickening of choroido-retinal layer.
Case report
Written consent was obtained from the parents of the infants for the use of their details and images.
Case 1: A three-month-old male infant presenting with unilateral leucocoria was referred for high frequency ultrasound of the left orbit. He did not have any other obvious congenital anomaly. The ultrasound examination was performed using an 8000 Ex Prime ultrasound unit (Medison, South Korea) and a 5–10MHz broadband linear transducer. On ultrasound the lens appeared normal. No retrolenticular mass was noted. A hyperechoic band was seen extending from the optic disc to the posterior aspect of the lens (Figure 1a). The thickness of the band measured 2–3 mm. Colour Doppler was performed with gain set at 50, the pulse repetition frequency at 1 kHz and a frame averaging of 2. The hyperechoic band showed colour flow with direction towards the lens (Figure 1b). On spectral Doppler with gain at 70, pulse repetition frequency of 2.5 kHz and a narrow sample gate of 1 mm, the flow was found to be pulsatile indicating a persistent hyaloid artery (Figure 2). No other finding was noted in the orbit. The other orbit was unremarkable on ultrasound (Figure 3).
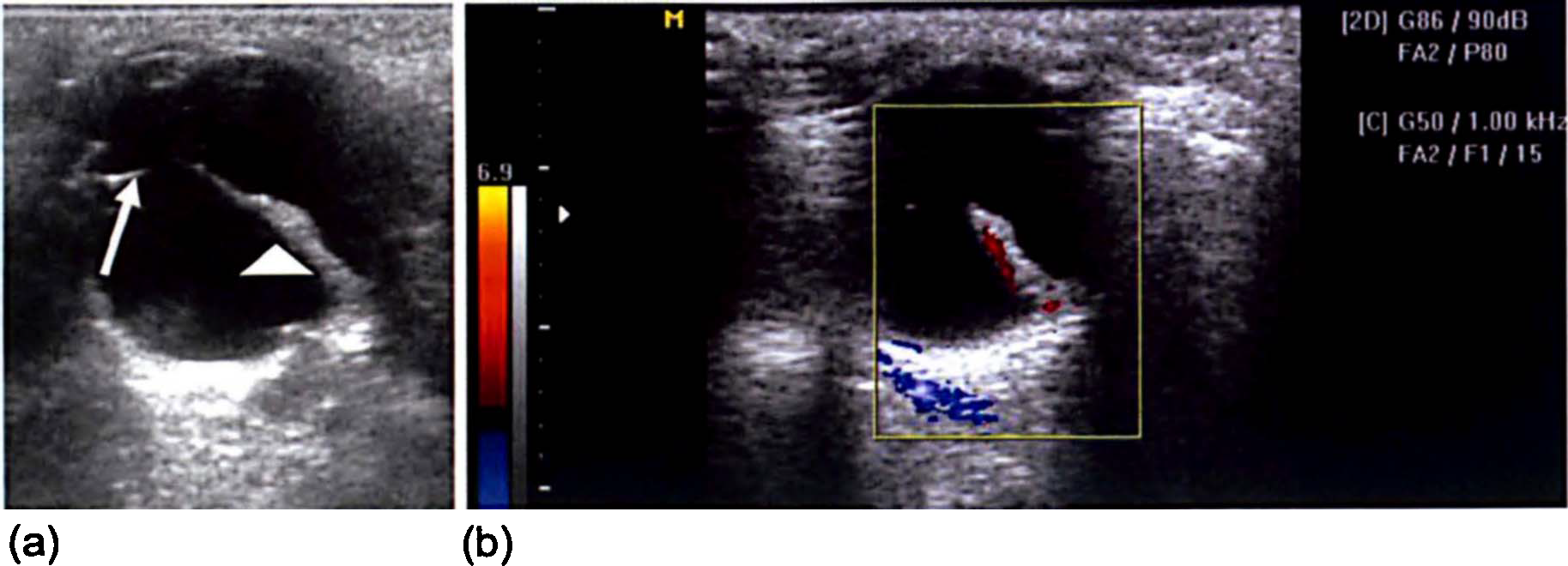
Case1: (a) Left orbit shows a hyperechoic band (White arrowhead) extending from the optic disc to the posterior aspect of the lens (White arrow). (b) Colour Doppler indicating the presence of the hyaloid artery with flow towards the lens
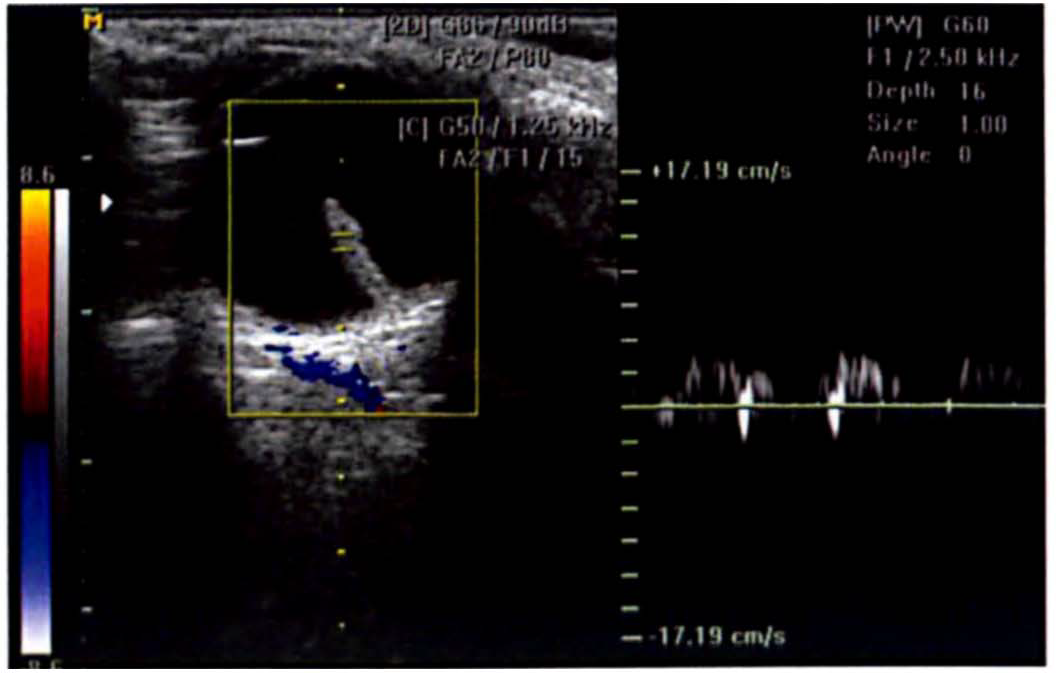
Case 1: Pulsed Doppler shows a pulsatile waveform indicating arterial flow
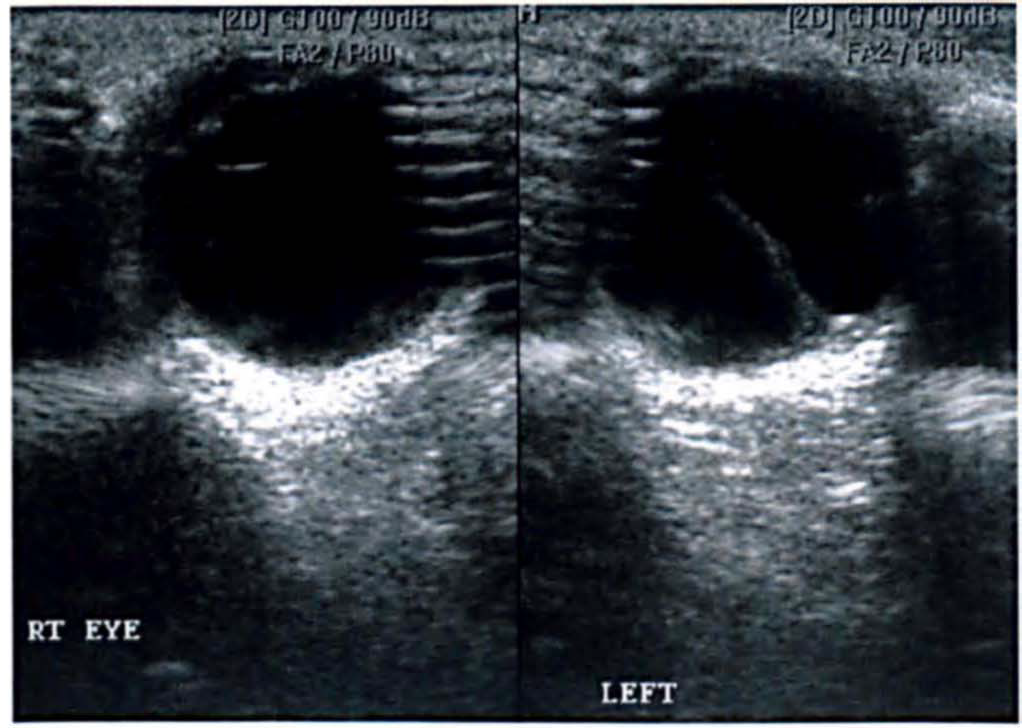
Case 1: The right orbit has a normal lens and clear vitreous. The left orbit demonstrates a hyperechoic band extending from the optic disc to the posterior aspect of lens
Case 2: A six-month-old male infant presenting with bilateral leucocoria was referred for high frequency ultrasound of both orbits. He did not have any other obvious congenital anomaly. The ultrasound examination was performed using an Esaote My Lab 50 (Esaote, Italy) and a 5–10 MHz broadband linear transducer. The right orbit showed a retrolenticular mass with a hyperechoic band extending from the optic disc to the posterior aspect of lens (Figure 4). The thickness of the band measured 3–4 mm. In addition, thickening of the choroido-retinal layer was present.

