
Abstract

One of the 2005 National Patient Safety Goals set by the Joint Commission of Accreditation of Healthcare Organizations required institutions to standardize and limit the number of drug concentrations available in order to prevent medication errors. All institutions must implement this standard by 2008. This paper describes the development of standard concentrations at the Monroe Carell Jr. Children's Hospital at Vanderbilt and the implementation of the standards using our computerized provider order entry system (CPOE).
Background
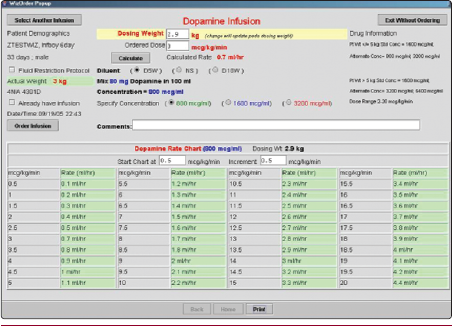
When computerized provider order entry was implemented in our pediatric critical care unit in 2001, screens were created to assist the prescriber in ordering medications administered as continuous infusions (Figure 1). These screens were also later utilized in our neonatal intensive care unit when CPOE was implemented in the unit in 2003. These ordering screens provided information such as dosing recommendations and concentration limits. The program utilized the patient's weight, the desired dose, and the desired rate to calculate the concentration of the drug to be prepared. The prescriber also had the option of entering a desired concentration and the rate would then be calculated for them. This feature would be used by prescribers if the patient was fluid restricted and the prescriber wished to order the most concentrated formulation possible. Though not utilizing the “rule of six,” this system had a similar limitation that resulted in a multitude of possible concentrations and lacked standardization.

Ordering screen for dopamine prior to standardization
In other areas of our institution where CPOE was not yet in place, including the operating rooms, patient transport vehicles and during cardiac resuscitation, the “rule of six” method was used to determine the concentration needed to administer medications by continuous infusion.
Development of Standard Concentrations
As a starting place for selecting standard concentrations, we relied on data from our existing CPOE system. Data on all continuous infusions that were prepared by the pharmacy during the previous one-year period was reviewed. Information such as the most common concentrations ordered, the most common dosing range, and the largest and smallest patients to whom the drug was administered was collected. Spreadsheets on which all the data could be applied and tested were then developed.
The most common concentrations ordered were selected as possible standard concentrations. If a medication was commercially available as a prepared dilution, this concentration was also considered as a possible standard concentration. Spreadsheets were created for each possible standard concentration. Each spreadsheet calculated the infusion rate that resulted from escalating the dose through the most common dosing range in patients ranging in weight from 0.5 kg to 50 kg.
One of the concerns surrounding conversion to standardized concentrations for infusions was retaining the ability to titrate doses. Because our former CPOE order screens allowed the prescriber to request the dose and rate of the infusion, titration was rarely a problem. To insure that ease of titration would not be lost, the change in the infusion rate that resulted from escalating the dose through the normal dose range was reviewed. This also allowed us to determine that all of the needed doses were measurable at the given concentration.
Another concern involved with using standardized concentrations was the volume of fluid that would be delivered to the patient. Using our former CPOE order screens, a small rate could be requested to provide a needed dose. The concentration of the medication would be adjusted automatically so that the dose could be given at the requested rate. Because only the dose and not the rate can be requested using standardized concentrations, there was a concern that standardized concentrations would increase the fluid volume delivered to the patient. To insure that the fluid delivered to the patient was appropriate, the infusion rate was calculated for many doses within the normal dosing range for patients of varying weights.
After all possible concentrations were tested in the spreadsheets for ease of titration, ability to measure the dose accurately, and fluid volume delivered to the patient, the most appropriate concentrations were selected. Standard concentrations were selected for 38 drugs administered by continuous infusion.
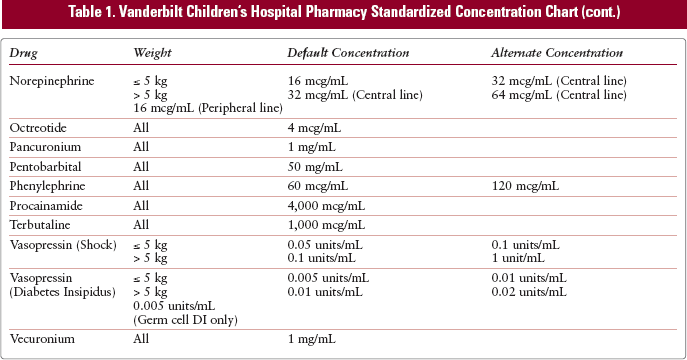
Because of the wide range of weights seen in a pediatric population, it was necessary to choose different standard concentrations for two weight groups for some medications. The two weight groups used were less than or equal to 5 kg and greater than 5 kg. An additional weight group of less than 1.5 kg was also necessary for one drug commonly used in the extremely low birth weight population. For each weight group, the concentration that seemed most appropriate for all weights within the group was selected as the default concentration. An alternate concentration was selected for some drugs when the option of a more concentrated dilution was needed. These concentrations are typically used in fluid-restricted patients. It was also necessary to select more dilute concentrations for drugs that are commonly used in the neonatal population because of the inability to deliver very small doses with concentrated dilutions. Sixteen drugs were assigned only one standard concentration for patients of all weights. The remaining 22 drugs were assigned a default concentration and one or two alternate concentrations. (Table 1).
Vanderbilt Children's Hospital Pharmacy Standardized Concentration Chart (cont.)
All of the concentrations selected were reviewed and accepted by physicians practicing in each unit. Physician involvement was encouraged throughout the selection process. Feedback from physicians and nurses was helpful in choosing standard concentrations that would clinically meet the needs of patients of many various weights and reduce the possibility for errors.
