The increasing complexity of cancer chemotherapy heightens the requirement that pharmacists be familiar with these highly toxic agents. This column will review various issues related to preparation, dispensing, and administration of cancer chemotherapy. It will also serve as a review of various agents, both commercially available and investigational, used to treat malignant diseases.
Drug Name: Nelarabine
Synonyms: 506U78, GW506U78, Arranon
Mechanism of Action
Nelarabine is the water-soluble prodrug of 9-beta-D-arabinofuranosylguanine (Ara-G), a deoxyguanosine analogue. Nelarabine is demethylated by adenosine deaminase to Ara-G, which is transported into leukemic blast cells by nucleoside transporters and mono-phosphorylated by nucleoside kinase. Ara-G is phosphorylated to arabinosylguanine triphosphate (Ara-GTP), the active 5'-triphosphate, by deoxyguanosine kinase and deoxycytidine kinase. Ara-GTP is incorporated into the DNA of T-cell lymphoblasts and lymphocytes, leading to inhibition of DNA synthesis and cell death.
Pharmacokinetics
Nelarabine and Ara-G are rapidly eliminated from plasma with half-lives of approximately 30 minutes and 3 hours, respectively, after a 1,500 mg/m2 dose in adult patients. Peak plasma levels of Ara-G typically occur at the end of nelarabine infusions and are usually higher than peak plasma nelarabine levels, suggesting rapid and extensive conversion of nelarabine to Ara-G. Mean plasma nelarabine and Ara-G peak levels were 5 mcg/mL and 31.4 mcg/mL, respectively, after a 1,500 mg/m2 IV infusion over 2 hours in adult patients; the Ara-G AUC was 37 times higher than that of nelarabine. After the same dose, a mean intracellular peak level of Ara-GTP occurred between 3 and 25 hours. The intracellular Ara-GTP AUC was 532 times higher than that for nelarabine and 14 times higher than that for Ara-G. Intracellular Ara-GTP elimination half-life cannot be accurately measured because of the prolonged intracellular Ara-GTP levels. Mean clearance of nelarabine is 30% higher in pediatric than adult patients with values of 259 L/h/m2 and 197 L/h/m2, respectively. The apparent clearance of Ara-G is comparable, with values of 10.5 L/h/m2 for adult patients and 11.3 L/h/m2 for pediatric patients. Both nelarabine and Ara-G are extensively distributed in the body, with steady state volumes of distribution (Vd) of 197 L/m2 and 213 L/m2 for nelarabine in adult and pediatric patients, respectively, and steady state apparent Vd of 50 L/m2 and 33 L/m2 for Ara-G in adult and pediatric patients, respectively. Neither nelarabine nor Ara-G is substantially bound to plasma proteins (less than 25% in vitro). Nelarabine is metabolized by adenosine deaminase-mediated O-demethylation to Ara-G, which is hydrolyzed to guanine. Some nelarabine is hydrolyzed to methylguanine, which is O-demethylated to guanine. Guanine is N-deaminated to xanthine. Nelarabine and Ara-G are partially eliminated by the kidneys, with mean urinary excretion of 6.6% and 27% of the administered dose, respectively, over 24 hours in adult patients. Renal clearance averaged 24 L/h and 6.2 L/h for nelarabine and Ara-G, respectively, in adult patients.
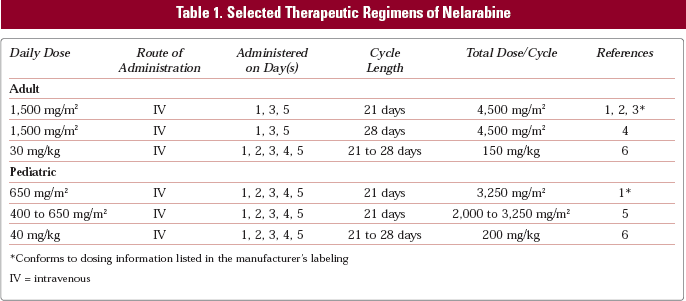
Selected therapeutic regimens of nelarabine appear in Table 1.
Conforms to dosing information listed in the manufacturer's labeling
IV = intravenous
Preparation
Nelarabine is prepared without dilution by transferring the dose into an empty, sterile glass or polyvinyl chloride (PVC) container.
Stability
Nelarabine is stable at room temperature in glass or PVC containers for up to 8 hours after dispensing.
Administration
Nelarabine is administered as a 1 or 2-hour infusion.
Toxicities
Cardiovascular:
Adult: Chest pain (grade 1 or 2) 5%; hypotension (grade 1 or 2) 6%, (grade 3 or 4) 2%; sinus tachycardia (grade 1 or 2) 7%, (grade 3 or 4) 1%.