Case 2: The right orbit shows a retrolenticular mass with a hyper-echoic band extending from the optic disc to the retrolenticular mass. Note choroido-retinal thickening
The left orbit also showed a retrolenticular mass with a thin hyperechoic band extending from the optic disc to the posterior aspect of lens. The thickness of the band measured 1–2 mm. On colour Doppler, the hyperechoic band showed flow towards the lens (Figure 5). Thickening of the choroido-retinal layer was again present.
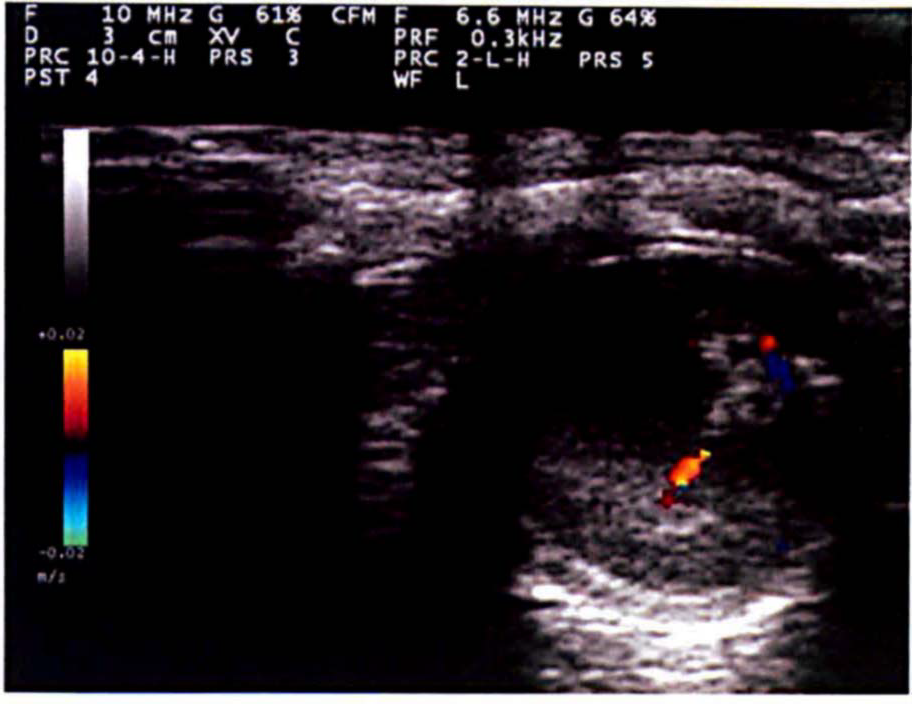
Case 2: Colour Doppler of the left orbit indicates the presence of a blood vessel with flow towards the lens. Vitreous opacities with choroido-retinal thickening are visible
The patient with unilateral involvement was managed conservatively. To date, the patient with bilateral involvement has not reported for follow up.
Discussion
Persistent hyperplastic primary vitreous is usually noted at birth or in early life. Rarely, cases manifesting in adults have been reported. The occurrence is sporadic. A predilection for whites is suggested. 1 The condition is unilateral in more than 90% of cases, and can be associated with Von-Hippel Lindau disease. 2 Rare bilateral cases have been reported with Norrie disease, Warburg syndrome, and other neurological and systemic anomalies. 1 Bilateral persistent hyperplastic primary vitreous is rare. In a large study of 83 cases, only two patients (2.4%) had bilateral involvement. 5 Common clinical signs are leucocoria and microphthalmia. 6 Sometimes it is associated with other ocular anomalies.
