
Abstract
The United States Pharmacopeia (USP) revised and renumbered the chapter describing sterile product preparation. Renumbering the document resulted in enforceable requirements for sterile preparation. This document, the infamous Chapter <797>, will improve sterile preparation in many institutions. The regulation change was a result of contaminated preparations following attempts to standardize sterile guidelines.
The process to understand, review, plan, and implement change and improvement in sterile preparation process is an initially vast, but ongoing task. The journey of USP <797> implementation at Oregon Health & Science University (OHSU) involved education, gap analysis, reorganization, and training. Sections of Chapter <797> posed particular challenges and issues in areas including environmental and equipment, product preparation, storage, and dating, as well as, personnel training and testing.
Financial implications of fully implementing the recommendations can be overwhelming. Regardless, institutions must start the process by working in their current environment, while maintaining focus on a vision of a fully compliant sterile product preparation system.
Sterile product preparation is an area of inconsistent compliance in pharmacy practice. Attempts to improve and standardize sterile product preparation have existed for years. In the early 1990s, serious medication errors, aseptic complications, and total parenteral nutrition (TPN) precipitation occurred. Some incidents resulted in patient injury and death, gaining the attention of the Food and Drug Administration (FDA).1–6 The FDA issued Warning Letters, Safety Alerts, and appealed to pharmaceutical organizations in an attempt to promote safe practices. Three pharmaceutical organizations responded: American Society of Health-Systems Pharmacy (ASHP) published Technical Assistance Bulletins, National Association of Boards of Pharmacy (NABP) published Standard Guidelines, and the United States Pharmacopeia (USP) published Guidelines.7–9 These publications varied but maintained a theme of safe preparation of sterile products. While the desire to prepare sterile products correctly was the goal, cost, space, and other issues prevented pharmacy practice from performing sterile product preparation according to recommendations. Despite these good intentions, the standardization of practice in sterile product preparation remained inconsistent and occasionally noncompliant.10–11
In January 2004, the USP revised and renumbered their existing chapter that described safe and sterile preparation of pharmaceuticals. Originally numbered <1206>, Pharmaceutical Compounding - Sterile Preparation was revised and categorized into Chapter <797>. 12 The USP chapter numbering system reflects the gravity of the standard. In essence, chapters numbering greater than 1,000 are recommendations, while chapter numbers under 1,000 are required and are usually FDA enforced. 13 The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) adopted Chapter <797> into its standards immediately. 14 ASHP and NABP were supportive of the change.
Adoption and implementation of the USP standards on sterile preparation will be difficult for many institutions. When the USP revised Chapter <797>, flexibility was designed into certain sections of the standards. The “grey areas” are intended to help each institution personalize, adapt, and comply with the intent of the chapter. 15
Examples of this can be found in the clean room description and basic categorization of low- and medium-risk level preparations. Also, JCAHO realizes timelines vary and creating a quality system that lasts is worth additional planning. As discussed at ASHP Midyear Clinical Meeting, JCAHO implementation expectations are more realistic 12 months following Chapter <797>'s release. See Table 1 for a sample timeline. 15
USP Chapter <797> and JCAHO's Timely Expectations 18
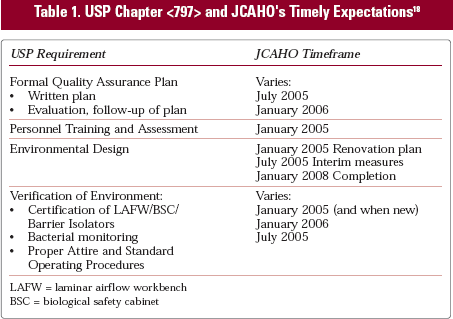
LAFW = laminar airflow workbench
BSC = biological safety cabinet
Materials and Methods
The purpose of this article is to describe the process our institution followed to assess its previous practice and to implement a plan to gain compliance in sterile product preparation. The intent is to provide assistance and insight for other institutions embarking on similar paths.
To begin, the following contains a summary of the sections of Chapter <797>, which have presented the greatest challenges for institutions in developing an implementation plan. Issues include product risk level categorization, environmental and equipment recommendations, and product dating and testing.