Endocrine/Metabolic
Pediatric: Hypocalcemia (grade 1 or 2) 6%, (grade 3 or 4) 2%; hypokalemia (grade 1 or 2) 5%, (grade 3 or 4) 6%; hypoglycemia (grade 1 or 2) 2%, (grade 3 or 4) 4%; hypomagnesemia (grade 1 or 2) 4%, (grade 3 or 4) 2%; malaise/fatigue (grade 1 or 2) 18%, (grade 3 or 4) 6%.
Adult: Anorexia (grade 1 or 2) 9%; dehydration (grade 1 or 2) 3%, (grade 3 or 4) 4%; edema (grade 1 or 2) 26%; fatigue (grade 1 or 2) 38%, (grade 3 or 4) 12%; hyperglycemia (grade 1 or 2) 5%, (grade 3 or 4) 1%; pyrexia (grade 1 or 2) 18%, (grade 3 or 4) 5%; rigors (grade 1 or 2) 8%.
Gastrointestinal
Pediatric: Vomiting (grade 1 or 2) 10%.
Adult: Abdominal distension (grade 1 or 2) 6%; abdominal pain (grade 1 or 2) 8%, (grade 3 or 4) 1%; constipation (grade 1 or 2) 20%, (grade 3 or 4) 1%; diarrhea (grade 1 or 2) 21%, (grade 3 or 4) 1%; nausea (grade 1 or 2) 41%; stomatitis (grade 1 or 2) 7%, (grade 3 or 4) 1%; vomiting (grade 1 or 2) 21%, (grade 3 or 4) 1%.
Hematologic
Pediatric: Anemia (grade 1 or 2) 40%, (grade 3 or 4) 55%; leukopenia (grade 1 or 2) 17%, (grade 3 or 4) 21%; neutropenia (grade 1 or 2) 15%, (grade 3 or 4) 79%; thrombocytopenia (grade 1 or 2) 29%, (grade 3 or 4) 59%.
Adult: Anemia (grade 1 or 2) 65%, (grade 3 or 4) 34%; febrile neutropenia (grade 1 or 2) 2%, (grade 3 or 4) 10%; neutropenia (grade 1 or 2) 18%, (grade 3 or 4) 63%; petechiae (grade 1 or 2) 10%, (grade 3 or 4) 2%; thrombocytopenia (grade 1 or 2) 27%, (grade 3 or 4) 59%.
Hepatic
Pediatric: Hypoalbuminemia (grade 1 or 2) 4%, (grade 3 or 4) 6%; hyperbilirubinemia (grade 1 or 2) 1%, (grade 3 or 4) 9%; transaminase elevations (grade 1 or 2) 8%, (grade 3 or 4) 4%.
Adult: AST elevations (grade 1 or 2) 4%, (grade 3 or 4) 2%.
Infection
Pediatric: (grade 1 or 2) 2%, (grade 3 or 4) 3%.
Adult: (grade 1 or 2) 6%, (grade 3 or 4) 3%; pneumonia (grade 1 or 2) 3%, (grade 3 or 4) 5%; sinusitis (grade 1 or 2) 6%, (grade 3 or 4) 1%.
Neurologic
Pediatric: Asthenia (grade 1 or 2) 5%, (grade 3 or 4) 1%; ataxia (grade 1 or 2) 1% to 3%, (grade 3 or 4) 1% to 3%; convulsions (grade 3 or 4) 3%; grand mal convulsions (grade 3 or 4) 1%; headache (grade 1 or 2) 6% to 10%, (grade 3 or 4) 3% to 6%; hypoesthesia (grade 1 or 2) 2% to 3%, (grade 3 or 4) 3% to 4%; motor dysfunction (grade 1 or 2) 2%, (grade 3 or 4) 1%; muscle atrophy/weakness/tiredness (grade 3 or 4) 6%; nervous system disorder (grade 1 or 2) 3%; neuropathy (grade 1 or 2) 3%, (grade 3 or 4) 3%; paresthesias (grade 1 or 2) 2%, (grade 3 or 4) 1%; peripheral neuropathy (grade 1 or 2) 4%, (grade 3 or 4) 2%; peripheral motor neuropathy (grade 1 or 2) 1%, (grade 3 or 4) 2%; peripheral sensory neuropathy (grade 3 or 4) 6%; somnolence (grade 1 or 2) 5% to 23%, (grade 3 or 4) 2% to 3%; status epilepticus (grade 3 or 4) 1%; tremor (grade 1 or 2) 3%.
