
Abstract
Purpose
To characterize the inpatient use of filgrastim in cancer patients hospitalized for management of post-chemotherapy fever after receiving either outpatient filgrastim or pegfilgrastim.
Method
Retrospective review of chart records in a single-center, tertiary-care, teaching hospital and outpatient oncology center of cancer patients hospitalized for fever after outpatient chemotherapy and proactive administration of filgrastim or pegfilgrastim. Patients with the following tumor types were included: breast cancer, cervical cancer, colon cancer, Hodgkin disease, intermediate- or high-grade non-Hodgkin lymphoma, small cell or non-small cell lung cancer, and ovarian cancer.
Result
Billing data identified 1,438 outpatient chemotherapy patients treated with filgrastim or pegfilgrastim; 261 (18.2%) of whom were hospitalized for fever. All patients in the filgrastim groups, and 78% of those in the pegfilgrastim group, were given inpatient filgrastim. Duration of filgrastim administration in the inpatient setting was significantly shorter (P < 0.001) for the pegfilgrastim group.
Conclusions
Filgrastim was frequently administered to cancer patients hospitalized for fever, even after outpatient pegfilgrastim was administered as an adjunct to chemotherapy. Patients treated with once-per-cycle pegfilgrastim in an outpatient setting do not require filgrastim if they are hospitalized for fever before neutrophil recovery. Thus, hospitals could realize immediate cost savings by not treating those patients with filgrastim. This study illustrates the need to develop operational procedures in institutions to rapidly identify prior outpatient pegfilgrastim administration as a patient is admitted for post-chemotherapy fever.
Granulocyte colony-stimulating factors (G-CSFs), such as filgrastim (Neupogen) and pegfilgrastim (Neulasta), initiated in the first cycle of chemotherapy can reduce the severity and duration of neutropenia.4-6 In addition, when administered 24 hours after highly-myelosuppressive chemotherapy regimens, G-CSFs can reduce the incidence of febrile neutropenia by at least 50%.4-6 A recent study has shown that G-CSFs have a greater effect when they are used with moderately-myelosuppressive chemotherapy, defined as agents having a 17% risk of inducing febrile neutropenia; the all-cycle use of pegfilgrastim resulted in a relative risk reduction (RRR) of 94% in the incidence of febrile neutropenia and a 93% RRR in hospitalizations for febrile neutropenia compared to placebo. 7
Minimizing chemotherapy-induced neutropenia (CIN) with outpatient filgrastim requires daily injections. Although many cases are prevented, some patients develop fever and are hospitalized. In these cases, filgrastim is continued in the inpatient setting along with antibiotics until the neutrophil count has recovered. Pegfilgrastim, produced by covalently binding a linear 20-kDa polyethylene glycol molecule to the N-terminal of filgrastim, is eliminated primarily by neutrophil-mediated clearance.8,9 As a result, the levels of pegfilgrastim are sustained during periods of neutropenia, and the pegfilgrastim is eliminated as the neutrophil counts recover. 5 Thus, patients who are given pegfilgrastim in the outpatient setting should not require filgrastim if they are admitted to the hospital for febrile neutropenia (see Figure 1).
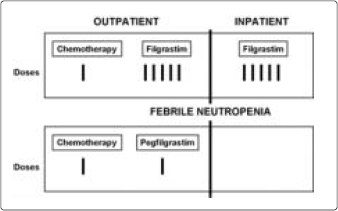
Potential effect of pegfilgrastim administered in the outpatient setting on the use of filgrastim in the inpatient setting.
The primary objective of this study was to characterize the use of inpatient filgrastim in cancer patients who are hospitalized for management of post-chemotherapy fever after receiving either outpatient filgrastim or pegfilgrastim.
Materials and Methods
This was a single-center retrospective chart review in an integrated hospital system. From the hospital's billing database, the records of chemotherapy patients who were treated with either outpatient filgrastim or pegfilgrastim were identified. The records of those patients who were hospitalized for any cause were then manually screened to find the cases in which fever was the cause for hospitalization.