Risk Levels
Categorization of sterile products into levels of risk of contamination illustrates the intricacy of sterile preparation. The complexity of preparation and origin of components greatly influence potential for contamination. Chapter <797> categorizes sterile products into three risk levels: low, medium, and high. The levels of products prepared at an institution determine the scope of the sterile preparation plan. Low- and medium-risk products constitute the majority of preparations in most institutions. In these cases, components are initially sterile and this must be maintained throughout preparation. Low-risk products involve minimal manipulation of three or fewer sterile components. Medium-risk products differ in that they either involve intricate procedures, take longer to prepare, or involve more than three additives. High-risk products are composed of ingredient(s) that begin nonsterile, but sterility must be attained. See Table 2 for specific examples.
USP Chapter <797> Risk-Level Product Examples
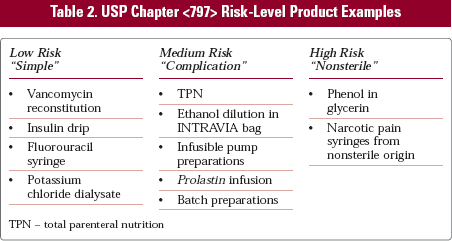
TPN – total parenteral nutrition
Environment and Equipment
Achieving air quality requirements set in Chapter <797> is the goal in designing a sterile preparation area. Controlling the preparation environment will decrease contamination potential. An International Organization for Standardization (ISO) Class 5 (Class 100) air quality for the primary preparation area is required. This is usually achieved by using a vertical flow biological safety cabinet (BSC) or horizontal laminar airflow workbench (LAFW). Ideally, this is placed in a buffer or clean room which has an ISO Class 7 (Class 10,000) air quality.16,17 High efficiency particulate air (HEPA) filters may or may not be needed in the rooms themselves in order to attain these air quality measurements. Access to sterile preparation areas should be limited. The USP description of these rooms is intentionally vague to allow flexibility. Common characteristics include: separation of sterile preparation area, creation of a positive pressure room, removal of paper and cardboard, minimal supplies, smooth room surfaces, easily cleanable (ideally stainless steel) carts and tables, and controlled traffic. The ante room, or the pre-sterile preparation area, should also be somewhat separate from the main pharmacy areas. Supplies, sink, garb, shelving, and tables are located here. Garb is required for sterile product preparation. It includes gown, mask, gloves, hat, and shoe covers. These are donned/removed in the ante area and worn in the preparation area at all times. 12 Barrier isolators are devices that create an “island of sterility” if located in an environment conducive to manufacturer's recommendations. 16 Inside, all necessary requirements for sterile preparation are provided. The operator remains outside and is not required to wear garb or be in a controlled area. External venting and air turnover rates are areas of discussion.18–21
It is worth noting that recent recommendations from National Institute for Occupational Safety and Health (NIOSH) indicate external-vented vertical flow LAFWs or BSCs, and negative pressure preparation areas may be required for preparation of hazardous drugs in the near future. 18
Beyond-Use Dating and Testing
Enemies of sterility are time and temperature. Increased temperature and extended storage dating will increase the potential for product contamination. Therefore, in Chapter <797>, the USP specifically designated maximum product dating and storage periods. Beyond-use dating recommendations, previously referred to as expiration dates, are provided for each risk level. The dating has been revised to include sterility factors relating to the length of time a sterile product is safe for administration. Drug stability data remain a component in determining dating and sterility aspects have been added. Table 2 contains a brief summary of the <797> recommendations. This product dating matrix may be prolonged, if sterility and pyrogen testing have been completed on the batch. High-risk products should be tested for sterility and pyrogenicity to ensure sterility was attained prior to dispensing. Chapter <797> only requires testing for route-dependant (central nervous or vascular system) high-risk products if prepared in groups greater than 25 single-dose, multidose vial intended for multiple patients or extended exposure period before sterilization. 12 In those cases, the dating in Table 3 may be waived and extended.
