
Abstract
We report a patient who was known to have an abdominal aortic aneurysm and was being assessed for endovascular repair by calibrated angiogram, who developed back pain and cardiovascular collapse, where a computed tomography scan proved essential in establishing the correct diagnosis – bleed from an accessory renal artery branch.
Introduction
Following invasive arterial investigation, bleeding from the arterial access site and development of a retroperitoneal hematoma are recognized complications. There are, however, other causes for a retroperitoneal hemorrhage, particularly in patients with a known abdominal aortic aneurysm where rupture can be into the retroperitoneal tissues. We describe an interesting case where a computed tomography (CT) scan was helpful in establishing the diagnosis and formulating a management plan.
Case report
An 80-year-old woman with a known 4.8-cm infrarenal abdominal aortic aneurysm underwent a calibrated angiogram to assess her suitability for endovascular repair of the aneurysm. She had a significant past history of ischemic heart disease having had a coronary artery bypass graft 19 years earlier. Since that time, her coronary artery disease had progressed and 18 years later she underwent coronary angiography and coronary artery stenting with a drug-eluting stent. Thus, at the time of admission she was on dual antiplatelet treatment (aspirin and clopidogrel). The caliberated angiogram was performed in another hospital by percutaneous access to the right common femoral artery using a 6 French sheath. The procedure was described as straightforward. The arterial access was closed using an Angio-Seal closure devise (St Jude Medical, Zaventem, Belgium).
Within an hour of the completion of the procedure, the patient complained of severe right flank pain. This was associated with hypotension (systolic blood pressure of 90 mmHg). Suspecting a retroperitoneal bleed from the arterial access site, the surgeon arranged an urgent contrast-enhanced CT scan (Figure 1). The CT scan (non-contrast followed by arterial phase contrast-enhanced) report was of a large hematoma in the right perirenal space displacing and compressing the right kidney. The retroperitoneal hemorrhage extended adjacent to the right psoas muscle. There was a small (less than 1 cm) aneurysm of the main renal artery which looked intact. There was no evidence of hemorrhage about the iliac or femoral arteries. There was no evidence of abdominal aortic aneurysm rupture.
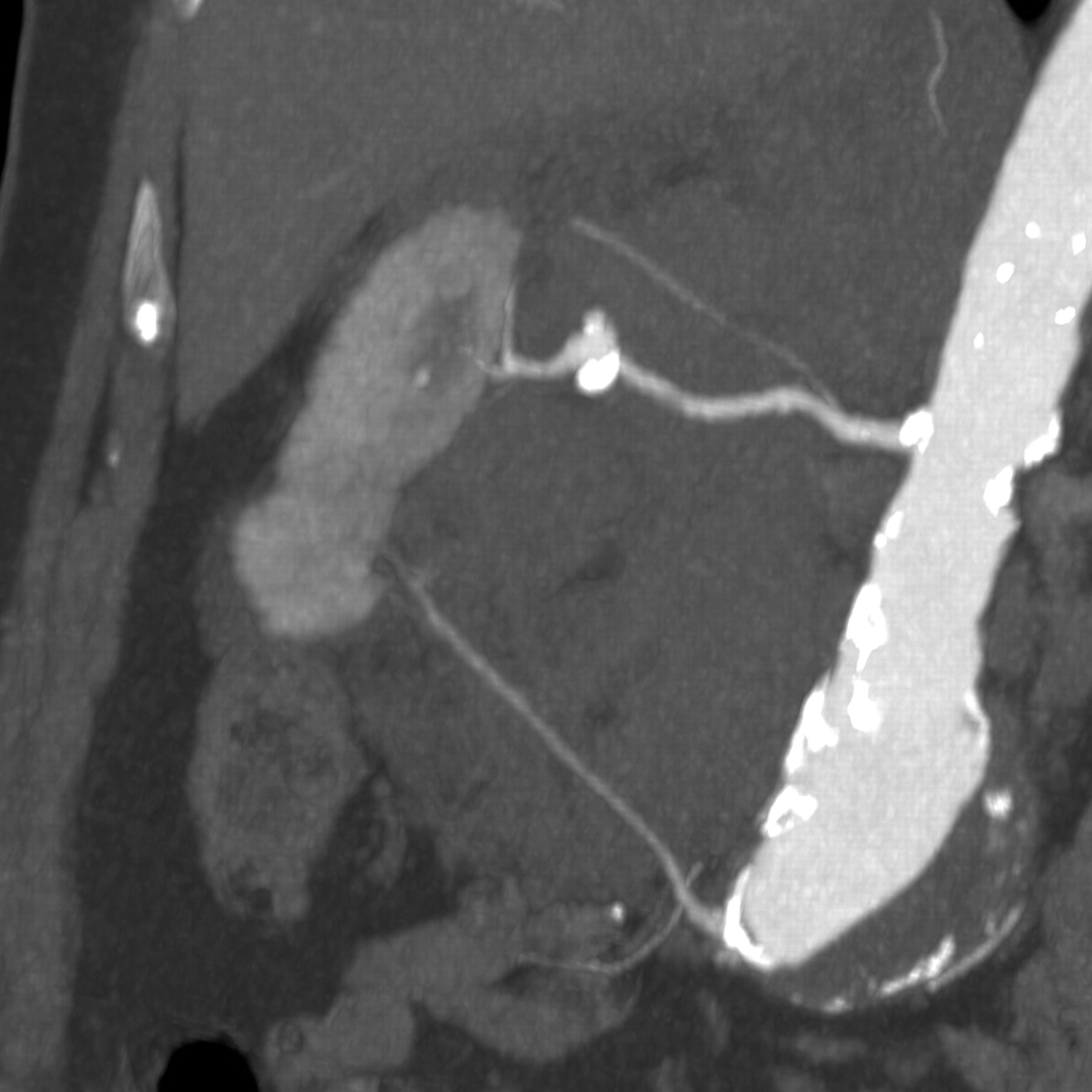
Maximum intensity projection reconstruction of the contrast-enhanced computed tomography scan showing an abdominal aortic aneurysm, a small aneurysm of the main right renal artery, the accessory renal artery to the lower pole of the right kidney and hematoma surrounding the right kidney