Adult: Abnormal reflexes (grade 1 or 2) 2%, (grade 3 or 4) 2%; amnesia (grade 1 or 2) 3%; arthralgia (grade 1 or 2) 8%, (grade 3 or 4) 1%; asthenia (grade 1 or 2) 16%, (grade 3 or 4) 1%; ataxia (grade 1 or 2) 5% to 7%, (grade 3 or 4) 2% to 3%; balance disorder (grade 1 or 2) 2%; confusion (grade 1 or 2) 6% to 15%, (grade 3 or 4) 2% to 7%; depressed level of consciousness (grade 1 or 2) 5%, (grade 3 or 4) 1%; depression (grade 1 or 2) 5%, (grade 3 or 4) 1%; dizziness (grade 1 or 2) 22%; dysgeusia (grade 1 or 2) 3%; encephalopathy (grade 3 or 4) 2%; gait disorder (grade 1 or 2) 6% to 8%, (grade 3 or 4) 12%; headache (grade 1 or 2) 14%, (grade 3 or 4) 1%; hypoesthesia (grade 1 or 2) 10% to 15%, (grade 3 or 4) 2% to 5%; insomnia (grade 1 or 2) 7%; malaise/fatigue (grade 1 or 2) 48%, (grade 3 or 4) 15%; motor dysfunction (grade 1 or 2) 6%, (grade 3 or 4) 2%; muscle atrophy/weakness/tiredness (grade 1 or 2) 3% to 7%, (grade 3 or 4) 5%; myalgias (grade 1 or 2) 12%, (grade 3 or 4) 1%; neurologic disorders (grade 1 or 2) 2%, (grade 3 or 4) 2%; neuromuscular disorders (grade 1 or 2) 2%, (grade 3 or 4) 2%; neuropathy (grade 1 or 2) 4%, (grade 3 or 4) 7%; paralysis (grade 3 or 4) 2%; paresthesias (grade 1 or 2) 5% to 15%, (grade 3 or 4) 2%; peripheral neuropathy (grade 1 or 2) 4%, (grade 3 or 4) 1%; peripheral motor neuropathy (grade 1 or 2) 6%, (grade 3 or 4) 1%; peripheral sensory neuropathy (grade 1 or 2) 13%; sensory loss (grade 1 or 2) 2%; somnolence (grade 1 or 2) 23% to 46%, (grade 3 or 4) 3%; tremor (grade 1 or 2) 5%.
Renal
Pediatric: serum creatinine elevation (grade 1 or 2) 6%.
Respiratory
Adult: Cough (grade 1 or 2) 25%; dyspnea (grade 1 or 2) 14%, (grade 3 or 4) 6%; dyspnea on exertion (grade 1 or 2) 7%; epistaxis (grade 1 or 2) 8%; pleural effusion (grade 1 or 2) 4%, (grade 3 or 4) 6%; wheezing (grade 1 or 2) 5%.
Raf kinase activates the Raf/MEK/ERK pathway, a signaling cascade that mediates cellular proliferation, differentiation, and transformation. Sorafenib inhibits Raf kinase and thus reduces deregulated proliferation of malignant cells. Sorafenib also inhibits the vascular endothelial growth factor (VEGF) receptors, VEGFR-2 and VEGFR-3, which are involved in tumor progression and angiogenesis.
Pharmacokinetics
Mean relative bioavailability of orally administered sorafenib tablets is 38% to 49% in the fasting state, with peak levels reached in about 3 hours. When given with a high-fat meal, sorafenib absorption is reduced by 29% compared to the fasting state. Mean elimination half-life is 25 to 48 hours. Multiple dosing for 7 days can produce a 2.5- to 7-fold accumulation compared to single-dose administration. Steady state plasma levels are achieved within 7 days, with a peak-to-trough ratio of mean concentrations of less than 2. Mean Cmax and AUC increase less than proportionately when a dose of greater than 400 mg twice a day is given. In vitro, sorafenib is 99.5% bound to human plasma proteins. Metabolism is primarily by the liver through CYP3A4-mediated oxidation and UGT1A9-mediated glucuronidation. The pyridine N-oxide metabolite has in vitro potency similar to that of sorafenib. Following a 100 mg oral dose, 96% of the dose was recovered within 14 days, with 77% excreted in feces and 19% in urine as glucuronidated metabolite. Unchanged sorafenib accounted for 51% of excretion, all in the feces.
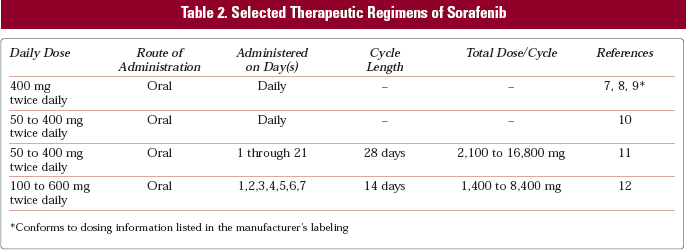
Selected therapeutic regimens of sorafenib appear in Table 2.