JCAHO's Storage Dating Recommendations 12
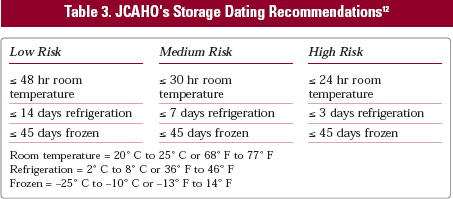
Room temperature = 20° C to 25° C or 68° F to 77° F
Refrigeration = 2° C to 8° C or 36° F to 46° F
Frozen = −25° C to −10° C or −13° F to 14° F
Background
Oregon Health & Science University Hospitals and Clinics (OHSU) is an expanding 454-bed teaching institution with a large research community. OHSU Department of Pharmacy Services has five pharmacy satellites that prepare sterile products (pediatric, operating room [OR], intensive care unit [ICU], research pharmacy services, and eye institute), a central pharmacy, and also staffs an oncology clinic—providing antineoplastic preparation services. The facility includes multiple on- and off-site clinics with the Department of Pharmacy Services providing pharmaceutical support to many of these locations. Personnel include full- and part-time employees. In recent years, a partial remodel created some sterile preparation environments that marginally complied with Chapter <797> in Central Pharmacy and the pediatric satellite.
Self -Education
Understanding Chapter <797> was essential in examining its impact on the department and institution as a whole. The standards can seem overwhelming, when viewed in total. Therefore, information was extracted and arranged into primary, usable categories. They were:
Environment
Equipment
Product
Personnel
Patient
Each category was then organized by:
Description or definition
Function
Education
Training
Quality assurance
The result was a practical and applicable report of Chapter <797>. Grouping this information by category was useful in creating a practical implementation plan and later in revising policies and procedures. For instance, descriptions of environment standards (LAFWs, buffer area or clean room area, ante room, barrier isolators) were combined with cleaning procedures (different needs for each area) and monitoring recommendations. As another example, products included risk level definitions and examples, verification procedures (accuracy, sterility, pyrogenicity), sterility testing, various standard operating procedures, storage, and beyond-use dating, and “after leaving the facility” quality control (handling, training, transportation, etc). This report was shared with pharmacy management to display the impact that Chapter <797> would have on OHSU. An upcoming JCAHO accreditation visit provided the catalyst to begin planning.
Gap Analysis
Following a thorough review and initial understanding of Chapter <797>, it became clear that a gap analysis of current procedures would be vital to the success of compliance with the chapter. A gap analysis is a report that diagrams where you are with where you want to be. Ideally, a bridge or multiple bridges, is designed to span from current practice to achieve the model practice, and the design process is often arduous. The gap analysis provided a stark appraisal of current practice—including a number of spreadsheets with extensive detail. Initially, an attempt was made to assess current practice and provide “the solution” simultaneously. This was not successful, due to the vast interrelationship of pharmacy processes both between satellites and Central Pharmacy and between sterile preparation and other pharmacy activities. In the second and successful attempt, each preparation area was visited multiple times (at different times of the day) for a detailed description of current facilities and practices. Spreadsheets were created for individual preparation areas. The process proved enlightening and valuable to both pharmacy managers and personnel working in the different areas.
The analysis was loosely based on the five sections mentioned earlier (product, environment, equipment, personnel, and patient). In order to stress the importance of the completed detailed analysis, these components are reiterated below both, as they were discovered before Chapter <797> implementation began and in the initial phases of implementation.
Results
Product
To determine the risk levels being produced, pharmacy prepared sterile products were categorized. Production was assessed as high-, medium-, and low-risk and tallied. Discussion with multiple practicing areas was completed to insure all production was included. Chapter <797> covers sterile product preparation regardless of who is involved or where the product is prepared. As the enormity of this task was realized, it was determined that initial implementation would focus on pharmacy prepared sterile products. Non-pharmacy (nursing, physician, respiratory therapist, etc.) prepared sterile preparation would be addressed at a later date. Assessment, education, and training would need intradepartmental support. Once compliant, the Pharmacy Department could be used as a model and education tool.