The patient was therefore transferred to our hospital for endovascular management of the bleed. Careful assessment of the contrast-enhanced CT scan revealed a small accessory right renal artery arising from the bifurcation of the abdominal aorta (Figures 1 and 2). This vessel supplied the lower pole of the right kidney and appeared to supply the area of the intra-renal hematoma.
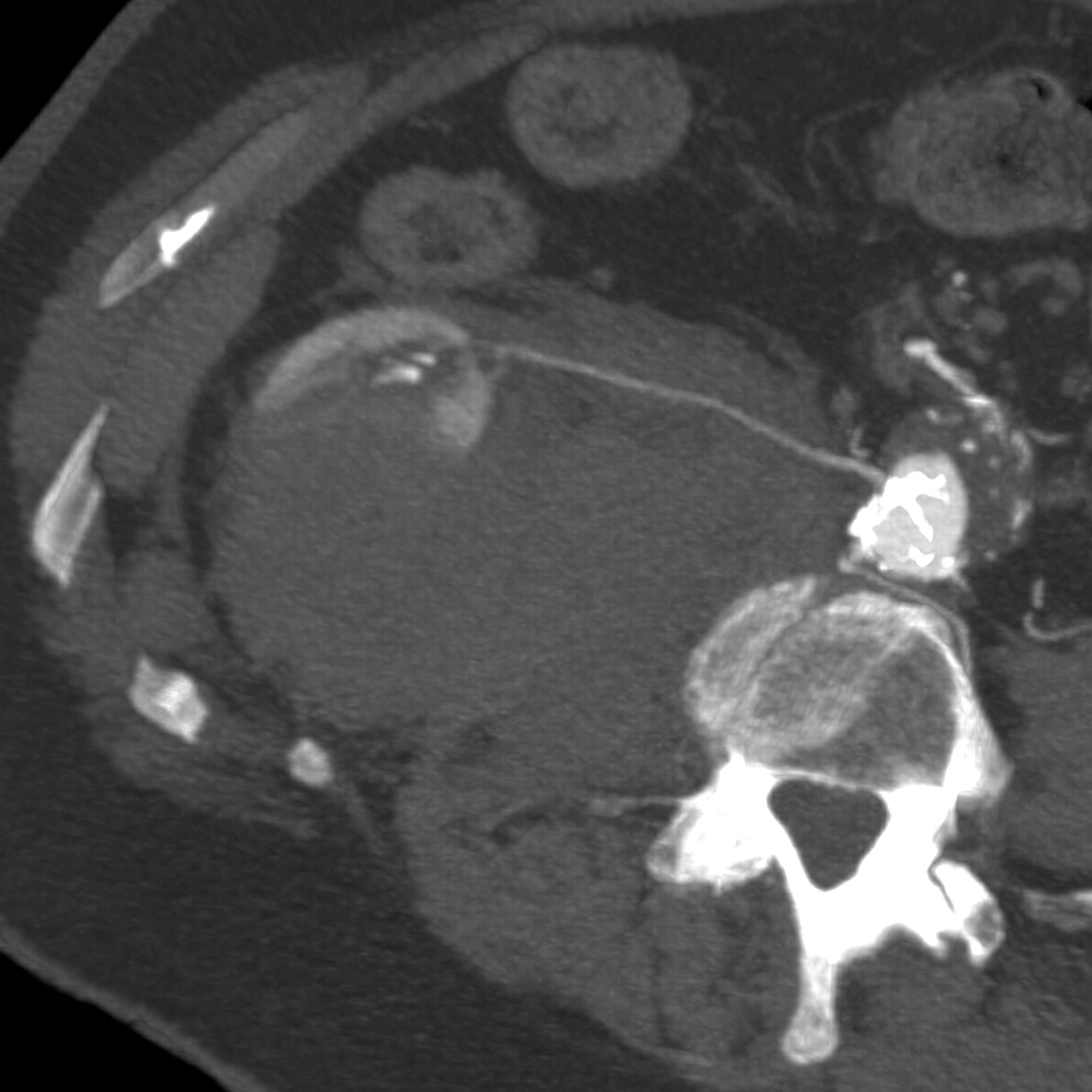
Maximum intensity projection reconstruction of the contrast-enhanced computed tomography scan showing the accessory right renal artery supplying the lower pole of the right kidney
Under local anesthetic, the right common femoral artery was again accessed percutaneously with a 6 French sheath. Diagnostic angiography was used to locate the origin of the accessory right renal artery. This vessel was selectively cannulated and selective angiography was performed. This confirmed the presence of extravasation from a branch of this vessel (Figure 3). The branch was selectively cannulated and a single, 2-mm complex, helical-fibered, platinum embolization coil (Target Vascular, Boston Scientific, Fremont, CA, USA) placed within the vessel. Completion angiography showed that there was no further extravasation (Figure 4). With crystalloid resuscitation, the patient's cardiovascular condition improved. Blood transfusion was not required.