During early embryonic life, the hyaloid artery develops from a branch of the ophthalmic artery and gains access to the lentiretinal space via the choroidal fissure on the ventral surface of the optic stalk. The hyaloid artery vascularizes the developing retina and initially also vascularizes the lens vesicle. The lips of the choroidal fissure fuse by day 33, enclosing the hyaloid artery and accompanying vein in a canal in the ventral wall of the optic stalk. When the lens matures during fetal life and ceases to need a blood supply, the portion of hyaloid artery that crosses the vitreous body degenerates and is removed by macrophages by the end of the fourth month. The proximal part of the hyaloid artery becomes the central arterial supply for the retina. 7 When this primitive mesenchymal tissue persists and continues to proliferate, a retrolental mass is formed. The fibrovascular tissue behind the lens varies in extent and thickness. In the first few months of life vitreous haemorrhage is common. Retinal detachment is seen in 30–56% of cases. 1
The condition has been detected antenatally at 23 weeks of gestation. It was visualized as a hyperechoic lens and bizarre thickness of the hyaloid artery –lens junction. 8
High frequency B-mode ultrasound is a simple, cost-effective and useful investigation for evaluating the orbit. In a normal eye, the vitreous is clear and the lens has a thin hyperechoic rim. In persistent hyperplastic primary vitreous, ultrasound is usually diagnostic and is the investigation of choice. It demonstrates a hyperechoic mass posterior to the lens. A hyperechoic band extending from the posterior pole of the globe to the posterior surface of the retrolental mass, corresponding to the hyaloid canal, is also seen. Ultrasound may demonstrate other associated findings like retinal detachment and vitreous haemorrhage. We did not find a retrolental mass in the case with unilateral involvement.
Within the hyaloid canal, the hyaloid artery may be seen with Doppler imaging. 9 The incidence of visualization by colour Doppler of the hyaloid artery in persistent hyperplastic primary vitreous is not known. However, visualization of the artery within the hyperechoic hyaloid canal is pathognomonic of persistent hyperplastic primary vitreous and virtually excludes all other differential diagnoses. 3 We demonstrated the hyaloid artery in two out of three orbits with persistent hyperplastic primary vitreous.
To the best of our knowledge bilateral choroido-retinal thickening in persistent hyperplastic primary vitreous has not been reported previously.
Ultrasound is clearly useful for the diagnosis of persistent hyperplastic primary vitreous and is able to exclude other conditions presenting as congenital leucocoria; therefore, it is helpful for informing management pathways. The optimum time to perform the ultrasound scan is in early infancy. In general, the earlier the diagnosis the better the outcome. One study suggests that eyes undergoing surgery with a mean age of around 41 days achieve 6/60 or better vision. 10
The surgical treatment available is aimed at visual rehabilitation and includes lensectomy with or without vitrectomy and trabeculectomy. Normal vision is not usually obtained even after surgical corrections. Around half of the patients may have vision up to counting fingers or perception of light whereas one-third do not have perception of light and go for eventual enucleation. 10
In untreated or conservatively managed patients, around one-third of eyes have counting finger vision or light perception vision whereas, in almost half, the eyes have no perception of light and undergo enucleation. 10
Differential diagnoses for persistent hyperplastic primary vitreous include retinoblastoma, haemangioblastoma, Coat's disease, vitreoretinal dysplasia, vitreous haemorrhage and retinopathy of prematurity. 11 Differentiation from retinopathy of prematurity may be difficult on imaging. A history of prematurity, low birth weight and supplementation of oxygen may help to support a diagnosis of retinopathy of prematurity. 12 Complications of this condition include haemorrhage and glaucoma which usually result in enucleation.
In conclusion, in both cases of persistent hyperplastic primary vitreous, high frequency ultrasound provided the diagnosis and colour Doppler confirmed the presence of the hyaloid artery. Therefore, we suggest that it may be prudent to evaluate every patient presenting with congenital leucocoria with high frequency ultrasound and colour Doppler.
Declarations
Footnotes
Conflict of interest:
None.
Acknowledgements
None.