High Risk
High-risk product preparation incurs extra cost, quality assurance parameters, and training needs. As a result, institutions are attempting to eliminate or minimize high-risk production. A high-risk production spreadsheet was created to evaluate use at OHSU. Each row represented a high-risk compounded product. The column headings included:
Product name and non-sterile ingredient
Preparation Area, ISO 5 (LAFW)
Method of sterilization
Certificate of authenticity of bulk ingredient
Batch sizes (greater than 25 single dose/multidose for multiple patients)
Product sterility and pyrogen testing information (if any)
Current expiration dating of final product
Frequency of preparation, physician requesting, and use patterns
Alternative sterile products
OHSU's current facilities did not meet high-risk product preparation requirements. Since construction plans to improve the environment were not finalized, the high-risk product preparation list needed to be minimized. Physicians were contacted, products were eliminated, and alternatives recommended where possible. Once the list was minimized, outsourcing compounding pharmacies were contacted to contract production for the remaining items. High-risk preparations were difficult to outsource, as not all compounding pharmacies are able to meet Chapter <797> requirements. Additional factors, such as narcotic preparations with DEA paperwork further complicated the issue. Chapter <797> requires obtaining documentation regarding quality assurance and testing from the outsourcing agency since the final product is an extension of the pharmacy. An outsourcing organization was located and contract negotiations completed. The initial outsourced products were high-dose narcotic syringes.
Medium Risk
TPN production comprised the largest component of medium-risk preparation. Current software provided all quality assurance measurements desired and was being used. Few adjustments were necessary.
Low Risk
Low-risk preparation was ubiquitous. An ISO 5 environment (LAFW) was being used for sterile preparation and documentation of specific product preparation was deemed unnecessary. As stated earlier, analysis was limited to pharmacy prepared sterile production only.
Beyond-Use Dating
Chapter <797> specifically addressed product beyond-use dating. While facilities previously used stability data to develop the expiration dating guidelines; sterility issues were not addressed. Resources such as Trissel's Handbook on Injectable Drugs, the King Guide to Parenteral Admixture, and manufacturer package inserts were used primarily. Chapter <797> incorporated both stability and sterility. Sterility and pyrogen testing are required to extend dating beyond the recommendations.
At OHSU, it was determined that Chapter <797> beyond-use dating recommendations would be followed (see Table 2). Costs of testing did not justify extended dating benefit. To determine the products affected by the new dating, a report of assigned expiration dating was produced using the computer order-entry system. Internal product tables (eg, antineoplastic table) were reviewed, identifying a remarkable quantity of items requiring adjustment in beyond-use dating. Many were slight adjustments (14 days instead of 21) while others were dramatic (14 days instead of 3 months). The automated dispensing cabinet inventory was also reviewed. Shorter dating decreased the convenience and cost effectiveness of storing products in this manner. As a result, some products were removed from the automated dispensing cabinet.
High-risk products, which were outsourced, received independent beyond-use dating due to testing completed and documented by the outsourcing pharmacy. The dating provided by the contracted compounding pharmacy was maintained.
Testing
High-risk products prepared at OHSU in the future (not outsourced or eliminated) would need sterility and pyrogen testing. Information was compiled regarding testing options, and the resulting cost estimates were far above expectations. When a sterile product is initially tested for sterility and pyrogens, the formulation must be tested for an expanded panel of pyrogens to avoid cross contamination. As a result, 17 vials must be sent to verify the formulation is successful and can result in a sterile product. Once the formulation has cleared, only two vials need to be sent for sterility and pyrogen testing. The estimated cost (from two different facilities) was approximately $2,000. Product testing for a confirmed formulation estimated cost was approximately $450. As stated earlier, production of high-risk sterile products is costly.
Environment and Equipment
Assessment of OHSU's current sterile preparation environments was completed. A spreadsheet was created for each preparation area composed of approximately one row with multiple columns.
Columns included:
Risk level prepared, batching, antineoplastic products
Ante area and gown area
Clean room or buffer area and LAFW/BSC
Partitions and general layout
Floors and walls
HVAC, ceilings, and sprinklers
Air source and venting
Lights
Exterior doors
Fixtures (bins, shelving, electrical outlets, lock boxes, chairs, stools, floor mats)
Counters, islands, and cabinets
Sink, soap dispenser, hand sanitizer, and hand dryer
Garb selection and storage
Storage and supply status
Refrigerator
Automated compounding devices (TPN, repeater pumps)
Boxes, paper, and other lint-producing products
Cleaning procedures, garbage handling, and housekeeping schedules
Environment
The assessment revealed floors square-tiled with seams, uncovered walls, and foam-tiled ceilings. Fluorescent lighting and sprinklers were not sealed, and movable shelving counters and cabinets were everywhere. (Some sterile preparation areas contained carpeting and others had outside windows.) Chairs or stools were composed of plastic or fabric. Paper, posters, cardboard boxes, and personal items were present everywhere. In one area, a sink was in the clean room area, as well as, the ante room. Floor mats were made of porous foam material. Islands and preparation tables were made of particleboard with laminate surface.