Prior to implementation of standardized concentrations, the choice of possible diluents was also reexamined. In the past, requests were often made for nonstandard diluents including various concentrations of dextrose and sodium. If the diluent and medication were compatible, the pharmacy would honor the request and dilute medications in 5%, 10%, 12.5%, 15%, 17.5%, or 20% dextrose. Additionally, medications were diluted in normal saline as well as 1/4 or 1/2 normal saline if requested and compatibility allowed. Medications were often requested with these diluents when it was felt that it was clinically necessary for the patient. For example, patients who need maximum calories may need medications diluted in 20% dextrose or patients who are sodium restricted would require 1/4 normal saline. This practice increased the time to prepare each medication and contributed to lack of standardization between patients and increased potential for errors during the preparation process.
To decrease preparation time and further standardize medications given by infusion, diluents were limited to only 5% dextrose, 10% dextrose, and normal saline. To insure that this was clinically appropriate, the actual amount of dextrose or sodium that was delivered to the patient by the diluent in a continuous infusion was examined. In all cases examined, the change in dextrose or sodium delivered to the patient would be negligible if standard diluents were used. Physicians practicing in all units of the institution where continuous infusions are used agreed that there was a lack of clinical difference provided by diluting medications in nonstandard versus standard diluents.
Implementation of Standardized Concentrations
Modifications to the existing CPOE ordering screen were necessary prior to implementation of standardized concentrations. The information displayed on the ordering screen is now automatically customized based upon the patient's weight, the patient's location, and the medication being ordered. The ordering screens were modified so that the prescriber can enter only the desired dose. The default concentration is automatically selected when the order is initiated, but the prescriber has the option to choose an alternate concentration if desired. The concentration options that appear on the screen are also based upon the patient's weight. For example, if dopamine is ordered in a patient less than 5 kg, the concentration options on the screen are 800 mcg/mL, 1,600 mcg/mL and 3,200 mcg/mL (Figure 3). If the patient is greater than 5 kg, the options that are presented to the prescriber are 1,600 mcg/mL, 3,200 mcg/mL and 6,400 mcg/mL (Figure 4). The prescriber is also given possible diluent options. Only those diluent options for which appropriate stability data are available for a particular drug appear on the screen. The rate at which the medication must be infused is calculated and displayed. This order is then sent electronically to the pharmacy computer system via CPOE interface. The pharmacist is given all the necessary information including drug, dose, concentration, rate, and diluent in the order. The computer also calculates the volume to be sent based upon whether the drug is stable for 24 hours or a longer period. This information, as well as how much drug should be added to that volume in order to achieve the desired concentration, is included in the order that is transmitted to the pharmacy.
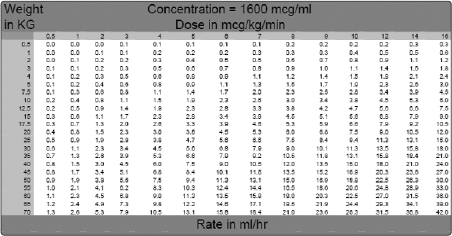
Sample spreadsheet for dopamine
Post-implementation CPOE ordering screen for dopamine in patient less than or equal to 5 kg
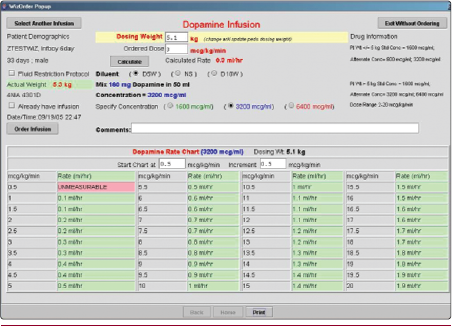
Post-implementation CPOE ordering screen for dopamine in patients greater than 5 kg
When a dose is modified for a continuous infusion, the prescriber is presented with a screen that shows the concentration that is currently being administered to the patient as well as a table of doses and corresponding rates (Figure 5). If the prescriber wishes to change concentrations, a new order must be entered for the patient. The nurse also has the ability to select the order in the CPOE system and obtain a printable rate chart to keep at the patient's bedside.
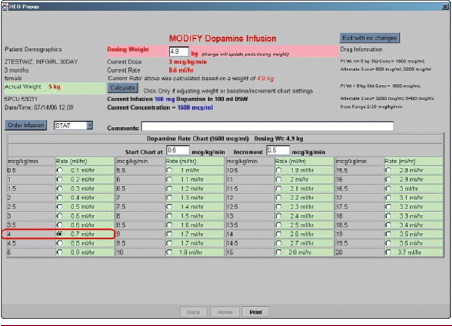
Ordering screen used for modifying dose of continuous infusion
All physicians, nurses, and residents were informed of the conversion to standardized concentrations prior to actual implementation. The prescribers were already familiar with the current CPOE order screens; thus, only minimal education was necessary to make them aware of changes that were made. Conversion to standardized concentrations took place over four days. The update to the CPOE system was made on the first day, after which time only the standardized concentrations could be ordered. Over the following three days, all existing orders for nonstandard concentrations were converted to standardized concentrations.
Conclusion
The use of standardized concentrations for medications given by continuous infusion was successfully implemented at our institution in December of 2004. Special ordering screens in our CPOE system that limit the prescriber to only the standardized concentrations have helped to enforce our new policy. Standard concentrations were also implemented in areas such as emergency transport vehicles and the operating room. This practice has been well accepted by members of the health care team and has allowed us to eliminate the practice of nonstandardized concentrations and meet JCAHO standards.