Conforms to dosing information listed in the manufacturer's labeling
Administration
Sorafenib is administered orally twice daily on an empty stomach (1 hour before or 2 hours after eating).
Toxicities
Cardiovascular: Hypertension (grade 1 or 2) 14%, (grade 3 or 4) 3% to 24%.
Constitutional: Fatigue (grade 1 or 2) 32% to 51%, (grade 3 or 4) 5% to 6%; weight loss (grade 1 or 2) 10%.
Dermatologic: Alopecia (grade 1 or 2) 13% to 27%, (grade 3) 3%; dry skin (grade 1 or 2) 11%; hand-foot skin reaction (grade 1 or 2) 18% to 48%, (grade 3 or 4) 6% to 13%; pruritis (grade 1 or 2) 19%; other skin reactions (grade 1) 7%; rash (grade 1 or 2) 26% to 62%; rash/desquamation (grade 1 or 2) 40%.
Gastrointestinal: Anorexia (grade 1 or 2) 16% to 42%; bilirubin (grade 3) 4%; constipation (grade 1 or 2) 15%; diarrhea (grade 1 or 2) 41% to 47%, (grade 3) 2% to 9%; nausea (grade 1 or 2) 23% to 30%; pancreatitis (grade 3) 4%; stomatitis (grade 1 or 2) 7%; vomiting (grade 1 or 2) 16%.
Hematologic: Hemorrhage – all sites (grade 1 or 2) 13%, (grade 3) 2%.
Neurologic: Sensory neuropathy (grade 1 or 2) 13%.
Pain: Abdomen (grade 1 or 2) 9%, (grade 3) 2%; headache (grade 1 or 2) 10%; joint (grade 1 or 2) 8%, (grade 3) 2%.
References
1.
Arranon [package insert].Research Triangle Park, NC: GlaxoSmithKline; 2005.
2.
DeAngeloD.J., YuD., DodgeR.K.. A phase II study of 2-amino-9-beta-D-arabinosyl-6-methoxy-9H-purine (506U78) in patients with relapsed or refractory T-lineage acute lymphoblastic leukemia or lymphoblastic lymphoma: CALGB study 19801 [abstract 743]. Blood.2003; 100(Suppl 1): 198a.
3.
GoekbugetN., ArnoldR., JohannesA.. Compound GW506U78 has high single-drug activity and good feasibility in heavily pretreated relapsed T-lymphoblastic leukemia (T-ALL) and T-lymphoblastic lymphoma (T-LBL) and offers the option for cure with stem cell transplantation (SCT) [abstract 150]. Blood.2005; 106.
4.
ThompsonM.A., ProB., SarrisA.. Results of a phase II study of 506U78 (nelarabine) in refractory indolent B-cell or peripheral T-cell lymphoma [abstract 2681]. Blood.2005; 106.
5.
BergS.L., BlaneyS.M., DevidasM.. Phase II study of nelarabine (compound 506U78) in children and young adults with refractory T-cell malignancies: a report from the Children's Oncology Group. J Clin Oncol.2005; 23: 3376–3382.
6.
KurtzbergJ., ErnstT.J., KeatingM.J.. Phase I study of 506U78 administered on a consecutive 5-day schedule in children and adults with refractory hematologic malignancies. J Clin Oncol.2005; 23: 3396–3403.
RatainM.J., EisenT., StadlerW.M.. Final findings from a phase II, placebo-controlled, randomized discontinuation trial (RDT) of sorafenib (BAY 43-9006) in patients with advanced renal cell carcinoma (RCC) [abstract 4544]. Proc Am Soc Clin Oncol.2005; 24.
9.
EscudierB., SzczylikC., EisenT.. Randomized phase III trial of the Raf kinase and VEGFR inhibitor sorafenib (BAY 43-9006) in patients with advanced renal cell carcinoma (RCC). Proc Am Soc Clin Oncol [abstract 4510]. 2005; 24. (abstr 4510).
10.
StrumbergD., RichlyH., HilgerR.A.. Phase I clinical and pharmacokinetics study of the novel Raf kinase and vascular endothelial growth factor receptor inhibitor BAY 43-9006 in patients with advanced refractory solid tumors. J Clin Oncol.2005; 23: 965–972.
11.
AwadaA., HendliszA., GilT.. Phase I safety and pharmacokinetics of BAY 43-9006 administered for 21 days on/7 days off in patients with advanced, refractory solid tumors. Br J Cancer.2005; 92: 1855–1861.
12.
ClarkJ.W., EderJ.P., RyanD., LathiaC., LenzH.J.Safety and pharmacokinetics of the dual action Raf kinase and vascular endothelial growth factor receptor inhibitor, BAY 43-9006, in patients with advanced, refractory solid tumors. Clin Cancer Res.2005; 11: 5472–5480.