In some satellites, the sterile preparation area was immediately adjacent to nonsterile preparation areas, computer terminals, printers, and texts. Partitions, where present, were not being used. They were erected years earlier in an attempt to follow previous recommendations. In some cases, pass-through doors were removed. Information obtained regarding current venting of BSCs was conflicting.
Cleanliness was assessed. The Housekeeping schedule consisted of daily light sweeping and weeky mopping. Garbage removal was completed daily, unless requested more frequently. Pharmacy personnel routinely cleaned the LAFWs and counter tops.
To bring these issues into compliance with Chapter <797>, practical changes, which could be made promptly with little financial implication, were addressed first. No additional square footage was available in the institution. Areas slated for construction and remodeling would be compared to an ideal ante room/clean room and planned.
In all areas, cardboard was removed, all signs were encased in plastic sleeves or laminated sheets, miscellaneous paper was removed, and required paper (formulations, tables) were encased in plastic. Attempts to partition a separate area for sterile preparation were completed, and doors were reat-tached to pass-through windows. A demarcation line was applied in satellites, where space was limited. LAFWs were moved to create separate preparation areas. Hooks were attached near the demarcation line to provide “ante area” for garb. Shelving units were purchased to replace movable shelving where possible. Stainless steel tables were purchased and placed in both ante and buffer room areas. The sink in the buffer room was designated “retired.” The housekeeping manager was contacted and new cleaning procedures discussed. Housekeeping personnel agreed to don garb appropriately and use the required cleaning supplies.
Equipment
OHSU currently has 12 LAFWs and four BSCs. New recommendations from the NIOSH state BSCs used for preparation of hazardous drugs should vent outside. 20 Appropriate venting was found in two of four BSCs. All LAFWs were certified every 6 months, as required.
As stated above, demarcation lines were applied to redirect traffic patterns in pharmacy satellites. LAFWs were then moved to provide maximum separation from nonsterile areas. Pumps and other equipment that were no longer used were removed.
Garb was being used for preparation of antineoplastic products only. Prior to the revisions of USP sterile product preparation recommendations, garb was not available in the Pharmacy and, therefore, not being used. Garb needed to be selected and a location for storage identified. Personnel satisfaction and compliance was dependant on product selection. The Surgical Department was consulted for samples and recommendations. Gloves, masks, and head and shoe coverings were readily available. Samples were obtained for personnel to assess. Gowns used in surgery would not meet Chapter <797> requirements due to their barrier properties; thus, washable gowns were pursued without success. The additional complication of pharmacy-only laundry requirements ended the search for reusable gowns.
Disposable gowns were easier to locate. Chapter <797> states gowns should be knee length and closed in front. 12 Cuffed wrists and collars are also recommended, while breathability was the most important feature desired from the staff. Two companies were selected and samples obtained. Personnel selected the final product. Two mask types and two styles of head coverings, from the surgery samples, were selected as well. Later, personnel were allowed to use washable, personalized, head coverings (again similar to surgery). Shoe covers were ordered.
By reorganizing the sterile product preparation areas, storage areas for garb were located. The OHSU Logistics Department currently stocked sterile preparation supplies daily, and arrangements were made for daily stocking of garb as well, requiring less storage space.
Automated compounding devices (ACDs) used were compliant with Chapter <797> standards. Successful practice revisions were made to improve preparation accuracy and efficiency. The ACD was located in a dedicated LAFW, with the ACD-dedicated computer and printer located outside the sterile preparation area. Accuracy assessments were completed throughout production and quality assurance reports were printed and reviewed daily. The ACD was calibrated and cleaned daily, and documentation was complete. Repeater pumps were used routinely for sterile compounding. Cleaning and calibration was completed daily and documented.
