
Abstract
The increasing complexity of cancer chemotherapy now requires that pharmacists be familiar with these highly toxic agents. This column will review various issues related to preparation, dispensing, and administration of cancer chemotherapy, and review various agents, both commercially available and investigational, used to treat malignant diseases.
Mechanism of Action
Ixabepilone is the first of a new group of antineoplastic agents called epothilones to be approved for clinical use. The drug suppresses the dynamic instability of alpha beta-II and alpha beta-III microtubules by binding to the beta-tubulin subunit of the microtubule. This stabilizes microtubular function, arresting the cell cycle in the G2/M phase and inducing apoptosis.
Pharmacokinetics
The maximum concentration (Cmax) following a single intravenous (IV) dose of ixabepilone 40 mg/m2 is 252 ng/mL. Ixabepilone is about 67% to 77% bound to plasma proteins and has a large (greater than 1,000 L/m2) volume of distribution (Vd). The drug is extensively metabolized by the liver, primarily by CYP3A4, into at least 30 inactive metabolites. The drug is not an inhibitor of CYP3A4, CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP2D6, nor an inducer of CYP1A2, CYP2B6, CYP2C9, or CYP3A4. Ixabepilone is excreted primarily (65%) in the feces with approximately 1.6% of the dose eliminated as unchanged drug. About 21% of a dose is excreted renally and 6% is as unchanged drug. Ixabepilone has an elimination half-life (T½) of about 52 hours.
Selected therapeutic regimens of ixabepilone appear in Table 1.
Selected Therapeutic Regimens of Ixabepilone a
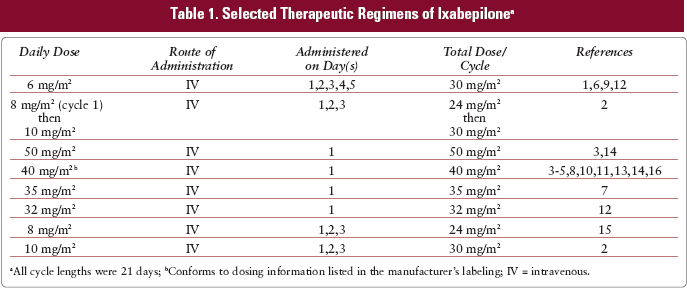
All cycle lengths were 21 days;
Conforms to dosing information listed in the manufacturer's labeling; IV = intravenous.
Preparation
The drug and diluent should be allowed to reach room temperature prior to reconstitution. The diluent may contain a white precipitate, which should dissolve when the solution reaches room temperature. Ixabepilone must be reconstituted to a concentration of 2 mg/mL with the provided diluent prior to dilution for infusion. This ixabepilone solution is further diluted in Ringer's lactate to a final concentration of 0.2 to 0.6 mg/mL (250 or 500 mL for most patients). The drug should be dispensed in a glass, polypropylene, or polyolefin (non-diethylhexyl phthalate) container.
Stability
Reconstituted vials are stable for 1 hour at room temperature; solutions diluted in Ringer's lactate for infusion are stable for 6 hours at room temperature.
Administration
Ixabepilone is administered as an IV infusion, usually over 3 hours.
Ixabepilone should be administered through a 0.22 micron filter using a polyethylene-lined (non-sorbing) infusion set.
Drug Interactions
Ixabepilone is a substrate of CYP3A4; therefore, inducers of CYP3A4 may decrease the effects of the drug, while CYP3A4 inhibiters may increase its effect. Due to limited experience with the drug, with the exception of ketoconazole, these interactions are based on theoretical considerations of the drugs' mechanisms of action rather than documented clinical cases.
Toxicities
Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
Recommended Reviews
Cortes J, Baselga J. Targeting the microtubules in breast cancer beyond taxanes: the epothilones. Oncologist. 2007;12(3):271-280.
Pivot X, Dufresne A, Villanueva C. Efficacy and safety of ixabepilone, a novel epothilone analogue. Clin Breast Cancer. 2007(7);7:543-549.
Mechanism of Action
Nilotinib is a selective tyrosine kinase inhibitor that targets BCR-ABL kinase, c-KIT and platelet derived growth factor receptor (PDGFR). Nilotinib inhibits BCR-ABL-mediated proliferation by connecting to the adenosine triphosphate (ATP)-binding site of BCR-ABL and inhibiting tyrosine kinase activity. Nilotinib is active against BCR-ABL kinase mutations but lacks activity against SRC enzymes.
Pharmacokinetics
Following oral administration, the Cmax is about 3 hours. Nilotinib is highly (about 98%) bound to plasma proteins. The peak concentration and area under the time curve (AUC) increase is about 112% and 82% if nilotinib is given after a high-fat meal. The drug is metabolized in the liver by oxidation and hydroxylation via CYP3A4 to primarily inactive metabolites. The elimination T1/2 of nilotinib is about 15 to 17 hours. Excretion is primarily fecal (93%, 69% as unchanged drug). Selected therapeutic regimens of nilotinib appear in Table 2.
Selected Therapeutic Regimens of Nilotinib
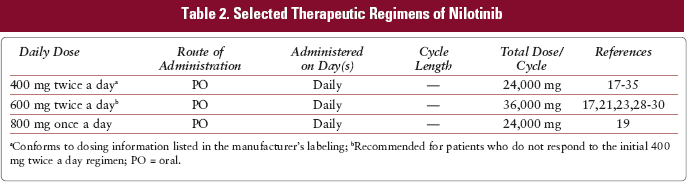
Conforms to dosing information listed in the manufacturer's labeling;
Recommended for patients who do not respond to the initial 400 mg twice a day regimen; PO = oral.
Availability
Nilotinib is available as 200 mg capsules.
Administration
Nilotinib is given orally, preferably on an empty stomach (1 hour before or 2 hours after a meal).
Interactions
Nilotinib is a substrate of CYP3A4 and p-glycoprotein; therefore inducers of CYP3A4 or p-glycoprotein may decrease the effects of the drug, while CYP3A4 or p-glycoprotein inhibitors may increase its effect. Nilotinib is an inducer of CYP2C8, 2C9, and 2D6 and may decrease the effect of drugs which are substrates of these isoenzymes.
Toxicities
Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
Recommended Reviews
Piccaluga PP, Paolini S, Martinelli G. Tyrosine kinase inhibitors for the treatment of Philadelphia chromosome-positive adult acute lymphoblastic leukemia. Cancer. 2007;110(6):1178-1186.
Weisberg E, Manley P, Mestan J, Cowan-Jacob S, Ray A, Griffin JD. AMN107 (nilotinib): a novel and selective inhibitor of BCR-ABL. Br J Cancer. 2006;94(12):1765-1769.