We evaluated post-chemotherapy febrile (defined as temperature greater than 38°C at admission) hospitalizations in patients who received myelosuppressive chemotherapy followed by either outpatient filgrastim or pegfilgrastim support. Patients with the following tumor types were included: breast cancer, cervical cancer, colon cancer, Hodgkin disease, intermediate- or high-grade non-Hodgkin lymphoma, small cell or non–small cell lung cancer, and ovarian cancer. Patients were excluded if their treatment began outside the study identification period, if they were already participating in a filgrastim or pegfilgrastim study, or if they were pregnant or became pregnant during the study.
Two periods of interest were selected: before the availability of pegfilgrastim (January to December 2001) and after the availability of pegfilgrastim (January 2003 to June 2004). Pegfilgrastim was added to the formulary in January 2003; however, full use did not begin until May 2003. In order to capture sufficient pegfilgrastim use data, period two was extended to 18 months. Patients were included if they began and completed chemotherapy within these periods. The first period included only patients given filgrastim in an outpatient setting (Cohort 1). The second period included patients given either filgrastim (Cohort 2) or pegfilgrastim (Cohort 3) in the outpatient setting.
All patient charts were abstracted through the completion of the patients' last chemotherapy cycle before admission. Absolute neutrophil counts (ANC) were measured before the administration of G-CSF in the outpatient setting and on the first day of hospital admission. The severity of neutropenia was determined using the National Cancer Institute criteria.
Statistics
Nominal data were examined by chi-squared analysis using SPSS version 11 statistical software.
Results
Billing data identified 1,438 outpatient chemotherapy patients treated with filgrastim or pegfilgrastim, 261 (18.2%) of whom were hospitalized for fever. Of these, 209 were given filgrastim as an adjunct to chemotherapy—107 before the availability of pegfilgrastim (Cohort 1) and 102 after pegfilgrastim was available (Cohort 2). The remaining 52 patients were given pegfilgrastim as an adjunct to chemotherapy (Cohort 3). The demographic characteristics of the patients, tumor types, and chemotherapy class of agents are shown in Tables 1 and 2.
Patient Characteristics Among Cohorts
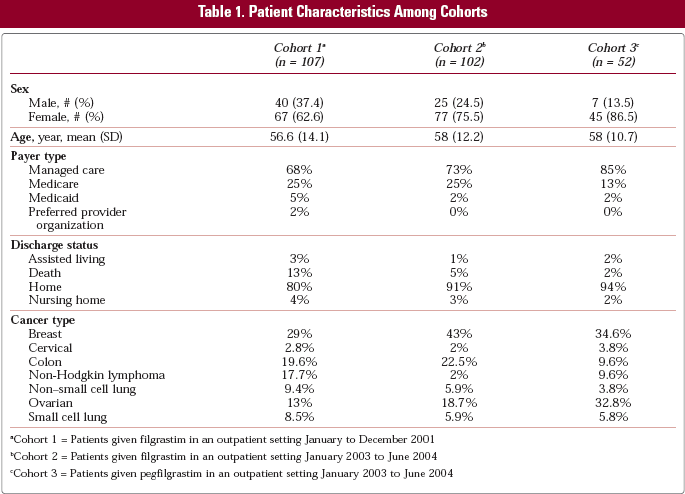
Cohort 1 = Patients given filgrastim in an outpatient setting January to December 2001
Cohort 2 = Patients given filgrastim in an outpatient setting January 2003 to June 2004
Cohort 3 = Patients given pegfilgrastim in an outpatient setting January 2003 to June 2004
Class of Chemotherapy Agent Used Among Cohorts
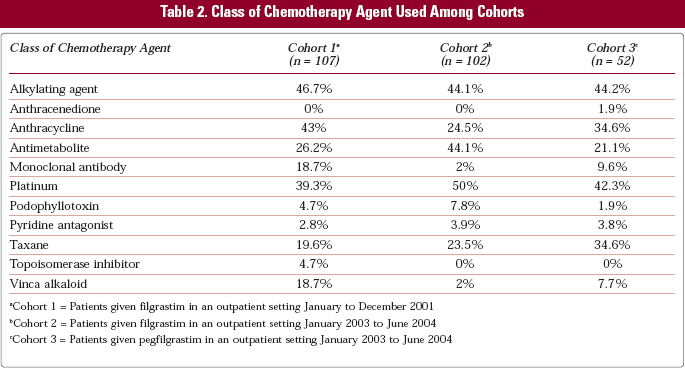
Cohort 1 = Patients given filgrastim in an outpatient setting January to December 2001
Cohort 2 = Patients given filgrastim in an outpatient setting January 2003 to June 2004
Cohort 3 = Patients given pegfilgrastim in an outpatient setting January 2003 to June 2004
In the outpatient setting, the number of G-CSF doses and the timing of G-CSF administration varied between Cohorts. Cohorts 1 and 2 received an average of 3.8 and 4.8 doses of outpatient filgrastim, respectively. Cohort 3 received a single injection of outpatient pegfilgrastim.