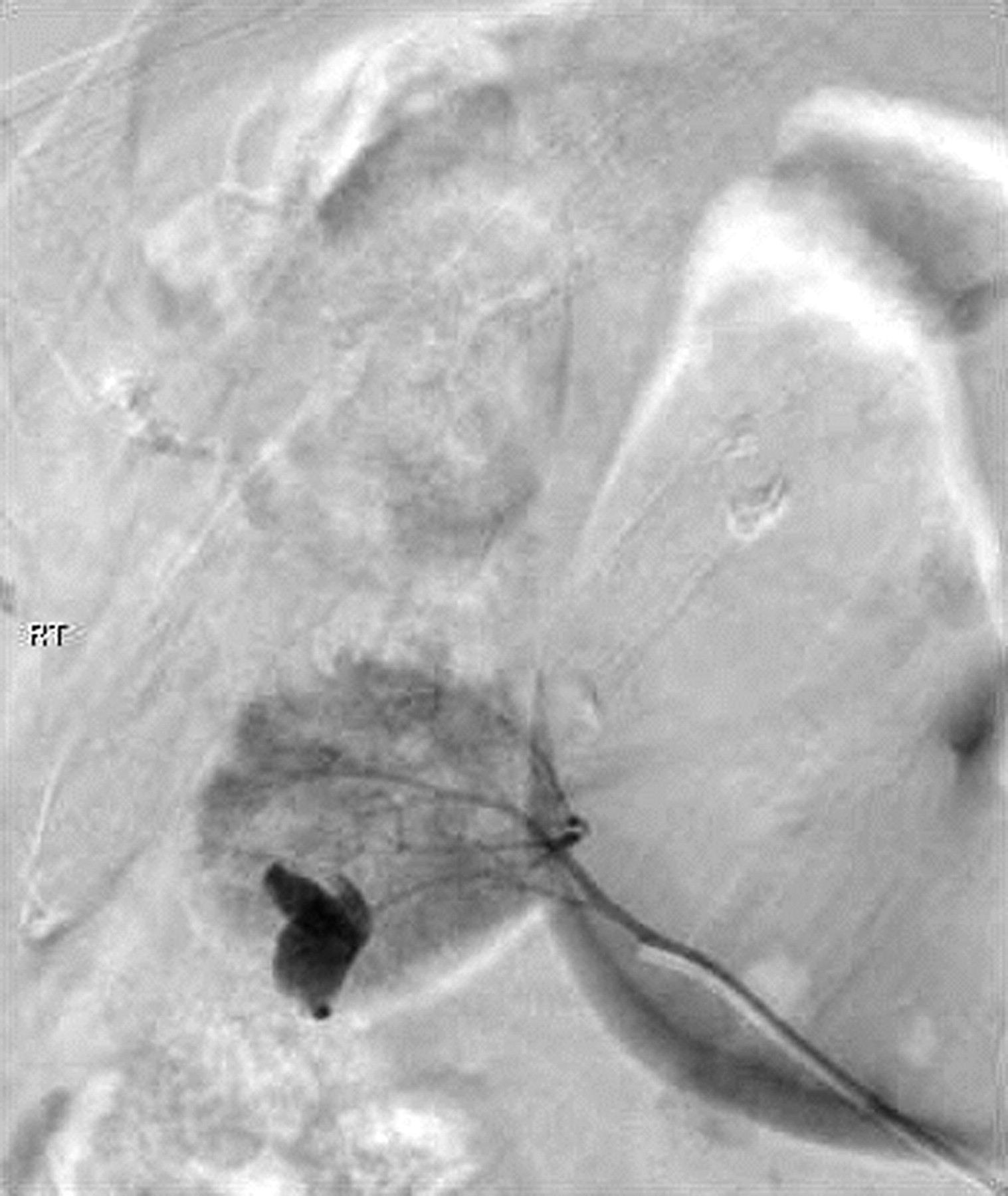
Selective angiogram showing extravasation from a branch of the accessory right renal artery
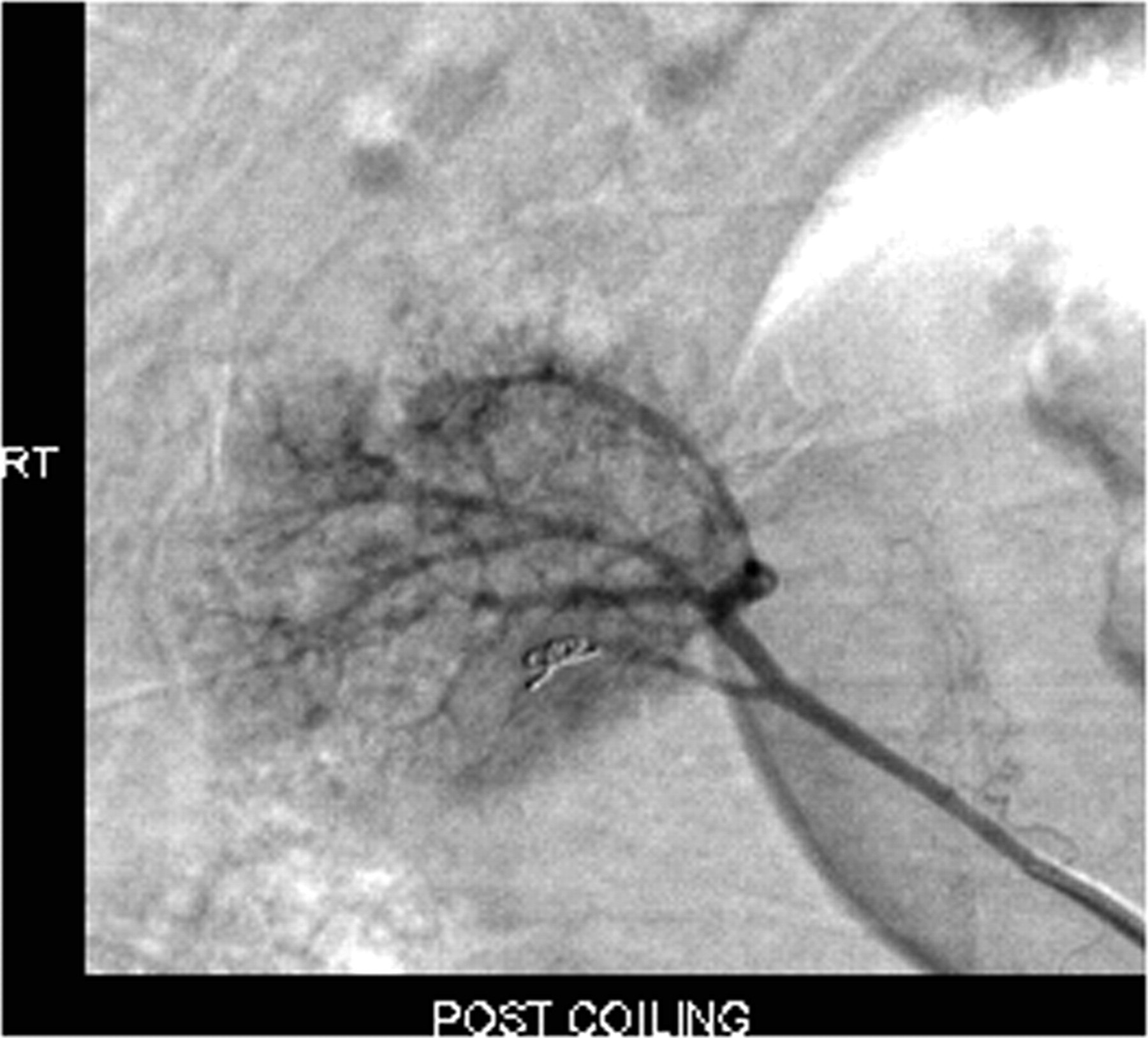
Completion angiogram showing no further contrast extravasation
Discussion
Onset of flank or iliac fossa pain following femoral arterial access should always raise the suspicion of retroperitoneal bleeding from the access site. Although conservative management of this is often successful, operative intervention or further endovascular intervention may be required to prevent further bleeding. Rupture of an abdominal aortic aneurysm can also cause retroperitoneal bleeding, even with small abdominal aortic aneurysms. In this case, these would be the two most likely diagnoses for the initial presentation. However, in this case, the CT scan showed an unexpected finding which radically altered management. The cause of the renal bleed remains unknown. A CT scan from two years ago showed no renal abnormality, and apart from the hemorrhage there was no renal abnormality on this occasion to explain a spontaneous bleed. Renal abnormalities such as polycystic kidney and tumors (including angiomyolipomas) are associated with spontaneous renal hemorrhage but there was no such evidence in this case. 1,2 Other reported causes of retroperitoneal hemorrhage arising from the kidney include polyarteritis nodosa. 3 Other causes of retroperitoneal hemorrhage include iatrogenic aortic injury, 4 anticoagulation and coagulation disorders, and 5–7 trauma to retroperitoneal vascular structures. 8,9
A potential cause for the bleed in this case could be accidental guidewire cannulation of the accessory renal artery and vascular trauma associated with this. This event was not reported by the operating surgeon.
This case highlights the usefulness of contrast-enhanced CT scans in the assessment of retroperitoneal hemorrhage.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.