Personnel
Integral to all of these recommendations were the actions and the commitment of the personnel responsible for preparing these vital sterile medications. Chapter <797> specifically addresses personnel training and development. The new standards incorporate written and media-fill testing to confirm accurate aseptic technique and knowledge, updated preparation procedures (including “proper attire” mentioned above), and ongoing education and training. Personnel are ultimately responsible for producing a compounded sterile product. Standard Operating Procedures describe the entire process from order appropriateness to product preparation and delivery to patient, and all aspects involve pharmacy personnel. Personnel behavior and knowledge are essential to the success of Chapter <797> compliance.
Previous personnel education and training were evaluated. Sterile preparation personnel did not consistently receive didactic training, when initially hired or throughout their career. Training occurred only upon initial hiring and periodically a training video was observed. Most often, training occurred by working with experienced personnel. Aseptic technique was addressed, but the emphasis of training was on learning site-specific systems and workflow. A written exam was not used. Media-fill testing was not incorporated. Approximately half of the sterile preparation personnel were certified technicians and had received formal aseptic training. Some pharmacists received formal aseptic and sterile-product preparation didactic training in pharmacy school; although, few pharmacists were able to practice their technique in a laboratory environment. Overall, personnel received minimal didactic training in sterile-product preparation.
Initially, personnel at OHSU were not aware of the implications of Chapter <797>. To encourage personnel involvement in implementation of Chapter <797>, a Sterile Preparation Team was created. The team was composed of technicians and pharmacists who were directly involved in sterile preparation. They were given extensive background regarding the requirements of the new standards and encouraged to act as leaders in the training process. Personnel with experience at other facilities had seen variations in sterile preparation compliance and added valuable input. Regardless of experience, personnel were receptive and provided valuable insight throughout Chapter <797> implementation.
An extensive sterile product preparation training program was developed. All staff received an overview of the impact of Chapter <797> and completed aseptic training and testing. Training was divided into three sections: didactic, coaching, and testing. The didactic program incorporated practical training with sterile-preparation regulations and standards. The program began with a discussion-format presentation that included:
Explanation of Chapter <797> and impact on pharmacy practice
Aseptic technique review
Demonstration of aseptic technique
The program ended with questions and discussion. Over 12 sessions were scheduled to accommodate all shifts and employees. The training program was well-received, with discussion at the end of each session providing valuable information. This information was incorporated into current and future implementation and construction plans. A video was created to use for future training as well.
The coaching program involved one-on-one review of aseptic technique in a supportive non-threatening environment. Ideally, 1 week of coaching was completed prior to media-fill testing.
The testing section of training followed. Media-fill testing provided unbiased evaluation of aseptic technique. Media-fill testing kits were obtained, which tested low- and medium-risk product preparations. Personnel were given the media-fill test later in their work shift to mimic more stressful scenario, as suggested by Chapter <797> and the literature.12,22 Media bags were incubated at room temperature for 14 days, then visually evaluated. Successful technique was indicated by a clear solution. A cloudy solution indicated contamination and poor technique. Personnel who did not pass were given additional coaching then retested. All personnel passed after follow-up coaching and retesting.
A written exam was developed to evaluate knowledge and understanding of aseptic preparation and Chapter <797>. The exam was three pages long and composed of multiple-choice, true/false, and short answer questions. Questions involving actual site-specific scenarios proved valuable to evaluate sterile-preparation concepts.
Workflow in each sterile-preparation area was dramatically affected by Chapter <797> requirements. Issues arose throughout the gap analysis, but the personnel training process and workflow revealed the greater challenges. Separating sterile-preparation activities from the nonsterile pharmacy area required reorganizing personnel responsibilities. Garb requirements increased personnel time commitment in restricted areas. The delivery system, which previously used sterile-preparation technicians to routinely deliver medications, would no longer be able to provide prompt service. Various paperwork, textbooks, and numerous boxes were stored in many sterile preparation areas. Pharmacists routinely walked into preparation areas, checked products, then returned to nonsterile areas. Unnecessary nonsterile items were located in sterile preparation areas (sterile ready-to-use products, extra printers, extra pumps, etc).