The timing of the administration of G-CSF relative to that of the chemotherapy improved during the study. In Cohorts 1 and 2, the initiation of filgrastim varied greatly, with growth factor initiated between 1 and 12 days after chemotherapy infusion. In Cohort 3, pegfilgrastim was given almost exclusively the day following chemotherapy infusion.
One hundred percent of patients in Cohorts 1 and 2 received inpatient filgrastim, while 78% of patients in Cohort 3 (patients receiving outpatient pegfilgrastim) were administered inpatient filgrastim (see Figure 2). All patients in Cohorts 1 and 2 received inpatient filgrastim for an average of 6.6 and 6.3 days respectively, whereas patients in Cohort 3 received inpatient filgrastim for an average of 2.3 days (P < 0.001).
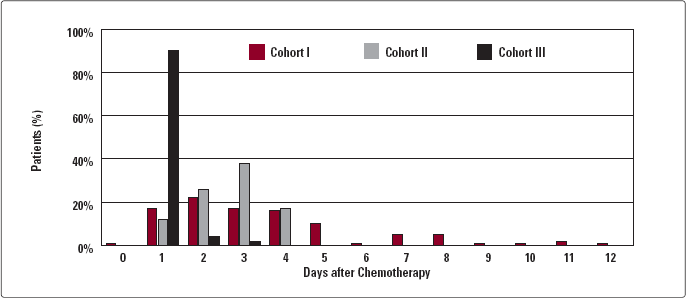
Outpatient G-CSF first dose administration following chemotherapy.
Discussion
The primary objective of this study was to review the use of inpatient filgrastim after outpatient treatment with either short-acting filgrastim or long-acting pegfilgrastim. Because of pegfilgrastim's neutrophil-mediated clearance, its serum concentrations remain high during periods of neutropenia, and the levels decline as the neutrophil count recovers.10,11 Therefore, patients treated with outpatient pegfilgrastim as an adjunct to myelosuppressive chemotherapy should not receive filgrastim if they are hospitalized for fever. In this study, however, inpatient filgrastim was given to as many as 78% of patients who had received outpatient pegfilgrastim, albeit for a shorter duration than those groups receiving filgrastim. Such inappropriate inpatient use of filgrastim after outpatient pegfilgrastim administration may increase the cost of cancer care. Conversely, hospitals may realize immediate cost savings by not administering filgrastim to inpatients who have received outpatient pegfilgrastim. Without access to the patient's outpatient records, the inpatient staff cannot determine whether the patient was given pegfilgrastim prior to hospitalization. Better coordination of care, using a combined inpatient-outpatient medical records system, which may be electronic, may help overcome this problem. This finding highlights the need for better communication, medication reconciliation, and coordination of care.
In addition to the inpatient G-CSF variation noted above, outpatient G-CSF use varied compared to current recommendations. According to the prescribing information for pegfilgrastim and filgrastim, therapy with G-CSFs should be initiated 24 hours after chemotherapy infusion. 12 In Cohorts 1 and 2 of this study, the timing of outpatient filgrastim administration after chemotherapy infusion was more erratic, with filgrastim being initiated mostly between days 1 and 3. Patients administered outpatient pegfilgrastim following chemotherapy infusion were most likely to receive their dose 24 hours after chemotherapy infusion.
Conclusion
This study highlights the need to develop operational procedures for institutions to identify outpatient administration of pegfilgrastim in patients admitted to the hospital for fever and febrile neutropenia. This will ensure that following administration of outpatient pegfilgrastim, inpatient filgrastim can be eliminated. Our institution is currently in the process of developing a mechanism to identify outpatient pegfilgrastim administration prior to admission. Prospective trials in larger patient populations are needed to better quantify the use of filgrastim among febrile inpatients.
Footnotes
Aknowledgements
The Saint Barnabas Health Care System received an educational grant from Amgen Inc.