Personnel were encouraged to contribute ideas throughout the transition process. It was decided that pass-through windows would be incorporated where possible, allowing the product to pass out of the clean room without the pharmacist removing garb. Recently, new software provided an item label and a production label for each sterile product. Preparation was streamlined, and safety measures increased by placing each product and its labels in separate plastic bins. Pharmacists checked each product by bin, confirming preparation accuracy against the production label. Ready-to-use products (frozens, premixes) were removed entirely from the clean room and labeled/checked in an adjacent area. Unnecessary traffic in the ante and clean room areas was decreased.
Technicians remained in the clean room to complete preparation sessions. If possible, one technician remained in the clean room at all times for stat orders. Stock was adjusted to accommodate needs for commonly prepared sterile products to avoid leaving the clean area. Ante room stock was also reorganized multiple times. Restocking in both areas occurred throughout the shift. Personnel outside the clean room obtained preparation components for specific orders. Upon leaving the clean room, technicians hung gowns in the ante area and discarded all other garb before leaving the ante area.
Personnel found garb cumbersome and uncomfortably warm. Room temperature was decreased to provide a more comfortable environment. Garb compliance in Central Pharmacy proved easier to maintain than in satellites. Satellite personnel had difficulty following garb requirements, because of delivery duties. Attempts were made to decrease delivery responsibility. Peer support was very important in maintaining garb compliance in the clean room.
Additional accommodations, including updating the delivery system and product turn around expectations, centralizing more sterile product preparation and increasing ready-to-use products will be addressed in the future. Workflow in Central Pharmacy and the satellites has been tracked and various algorithms were created to increase efficiency while maintaining compliance. Issues to be addressed include: technician movement into and out of sterile areas, pharmacist checking process, pass-through window efficiency, refrigerator location, general traffic patterns, communication issues (stat orders, scheduling personnel lunches and breaks, changes in order mid-sterile preparation, etc), stocking efficiently, wiping products when stocking, and use a production cart, and movement restrictions. Examination of these interconnected functions will be useful in designing the next phase of implementation.
Patient
Currently, patient monitoring and adverse event reporting are diligently completed at OHSU. Plans to continue emphasis in these areas, and expanded use of the new software, will increase monitoring capabilities and documentation.
Discussion
Implementation of Chapter <797> at any institution is a journey. While initial assessment and evaluation of current practice provides the starting point, Chapter <797> compliance provides the goal. The process of redesigning and incorporating change is unique to each facility. External factors such as space allocation, time constraints, and budgets greatly influence plans. The USP expects persistent diligence in achieving compliance with Chapter <797>. As discussed earlier, JCAHO will be evaluating compliance with Chapter <797> in a realistic yet rigorous format. Regardless, institutions must start the process by working in their current environment, while maintaining focus on a vision of a fully compliant, sterile-product preparation system.
The changes described in this article were considered “first phase.” Dramatic changes in environment will follow with dates yet to be determined. Additional space allocation is virtually nonexistent and reorganization of present square footage may be necessary. Although multiple clean-room designs have been entertained, the final decision will likely consist of a negative-pressure room for antineoplastic preparation, a positive-pressure room for all other sterile products, and a shared ante room. Permanent partitions will be installed. As discussed earlier, some high-risk preparation will eventually return as part of standard production, and it is desired to meet high-risk preparation standards. More rigorous training, testing, and monitoring programs will follow.
Due to the enormous financial implications of building a clean-room preparation area, it is likely that sterile-product preparation will be centralized. Barrier isolators have been discussed for use in areas outside the centralized-preparation area. Complications, such as air turnover rates and exterior venting needs for antineoplastic-product preparation, will increase the cost estimate of this option. The recent definition of “immediate use” in the USP revision has provided flexibility in sterile preparation, which may allow avoiding centralized-sterile production. 16 LAFWs may remain in satellite pharmacies to provide sterile products for immediate use in patient care areas.
Summary
USP Chapter <797> sterile-product preparation requirements and JCAHO support provides an opportunity for Pharmacy to meet the challenge and consistently prepare sterile products. Standards must be set and not compromised with patient safety as the ultimate goal. Financial investment, including personnel and space allotment, should be recognized by hospital administration as an opportunity to ensure patient safety and quality care.
Footnotes
Acknowledgements
The author acknowledges the input of Kate Farthing, Gae Ryan, and James Robbins. The thoughtful comments of Brad Fujisaki, Kristine Marcus, Michael Brownlee, and Kimberly McConnell are greatly appreciated.